 2016, Vol. 37
2016, Vol. 37文章信息
- 朱陈, 王乐, 杜灵彬, 李静, 张娟, 代敏, 石菊芳 .
- Zhu Chen, Wang Le, Du Lingbin, Li Jing, Zhang Juan, Dai Min, Shi Jufang .
- 乳腺X线摄影技术应用于人群筛查准确性的Meta分析
- The accuracy of mammography screening for breast cancer: a Meta-analysis
- 中华流行病学杂志, 2016, 37(9): 1296-1305
- CHINESE JOURNAL OF EPIDEMIOLOGY, 2016, 37(9): 1296-1305
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2016.09.022
-
文章历史
收稿日期: 2016-05-04




2. 310022 杭州, 浙江省肿瘤医院, 放射科;
3. 100021 北京, 国家癌症中心/中国医学科学院北京协和医学院肿瘤医院, 城市癌症早诊早治项目办公室;
4. 100021 北京, 国家癌症中心/中国医学科学院北京协和医学院肿瘤医院, 影像诊断科
2. Radiology Department, Zhejiang Cancer Center, Zhejiang Cancer Hospital, Hangzhou 310022, China;
3. Program Office for Cancer Screening in Urban China, National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100021, China;
4. Diagnostic Imaging Department, National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100021, China
乳腺癌是全世界女性最常见的恶性肿瘤,据国际癌症研究署GLOBOCAN2012估计,全球每年乳腺癌新发病例167.1万,死亡52.2万[1]。乳腺癌是一种发展相对缓慢的恶性肿瘤,从原位癌发展成浸润性乳腺癌需要约6.3年[2]。目前仍缺乏有效的预防措施,因此乳腺癌筛查应作为乳腺癌预防的重点[3]。乳腺X线摄影(Mammography)是一种传统且被广泛应用的乳腺影像学检查方法,乳腺X线摄影可以检出临床触诊阴性的早期乳腺癌,是迄今为止唯一已被证实可以降低乳腺癌死亡率的筛查方法[4]。WHO国际癌症研究机构(WHO/IARC)推荐对50~69岁的女性开展有组织的定期乳腺X线摄影筛查[3]。
自1963年美国最早开展乳腺X线摄影筛查至今,西方国家进行了大量关于乳腺X线应用于一般人群乳腺癌筛查准确性的研究。但是,由于存在筛查对象个体变异(年龄、乳腺密度、基因突变、激素治疗)、不同的乳腺X线摄影技术(专用屏-片摄影/全视野数字乳腺X线摄影)、摄影方位(单位片/双位片)、阅片方式(单人/双人/CAD辅助诊断)以及阅片者经验等诸多因素的异质性,乳腺X线摄影技术的准确性在不同研究中存在差异。
20世纪,Mushlin等[5]首次对乳腺X线摄影技术筛查准确性进行了Meta分析,但仅纳入6项研究,且未对灵敏度和特异度进行定量合成。2002年WHO/IARC在对全球范围内乳腺癌不同筛查方案的有效性和准确性进行了系统梳理和评估,报告指出乳腺X线摄影筛查乳腺癌的灵敏度为68%~92%,特异度为82%~98%[6]。2000年以后,全球乳腺癌筛查项目不断增加,因此对乳腺X线摄影技术准确度的评价也亟需更新。为此,笔者通过系统收集和整理探讨乳腺X线摄影技术对乳腺癌筛查准确度的研究,并在此基础上进行汇总分析,客观、准确地评价乳腺X线摄影技术的筛查效果,为以后乳腺癌筛查技术的选择提供合理的参考依据。
资料与方法1. 文献检索:以外文电子数据库Medline、Embase、Cochrane和中国学术期刊网全文数据库(CNKI)为信息源,检索与基于人群的乳腺X线筛查准确性有关的国内外文献。检索日期从1980年1月1日至2015年6月4日,检索式整合疾病名称、筛查干预、结果指标等系列检索词。英文检索式以“Breast Neoplasms” “Mass screening” “Early diagnosis” “Mammography”为MeSH主题词,并与“Breast Cancer”“Screen*”“Early Detection” “Mammographic”“Mammogram*” “Sensitivity” “Specificity” “Negative rate” “Positive rate” “Predictive value” “Predictive values” “Diagnostic accuracy” “Diagnostic performance”自由词组合,限定文献语种为英语,研究对象为人类,文献类型非快报、评论、综述、采访、荟萃分析及出版物。中文检索式以 “乳腺癌” “乳腺肿瘤” “普查” “筛查” “早期诊断”“早诊早治” “钼靶” “乳腺X线” “灵敏度” “特异度”为主题词进行检索。此外,手动检索与主题相关的系统综述及研究的参考文献,作为电子检索的补充。
通过阅读标题和摘要对检索到的文献进行初筛,对选出的文献进行全文阅读,由两人依据严格的纳入和排除标准独立进行文献复筛,如出现异议,由第三人判读,直至达成一致结果。
2. 纳入和排除标准:纳入标准:①乳腺X线筛查准确性的原创性研究;②基于人群,研究类型可为前瞻性或回顾性;③乳腺癌诊断标准明确(活检、手术或随访结果);④可从文章中摘录或计算出真阳性、假阳性、假阴性、真阴性的例数。排除标准:①研究对象有乳腺疾病相关症状的报告;②研究对象有既往乳腺癌或癌前病变病史;③诊断性X线摄影;④计算机辅助诊断技术(CAD)准确性;⑤综述和病例报告;⑥仅对于灵敏度和特异度进行估计的文章;⑦样本量<500;⑧研究对象重叠时保留样本量较大的研究。
3. 数据提取及质量评价:由两名工作人员按照预先制定的数据采集表独立提取数据,若出现不一致时,由第三名专业人员进行判断。提取的数据包括四个部分:①文献特征提取数据,包括第一作者、文献发表年份、期刊名称等;②筛查方案信息提取数据,包括研究地点、筛查时间、研究对象年龄、样本量、金标准;③研究结果信息提取数据,包括真阳性、假阳性、假阴性、真阴性的例数;④备注。如出现四格表数据不完整的情况,则通过联系作者获得数据,或根据文献中报导的灵敏度、特异度、阳性预测值等指标推算。4项研究中假阳性和真阴性的例数通过特异度和阳性预测值估算得到[7-10],1项研究中四格表例数由总样本量乘以率估算得到[11]。
本研究采用QUADAS(Quality Assessment of Diagnostic Accuracy Studies)量表对文献质量进行评价。QUADAS是由英国约克大学2003年制定的专用于系统评价中评价诊断准确性试验质量的工具[12],是目前唯一经过严格评价和验证的诊断准确性试验质量评价标准[13]。该量表共14个条目,涵盖疾病谱、选择标准、金标准、疾病进展偏倚、部分参照偏倚、多重参照偏倚、混合偏倚、待评价试验的实施、金标准的实施、试验解读偏倚、金标准解读偏倚、临床解读偏倚、难以解释的试验结果和退出病例,每一条目采用“是”“否”“不清楚”评价。采用百分比堆积条形图分析每一条目下纳入研究评定为“是”“否”或“不清楚”的比例。
4. 统计学分析:采用的软件为Stata 12.1。本研究用来描述X线摄影技术准确度的指标主要包括SROC曲线下面积(AUC)、灵敏度和特异度。采用双变量混合效应模型对X线摄影的灵敏度及特异度进行定量合并。对样本量>10万的亚组进行敏感性分析。由于筛查年代跨度较长,以筛查起始年每5年一个时段划分亚组,探讨筛查年份对乳腺X线摄影技术准确度的影响。本研究将人们普遍认为人群乳腺密度较致密的亚洲地区(中国、日本、韩国)研究对象以及欧洲地区及美国专门针对乳腺致密女性所做的研究合并,进行亚组分析。利用Q检验和I2统计量分析文献异质性,并将异质性分为低、中、高3个级别,对应的I2值分别为25%、50%、75%,P<0.05为差异有统计学意义。对样本量发表偏倚通过Deek漏斗图进行量化检测,P<0.05时认为存在发表偏移。
结 果1. 检索结果:通过检索式在Medline、Embase、Cochrane和CNKI电子数据库中共检索到相关文献1 167篇,手动检索补充57篇文献。参照纳入和排除标准,对文献进行初筛,通过阅读标题和摘要剔除文献946篇,然后对剩余文献进行全文阅读,共排除187篇文献,最终纳入文献48篇[7-11, 14-56],其中外文文献45篇,中文文献3篇[16, 19, 28]。文献筛选流程如图 1所示。

|
| 图 1 文献筛选流程 |
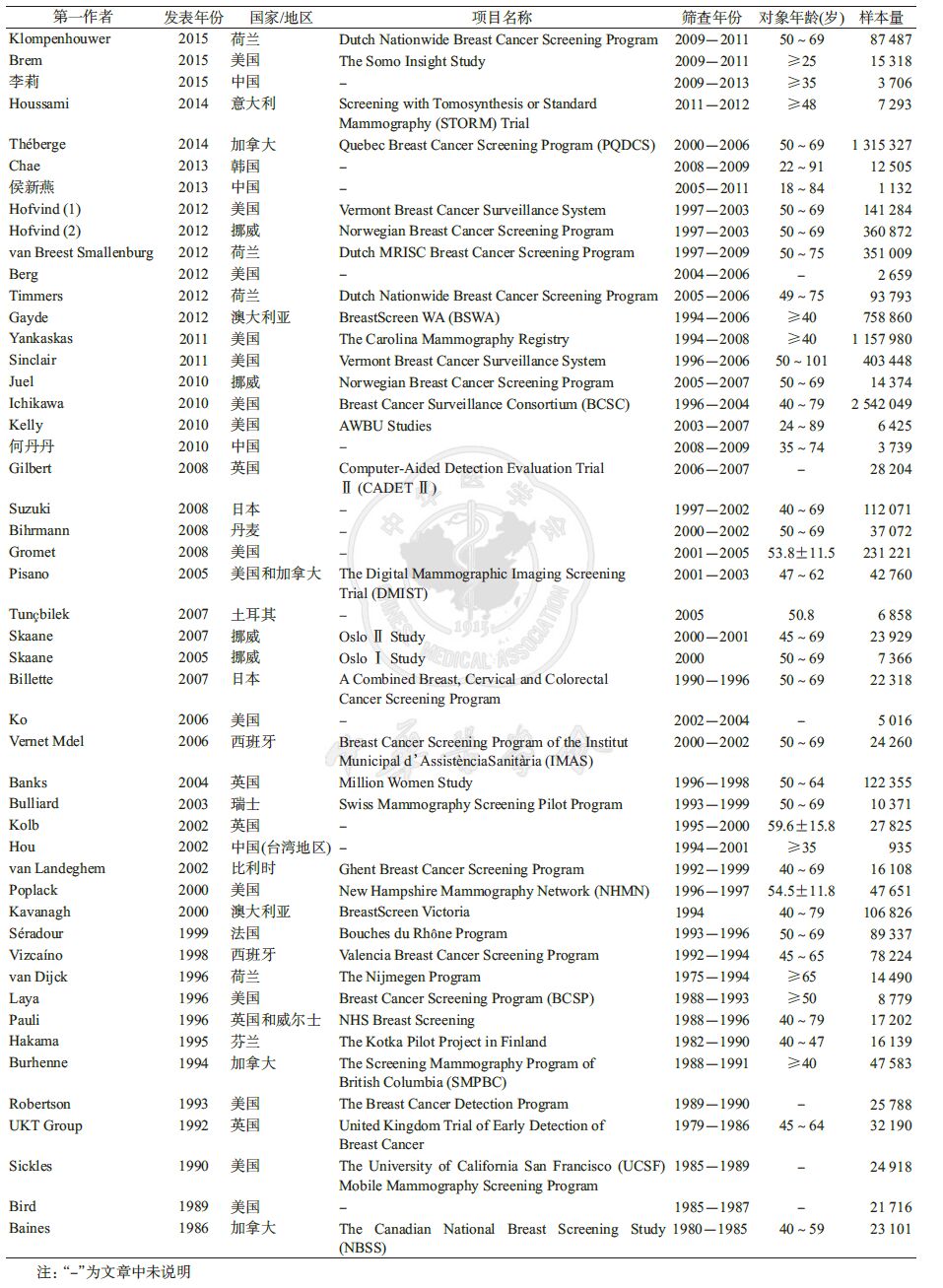
2. 纳入研究基本信息:Hofvind等[11]文献报道了两项独立的研究(美国和挪威),本次Meta分析共纳入49项研究。其中21项研究地点为欧洲地区,18项研究地点为北美洲地区,8项研究地点为亚洲地区,2项研究地点为大洋洲地区。纳入研究发表年份为1986-2015年,筛查年限为1975-2013年,最早的筛查项目来自荷兰[47],最近的筛查项目来自中国新疆维吾尔族女性的筛查项目[16]。纳入研究对象共计8 551 873例,各研究的样本量范围为935~2 542 049例,其中77.6%(38/49)研究样本量>1万例,24.5%(12/49)研究样本量>10万例。对象起止筛查年龄大部分在40~75岁,其中筛查对象为50~69岁年龄段人群的研究有11项(表 1)。
3. 纳入研究质量评价:依据QUADAS量表的评价准则,对纳入的49项研究进行质量评价,结果显示,纳入的研究质量均较高,仅少数条目显示部分研究存在偏倚(图 2)。Ko等[37]研究未完全排除乳腺癌患者,可能存在疾病谱偏倚;4项研究的研究对象为乳腺致密的人群[7-8, 15, 21],1项研究为乳腺癌患者的女性亲属[10],1项研究为临床乳腺检查阴性人群[33],1项研究为激素代替治疗人群[38],3项研究未详细说明纳入/排除标准[52, 54-55],可能存在选择标准偏倚;5项研究随访时间不一致或未明确说明随访时间,可能存在金标准偏倚[10, 34, 41, 45, 54];2项研究随访时间>6.3年[10, 50],可能存在疾病进展偏倚;Tuníbilek等[33]的研究筛查间期乳腺癌病例为0,Vizcaíno等[46]研究报道的特异度与通过四格表计算得到的特异度不一致,存在难以解释的试验结果偏倚。

|
| 图 2 纳入研究的方法学质量评价 |
4. 阈值效应检验:灵敏度及特异度分布未呈现“肩背状”,且SROC曲线关于反对角线对称(图 3),提示纳入的研究间不存在阈值效应。再对灵敏度与1-特异度进行相关性检验,得到Spearman系数为0.24,P=0.10>0.05,提示灵敏度和特异度是独立的,进一步证实两个变量间不存在阈值效应。X线摄影技术准确度评价的综合指标AUC为0.95(95%CI: 0.93~0.97)。

|
| 图 3 加权受试者工作特征曲线 |
5. Meta分析:采用双变量混合效应模型对总体灵敏度及特异度进行定量合成,结果显示,总体灵敏度为0.81(95%CI:0.77~0.84),总体特异度为0.96(95%CI:0.94~0.96)。异质性检验结果提示灵敏度和特异度均存在较大的异质性(P<0.05)。对样本量>10万的12项研究合并,敏感性分析结果显示:灵敏度略有增加,特异度不变,分别为0.83(95%CI:0.80~0.86)和0.95(95%CI:0.93~0.97),AUC为0.93(95%CI:0.91~0.95),提示本研究得到的乳腺X线摄影技术筛查准确度结果稳健。见图 4。虽然乳腺X线摄影技术筛查的年代跨度较长,但灵敏度和特异度的小幅波动不具有统计学意义(P>0.05),准确度的综合评价指标AUC非常稳定(图 5)。

|
| 图 4 乳腺X线摄影技术合并灵敏度和特异度的森林图 |

|
| 图 5 不同筛查年份乳腺X线摄影技术准确性比较 |
对于乳腺致密的女性,10项研究的荟萃分析发现X线摄影技术的筛查灵敏度下降明显,为0.74(95%CI:0.61~0.83),合并特异度为0.93(95%CI: 0.89~0.96),AUC为0.92(95%CI:0.89~0.94);对以上10项研究中,研究对象来自亚洲地区,即中国、日本、韩国的7项研究合并,分析结果也提示X线摄影对于亚洲地区女性筛查灵敏度和特异度均有不同程度降低,合并灵敏度为0.80(95%CI:0.69~0.88),合并特异度为0.94(95%CI:0.88~0.97),AUC为0.93(95%CI:0.91~0.95)。见图 6。

|
| 图 6 乳腺致密人群X线摄影筛查合并灵敏度及特异度的森林图 |
6. 发表偏倚:采用加权线性回归来检验漏斗图的对称性,以诊断优势比(DOR)为因变量,1/有效样本容量的平方根[root(ESS)]为自变量,权重为有效样本容量(图 7)。经计算,回归线的斜率为11.44,P=0.24>0.05,差异无统计学意义,表明纳入研究间不存在发表偏倚。

|
| 图 7 检验发表偏倚的Deek漏斗图 |
西方国家自20世纪90年代以来,乳腺癌病死率以每年2%的幅度持续下降,除因治疗方法改善外,主要得益于以乳腺X线检查为主的筛查工作的普遍开展。但癌症筛查从来就是一把利弊共存的双刃剑,它在带来病死率逐年下降之实效的同时,也可能带来放射线引起的损害以及过度诊断的问题。因此,筛查的综合质量对保持筛查利弊平衡至关重要[57],其中筛查技术的准确性是筛查质量保证的重要因素。本研究通过Meta分析的方法,系统评价了X线摄影技术应用于人群乳腺癌筛查的准确性,结果显示乳腺X线摄影技术筛查准确性高,研究结果稳健:总体灵敏度为0.81(95%CI: 0.77~0.84),特异度为0.96(95%CI:0.94~0.96),AUC为0.95(95%CI:0.93~0.97)。Mushlin等[5]对乳腺X线摄影技术筛查准确性的荟萃分析结果显示,随访1年X线摄影技术灵敏度为83%~95%,随访2年灵敏度为56%~86%,特异度为93.5%~99.1%。但该文献发表年份较久,仅纳入6项研究进行分析,样本量有限。本次Meta分析共纳入49项研究,样本量达到8 551 873例,>10万筛查人群的研究占24.5%。此外,本研究增加了筛查时间为2000年以后的多项研究,使得研究结果更具现实指导意义。本研究未限制随访间隔,对明确说明随访日期的41项研究发现,20项研究随访1年,1项研究随访1.5年,16项研究随访2年,2项研究随访2.5年,2项研究随访3年,因此本研究得到的合并灵敏度介于Mushlin等[5]报道的随访1年和随访2年灵敏度之间。2002年WHO/IARC在对全球范围内乳腺癌不同筛查方案的有效性和准确性进行了系统梳理和评估,共纳入20项研究,分析发现乳腺X线摄影筛查乳腺癌的灵敏度为68%~92%,特异度为82%~98%[6]。本次Meta分析得到的合并灵敏度和特异度将评价指标精确化,并且可信区间均在WHO/IARC报道的灵敏度和特异度范围内,一定程度上论证了本研究结果的可靠性。
本次Meta分析纳入的研究绝大部分为欧美地区研究,仅有8项研究来自亚洲地区,分别为中国、日本和韩国。考虑到研究对象乳腺密度对乳腺X摄影筛查准确性影响较大,亚洲地区女性乳腺癌发病高峰较西方国家前移约10~15年[1],且绝经前患者比例高,乳腺小且质地致密。因此,将4项亚洲地区人群研究以及3项乳腺致密(BI-RADS评分为3或4)的欧美地区人群研究合并,进行亚组分析。结果显示,乳腺X线摄影对于这部分人群筛查的准确性降低,主要表现为灵敏度显著降低,合并灵敏度仅为0.74(95%CI:0.61~0.83),而在欧美地区一般人群中筛查的合并灵敏度高达0.82(95%CI:0.78~0.85)。这一结果可以部分解释为什么乳腺X线检查的成本效果研究在亚洲地区女性中没有西方女性中那样令人信服,此外欧美地区保险体系下的专业乳腺随诊保健服务十分健全,漏诊率低也是不可忽视的一个因素。
虽然康敏等[58]的研究认为乳腺X线在亚洲地区女性乳腺癌筛查中同样拥有较高的准确性,但近期发表的一项中国人群多中心随机队列的研究结果发现乳腺X线摄影技术在中国30~65岁乳腺癌高风险女性中的筛查灵敏度仅为57.1%(95%CI:29.6%~81.2%),而乳腺B超筛查灵敏度却达到100.0%(95%CI:73.2%~100.0%)[59]。相对于乳腺X线摄影检查而言,超声检查具有对致密型乳腺内病变检出率高、便利、辐射损伤小、设备成本低等潜在优势,但对设备及检查医师技术、经验、诊断水平的依赖性强。虽然乳腺X线摄影对致密性腺体乳腺癌的筛查易出现假阴性,但对只出现钙化而没有肿块的类型,乳腺X线摄影拥有绝对优势。依据中国妇女乳房生物学特性和我国医疗资源的配置特点以及现有的医疗模式,国内专家提出乳腺X线摄影和乳腺B超互补应用于中国人群乳腺癌筛查,可提高筛查准确性。2009年起开展的农村妇女“两癌(乳腺癌、宫颈癌)”筛查及早诊早治项目乳腺癌检查均采用超声检查为主,阳性或可疑者补充乳腺X线摄影的筛查方案[60];2012年起,国家癌症中心开展的城市癌症早诊早治项目为40~44岁女性提供乳腺超声初筛(阳性者再行X线摄影),为45~69岁女性提供超声联合乳腺X线摄影的筛查方案[61]。为此,本研究团队后续也将对乳腺超声检查以及超声联合乳腺X线摄影筛查准确性进行系统综述研究。
筛查对象年龄、激素治疗情况、不同的乳腺X线摄影技术(专用屏-片摄影/全视野数字乳腺X线摄影)、摄影方位(单位片/双位片)、阅片方式(单人/双人/CAD辅助诊断)等因素均可能对乳腺X线摄影准确性产生影响。既往研究发现对于低年龄组[5, 26, 31]以及使用激素代替治疗[37]的筛查对象乳腺X线摄影准确性较低。全视野数字乳腺X线摄影对于50岁以下年龄组的筛查准确性较高[62]。本课题组后续将针对以上因素进行深入研究,为政策决策者制定前瞻性的乳腺癌筛查项目提供重要信息,优选筛查方案。
本研究汇总了全球范围乳腺X线摄影技术应用于乳腺癌筛查的准确性数据,一方面为政策决策者在制定前瞻性的乳腺癌筛查项目时提供了基础数据,另一方面有助于参与筛查的受试者更科学的权衡筛查的利弊。目前基于我国人群的严格科学设计的乳腺癌筛查技术准确度评价研究仍十分有限,因此,以科学严格的设计开展基于我国人群的低成本初筛技术和方案的综合评价将是下一步的重要工作方向。
| [1] | Ferlay J,Soerjomataram I,Ervik M,et al.GLOBOCAN 2012 v1.0,Cancer Incidence and Mortality Worldwide:IARC CancerBase No.11[EB/OL].Lyon,France:IARC Press,2013.http://globocan.iarc.fr. |
| [2] | To T, Wall C, Baines CJ, et al. Is carcinoma in situ a precursor lesion of invasive breast cancer?[J]. Int J Cancer , 2014, 135 (7) : 1646–1652 DOI:10.1002/ijc.28803 |
| [3] | Lauby-Secretan B, Scoccianti C, Loomis D, et al. International Agency for Research on Cancer Handbook Working Group.Breast-cancer screening-viewpoint of the IARC Working Group[J]. N Engl J Med , 2015, 372 (24) : 2353–2358 DOI:10.1056/NEJMsr1504363 |
| [4] | Gotzsche PC, Nielsen M. Screening for breast cancer with mammography[J]. Cochrane Database Syst Rev , 2013, 6 : CD001877 DOI:10.1002/14651858 |
| [5] | Mushlin AI, Kouides RW, Shapiro DE. Estimating the accuracy of screening mammography:a meta-analysis[J]. Am J Prev Med , 1998, 14 (2) : 143–153 DOI:10.1016/S0749-3797(97)00019-6 |
| [6] | International Agency for Research on Cancer World Health Organization.ARC handbooks of cancer prevention.Volume 7:Breast Cancer Screening[M].Lyon,France: IARC Press, 2002: 28–32 |
| [7] | Chae EY, Kim HH, Cha JH, et al. Evaluation of screening whole-breast sonography as a supplemental tool in conjunction with mammography in women with dense breasts[J]. J Ultrasound Med , 2013, 32 (9) : 1573–1578 DOI:10.7863/ultra.32.9.1573 |
| [8] | Kelly KM, Dean J, Comulada WS, et al. Breast cancer detection using automated whole breast ultrasound and mammography in radiographically dense breasts[J]. Eur Radiol , 2010, 20 (3) : 734–742 DOI:10.1007/s00330-009-1588-y |
| [9] | Suzuki A, Kuriyama S, Kawai M, et al. Age-specific interval breast cancers in Japan:estimation of the proper sensitivity of screening using a population-based cancer registry[J]. Cancer Sci , 2008, 99 (11) : 2264–2267 DOI:10.1111/j.1349-7006.2008.00926.x |
| [10] | Hou MF, Chuang HY, Ou-Yang F, et al. Comparison of breast mammography,sonography and physical examination for screening women at high risk of breast cancer in taiwan[J]. Ultrasound Med Biol , 2002, 28 (4) : 415–420 DOI:10.1016/S0301-5629(02)00483-0 |
| [11] | Hofvind S, Geller BM, Skelly J, et al. Sensitivity and specificity of mammographic screening as practised in Vermont and Norway[J]. Br J Radiol , 2012, 85 (1020) : e1226–1232 DOI:10.1259/bjr/15168178 |
| [12] | Whiting P, Rutjes AW, Reitsma JB, et al. The development of QUADAS:a tool for the quality assessment of diagnostic accuracy included in systematic reviews[J]. BMC Med Res Methodol , 2003, 3 : 25 DOI:10.1186/1471-2288-3-25 |
| [13] | Whiting P, Rutjes AW, Dinnes J, et al. Development and validation of methods for assessing the quality of diagnostic accuracy studies[J]. Health Technol Assess , 2004, 8 (25) : iii,1–234 DOI:10.3310/hta8250 |
| [14] | Klompenhouwer EG, Voogd AC, den Heeten GJ, et al. Blinded double reading yields a higher programme sensitivity than non-blinded double reading at digital screening mammography:a prospected population based study in the south of The Netherlands[J]. Eur J Cancer , 2015, 51 (3) : 391–399 DOI:10.1016/j.ejca.2014.12.008 |
| [15] | Brem RF, Tabár L, Duffy SW, et al. Assessing improvement in detection of breast cancer with three-dimensional automated breast US in women with dense breast tissue:the SomoInsight Study[J]. Radiology , 2015, 274 (3) : 663–673 DOI:10.1148/radiol.14132832 |
| [16] | 李莉, 刘巍, 汪湍, 等. 不同筛查方案在新疆维族女性乳腺癌筛查中的准确性及临床意义[J]. 中国医学前沿杂志:电子版 , 2015, 5 : 42–45 L, Liu W, Wang T, et al. The accuracy and clinical significance of different screening methods for breast cancer among Xinjiang Uigur women[J]. Chin J Frontiers Med Sci:Electronic Version , 2015, 5 : 42–45 |
| [17] | Houssami N, Macaskill P, Bernardi D, et al. Breast screening using 2D-mammography or integrating digital breast tomosynthesis (3D-mammography) for single-reading or double-reading-evidence to guide future screening strategies[J]. Eur J Cancer , 2014, 50 (10) : 1799–1807 DOI:10.1016/j.ejca.2014.03.017 |
| [18] | Théberge I, Chang SL, Vandal N, et al. Radiologist interpretive volume and breast cancer screening accuracy in a Canadian organized screening program[J]. J Natl Cancer Inst , 2014, 106 (3) : djt461 DOI:10.1093/jnci/djt461 |
| [19] | 侯新燕, 张江霞, 李丹. 超声和钼靶X线诊断乳腺癌的临床价值比较[J]. 中国肿瘤 , 2013, 3 : 198–201 X Y, Zhang JX, Li D. A comparison of clinical value between ultrasonography and mammography in the diagnosis for breast cancer[J]. Chin Cancer , 2013, 3 : 198–201 |
| [20] | van Breest Smallenburg V, Duijm LE, Voogd AC, et al. Mammographic changes resulting from benign breast surgery impair breast cancer detection at screening mammography[J]. Eur J Cancer , 2012, 48 (14) : 2097–2103 DOI:10.1016/j.ejca.2012.03.011 |
| [21] | Berg WA, Zhang Z, Lehrer D, et al. Detection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk[J]. JAMA , 2012, 307 (13) : 1394–1404 DOI:10.1001/jama.2012.388 |
| [22] | Timmers JM, van Doorne-Nagtegaal HJ, Zonderland HM, et al. The Breast Imaging Reporting and Data System (BI-RADS) in the Dutch breast cancer screening programme:its role as an assessment and stratification tool[J]. Eur Radiol , 2012, 22 (8) : 1717–1723 DOI:10.1007/s00330-012-2409-2 |
| [23] | Gayde C, Goolam I, Bangash HK, et al. Outcome of mammography in women with large breasts[J]. Breast , 2012, 21 (4) : 493–498 DOI:10.1016/j.breast.2011.12.001 |
| [24] | Yankaskas BC, May RC, Matuszewski J, et al. Effect of observing change from comparison mammograms on performance of screening mammography in a large community-based population[J]. Radiology , 2011, 261 (3) : 762–770 DOI:10.1148/radiol.11110653 |
| [25] | Sinclair N, Littenberg B, Geller B, et al. Accuracy of screening mammography in older women[J]. AJR Am J Roentgenol , 2011, 197 (5) : 1268–1273 DOI:10.2214/AJR.10.5442 |
| [26] | Juel IM, Skaane P, Hoff SR, et al. Screen-film mammography versus full-field digital mammography in a population-based screening program:The Sogn and Fjordane study[J]. Acta Radiol , 2010, 51 (9) : 962–968 DOI:10.3109/02841851.2010.504969 |
| [27] | Ichikawa LE, Barlow WE, Anderson ML, et al. Time trends in radiologists' interpretive performance at screening mammography from the community-based Breast Cancer Surveillance Consortium,1996-2004[J]. Radiology , 2010, 256 (1) : 74–82 DOI:10.1148/radiol.10091881 |
| [28] | 何丹丹, 方红, 黄俊, 等. 3740例社区女性乳腺癌筛查结果分析[J]. 中国慢性病预防与控制 , 2010, 4 : 413–415 D D, Fang H, Huang J, et al. The breast cancer screening results of 3740 female residents in a community of minhang district of Shanghai[J]. Chin J Prev Contr Chr Dis , 2010, 4 : 413–415 |
| [29] | Gilbert FJ, Astley SM, Gillan MG, et al. Single reading with computer-aided detection for screening mammography[J]. N Engl J Med , 2008, 359 (16) : 1675–1684 DOI:10.1056/NEJMoa0803545 |
| [30] | Bihrmann K, Jensen A, Olsen AH, et al. Performance of systematic and non-systematic(‘opportunistic’)screening mammography:a comparative study from Denmark[J]. J Med Screen , 2008, 15 (1) : 23–26 DOI:10.1258/jms.2008.007055 |
| [31] | Gromet M. Comparison of computer-aided detection to double reading of screening mammograms:review of 231221 mammograms[J]. AJR Am J Roentgenol , 2008, 190 (4) : 854–859 DOI:10.2214/AJR.07.2812 |
| [32] | Pisano ED, Gatsonis C, Hendrick E, et al. Diagnostic performance of digital versus film mammography for breast-cancer screening[J]. N Engl J Med , 2005, 353 (17) : 1773–1783 DOI:10.1056/NEJMoa052911 |
| [33] | Tunçbilek I, Ozdemir A, Gültekin S, et al. Clinical outcome assessment in mammography:an audit of 7506 screening and diagnostic mammography examinations[J]. Diagn Interv Radiol , 2007, 13 (4) : 183–187 |
| [34] | Skaane P, Hofvind S, Skjennald A. Randomized trial of screen-film versus full-field digital mammography with soft-copy reading in population-based screening program:follow-up and final results of OsloⅡstudy[J]. Radiology , 2007, 244 (3) : 708–717 DOI:10.1148/radiol.2443061478 |
| [35] | Skaane P, Skjennald A, Young K, et al. Follow-up and final results of the OsloⅠStudy comparing screen-film mammography and full-field digital mammography with soft-copy reading[J]. Acta Radiol , 2005, 46 (7) : 679–689 DOI:10.1080/02841850500223547 |
| [36] | Billette de Villemeur A, Exbrayat C, Garnier A, et al. Evaluation of a combined screening programme for breast,cervical and colorectal cancers in France[J]. Eur J Cancer Prev , 2007, 16 (1) : 26–35 DOI:10.1097/01.cej.0000228399.30235.bc |
| [37] | Ko JM, Nicholas MJ, Mendel JB, et al. Prospective assessment of computer-aided detection in interpretation of screening mammography[J]. AJR Am J Roentgenol , 2006, 187 (6) : 1483–1491 DOI:10.2214/AJR.05.1582 |
| [38] | Vernet Mdel M, Checa MA, Macià F, et al. Influence of hormone replacement therapy on the accuracy of screening mammography[J]. Breast J , 2006, 12 (2) : 154–158 DOI:10.1111/j.1075-122X.2006.00224.x |
| [39] | Banks E, Reeves G, Beral V, et al. Influence of personal characteristics of individual women on sensitivity and specificity of mammography in the Million Women Study:cohort study[J]. BMJ , 2004, 329 (7464) : 477 DOI:10.1136/bmj.329.7464.477 |
| [40] | Bulliard JL, de Landtsheer JP, Levi F. Results from the Swiss mammography screening pilot programme[J]. Eur J Cancer , 2003, 39 (12) : 1761–1769 DOI:10.1016/S0959-8049(03)00238-7 |
| [41] | Kolb TM, Lichy J, Newhouse JH. Comparison of the performance of screening mammography,physical examination,and breast US and evaluation of factors that influence them:an analysis of 27825 patient evaluations[J]. Radiology , 2002, 225 (1) : 165–175 DOI:10.1148/radiol.2251011667 |
| [42] | van Landeghem P, Bleyen L, de Backer G. Age-specific accuracy of initial versus subsequent mammography screening:results from the Ghent breast cancer-screening programme[J]. Eur J Cancer Prev , 2002, 11 (2) : 147–151 DOI:10.1097/00008469-200204000-00006 |
| [43] | Poplack SP, Tosteson AN, Grove MR, et al. Mammography in 53803 women from the New Hampshire mammography network[J]. Radiology , 2000, 217 (3) : 832–840 DOI:10.1148/radiology.217.3.r00dc33832 |
| [44] | Kavanagh AM, Giles GG, Mitchell H, et al. The sensitivity,specificity,and positive predictive value of screening mammography and symptomatic status[J]. J Med Screen , 2000, 7 (2) : 105–110 DOI:10.1136/jms.7.2.105 |
| [45] | Séradour B, Estève J, Heid P, et al. Hormone replacement therapy and screening mammography:analysis of the results in the Bouches du Rhône programme[J]. J Med Screen , 1999, 6 (2) : 99–102 DOI:10.1136/jms.6.2.99 |
| [46] | Vizcaíno I, Salas D, Vilar JS, et al. Breast cancer screening:first round in the population-based program in Valencia,Spain.Collaborative Group of Readers of the Breast Cancer Screening Program of the Valencia Community[J]. Radiology , 1998, 206 (1) : 253–260 DOI:10.1148/radiology.206.1.9423680 |
| [47] | van Dijck J, Verbeek A, Hendriks J, et al. Mammographic screening after the age of 65 years:early outcomes in the Nijmegen programme[J]. Br J Cancer , 1996, 74 (11) : 1838–1842 DOI:10.1038/bjc.1996.640 |
| [48] | Laya MB, Larson EB, Taplin SH, et al. Effect of estrogen replacement therapy on the specificity and sensitivity of screening mammography[J]. J Natl Cancer Inst , 1996, 88 (10) : 643–649 DOI:10.1093/jnci/88.10.643 |
| [49] | Pauli R, Hammond S, Cooke J, et al. Comparison of radiographer/radiologist double film reading with single reading in breast cancer screening[J]. J Med Screen , 1996, 3 (1) : 18–22 |
| [50] | Hakama M, Pukkala E, Kallio M, et al. Effectiveness of screening for breast cancer in women under 50 years at entry:the Kotka pilot project in Finland[J]. Int J Cancer , 1995, 63 (1) : 55–57 DOI:10.1002/(ISSN)1097-0215 |
| [51] | Burhenne HJ, Burhenne LW, Goldberg F, et al. Interval breast cancers in the Screening Mammography Program of British Columbia:analysis and classification[J]. AJR Am J Roentgenol , 1994, 162 (5) : 1067–1071 DOI:10.2214/ajr.162.5.8165983 |
| [52] | Robertson CL. A private breast imaging practice:medical audit of 25788 screening and 1077 diagnostic examinations[J]. Radiology , 1993, 187 (1) : 75–79 DOI:10.1148/radiology.187.1.8451440 |
| [53] | United Kingdom Trial of Early Detection of Breast Cancer Group. Specificity of screening in United Kingdom trial of early detection of breast cancer[J]. BMJ , 1992, 304 (6823) : 346–349 DOI:10.1136/bmj.304.6823.346 |
| [54] | Sickles EA, Ominsky SH, Sollitto RA, et al. Medical audit of a rapid-throughput mammography screening practice:methodology and results of 27114 examinations[J]. Radiology , 1990, 175 (2) : 323–327 DOI:10.1148/radiology.175.2.2326455 |
| [55] | Bird RE. Low-cost screening mammography:report on finances and review of 21716 consecutive cases[J]. Radiology , 1989, 171 (1) : 87–90 DOI:10.1148/radiology.171.1.2494683 |
| [56] | Baines CJ, Miller AB, Wall C, et al. Sensitivity and specificity of first screen mammography in the Canadian National Breast Screening Study:a preliminary report from five centers[J]. Radiology , 1986, 160 (2) : 295–298 DOI:10.1148/radiology.160.2.3523590 |
| [57] | Von Karsa L, Dean P, Arrossi S.Screening principles.World cancer report[M].Lyon,France: IARC Press, 2014: 322–329 |
| [58] | 康敏, 庞轶, 李佳圆, 等. 钼靶X线在亚洲女性乳腺癌筛查中的准确性评价[J]. 中华肿瘤杂志 , 2010, 32 (3) : 212–216 M, Pang Y, Li JY, et al. Accuracy evaluation of mammography in the breast cancer screening in Asian women:a community-based follow-up study and meta analysis[J]. Chin J Oncol , 2010, 32 (3) : 212–216 |
| [59] | Shen S, Zhou Y, Xu Y, et al. A multi-center randomized trial comparing ultrasound vs mammography for screening breast cancer in high-risk Chinese women[J]. Br J Cancer , 2015, 112 (6) : 998–1004 DOI:10.1038/bjc.2015.33 |
| [60] | 国家卫生计生委.卫生部、全国妇联关于印发《农村妇女"两癌"检查项目管理方案》的通知[EB/OL].(2009-06-30)[2016-04-01].http://www.nhfpc.gov.cn/fys/s3581/200906/cd3c33a7ad624a50b8100b262041dabe.shtml. The National Health and Family Planning Commission.Notice of the ministry of health and the national women's federation on the issuance of rural women "two cancer screening program" management[EB/OL].(2009-06-30)[2016-04-01].http://www.nhfpc.gov.cn/fys/s3581/200906/cd3c33a7ad624a50b8100b 262041dabe.shtml. |
| [61] | 代敏, 石菊芳, 李霓. 中国城市癌症早诊早治项目设计及预期目标[J]. 中华预防医学杂志 , 2013, 47 (2) : 179–182 M, Shi JF, Li N. The design and expectation of Cancer Screening Program in urban China[J]. Chin J Prev Med , 2013, 47 (2) : 179–182 |
| [62] | Souza FH, Wendland EM, Rosa MI, et al. Is full-field digital mammography more accurate than screen-film mammography in overall population screening? A systematic review and meta-analysis[J]. Breast , 2013, 22 (3) : 217–224 DOI:10.1016/j.breast.2013.02.013 |