 2016, Vol. 37
2016, Vol. 37文章信息
- 王颖, 李玫, 解冰洁, 郭朋鸽, 程雁鹏, 冯永亮, 张萍, 邬惟为, 王素萍, 张亚玮, 杨海澜 .
- Wang Ying, Li Mei, Xie Bingjie, Guo Pengge, Cheng Yanpeng, Feng Yongliang, Zhang Ping, Wu Weiwei, Wang Suping, Zhang Yawei, Yang Hailan .
- 妊娠期高血压疾病对小于胎龄儿的影响及潜在交互作用研究
- Influence of hypertension disorder complicating pregancy and its interaction with other factors on incidence of small for gestational age
- 中华流行病学杂志, 2016, 37(9): 1283-1287
- CHINESE JOURNAL OF EPIDEMIOLOGY, 2016, 37(9): 1283-1287
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2016.09.020
-
文章历史
收稿日期: 2016-04-05




2. 030001 太原, 第一医院妇产科;
3. 耶鲁大学公共卫生学院环境健康科学系
2. Obstetrics and Gynecology of First Affiliated Hospital, Shanxi Medical University, Taiyuan 030001, China;
3. Division of Environmental Health Sciences, School of Public Health, Yale University, USA
妊娠期高血压疾病(HDCP)是常见的妊娠期并发症,也是影响新生儿低出生体重的重要原因之一[1]。低出生体重儿是指出生体重低于2 500 g的新生儿,而小于胎龄儿(SGA)是指出生体重在同胎龄儿平均出生体重的第10百分位(P10)以下的婴儿,即排除了孕周对出生体重的干扰,更能较为全面地反映胎儿生长发育情况。SGA是导致新生儿死亡的重要原因,其成年后发生慢性非传染性疾病概率也明显升高[2-3]。目前国内外研究提示HDCP是胎儿低出生体重的危险因素[4],但有关HDCP对SGA影响的研究较少,尽管有学者提出HDCP是发生SGA的危险因素[5-6],但HDCP是一种复杂的妊娠合并症,不同临床亚型可能对SGA的作用存在差异,此外HDCP还可能与其他因素存在联合作用。为此本次研究采用巢式病例对照研究探讨HDCP及其各临床亚型对SGA的影响,并分析其潜在的交互作用,为临床干预提供参考依据。
对象与方法1. 研究对象:以2012年3月至2015年7月于山西医科大学第一医院产科住院分娩孕妇为研究队列,所有研究对象均经知情同意后采集病历信息及问卷调查收集孕妇产前、产中及产后的流行病学和临床资料,同时收集新生儿基本信息。入组标准:①母亲(孕妇)需知情同意,自愿参加;②婴儿为单胎活产,无出生缺陷。其中剔除孕周<20周、人工流产及大于胎龄儿等情况者。共收集789例SGA作为病例组,5 508例正常胎龄儿作为对照组。
2. 问卷设计与调查方法:采用统一的孕期妇女健康调查问卷,由培训合格调查人员对分娩后孕妇进行面对面调查,并查阅相关病历信息。调查问卷采用标准化的结构式调查问卷,内容包括一般人口学特征、生活方式和可能的混杂因素(包括生育史、病史、围产期保健、职业、吸烟、饮酒情况及体育活动情况)。
3. 诊断标准和定义:①HDCP诊断依据“妊娠期高血压疾病诊治指南(2015版)”[7],并分为妊娠期高血压、子痫前期/子痫、妊娠合并慢性高血压、慢性高血压并发子痫前期四类。②妊娠胎儿娩出<37周(258 d)定义为早产。③婴儿出生体重低于同胎龄儿平均出生体重P10以下定义为SGA,在同胎龄儿平均出生体重的P10至P90者为适于胎龄儿(AGA),并以我国婴儿出生体重百分位数值报告为判定标准[8]。
4. 统计学分析:采用EpiData 3.1软件录入问卷,应用SAS 9.3软件进行数据清理及数据分析。单因素分析采用 χ2检验,多因素分析及相乘交互作用采用非条件logistic回归分析。鉴于HDCP可致全身小动脉发生痉挛,造成胎盘早剥、羊水偏少使胎儿摄氧降低,影响生长发育,导致早产而常发生SGA[9],故本研究采用Andersson等[10]编制的Excel软件分析HDCP与早产、胎盘早剥、性别、羊水偏少的相加交互作用,用交互作用超额相对危险度(RERI)=RR11-RR10-RR01+1、交互作用归因比(AP)=RERI/RR11和交互作用指数(SI)=(RR11-1)/[(RR01-1)+(RR10-1)]对交互作用进行评价,其中RR11表示两因素同时存在,RR10、RR01分别表示只存在单因素。当RERI和AP的可信区间包含0、SI的可信区间包含1时,认为两因素无相加交互作用。
结 果1. 一般特征:2012年3月至2015年7月于山西医科大学第一医院产科分娩孕妇共6 297人,年龄15~59岁,平均(28.76±4.58)岁。新生儿平均出生体重(3 086.78±508.98) g,平均孕周(38.47±1.98)周。HDCP 836例,发生率为13.28%,其中既往慢性高血压87例(10.41%),HDCP中于孕早期发现191例(22.84%),孕中期发现56例(6.70%),孕晚期发现502例(60.05%)。SGA 789例,发生率为12.53%。
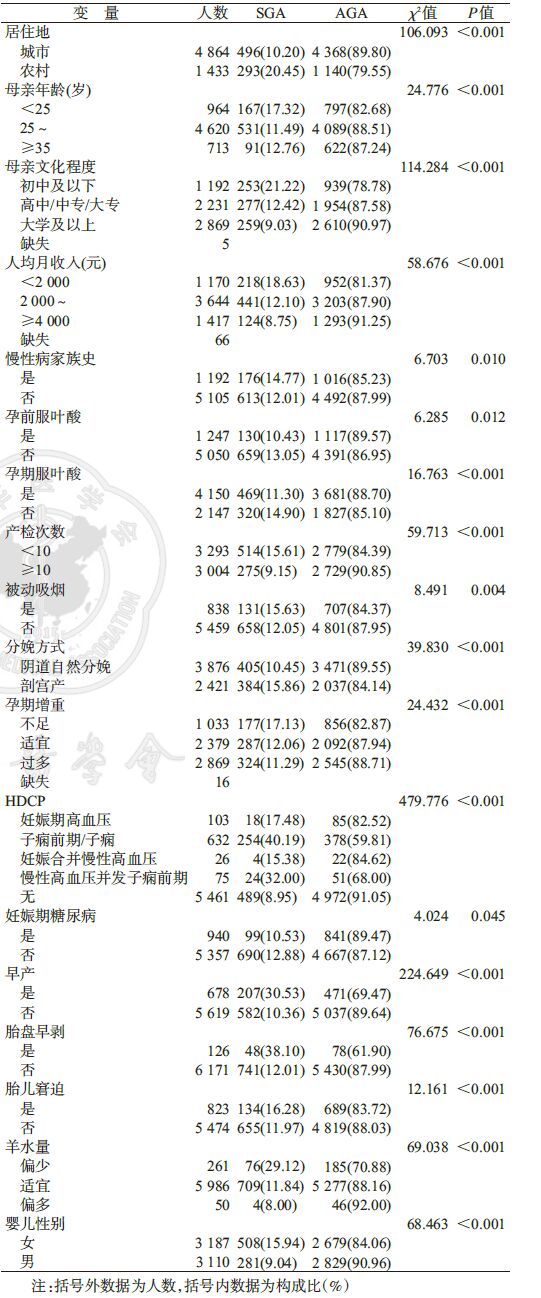
2. SGA发生情况及影响因素:单因素分析显示,居住地、孕妇年龄、文化程度、人均月收入、慢性病家族史、孕前或孕期补充叶酸、产检次数、被动吸烟、分娩方式、孕期增重、HDCP、妊娠期糖尿病、早产、胎盘早剥、胎儿窘迫、羊水量、婴儿性别与SGA发生有关,差异有统计学意义(P<0.05),见表 1。
3. HDCP对SGA的影响因素分析:836例HDCP中分娩SGA 300例,发生率为35.89%。非条件logistic回归分析显示,与非HDCP孕妇相比,妊娠期高血压孕妇、子痫前期/子痫孕妇和慢性高血压并发子痫前期孕妇发生SGA的危险均明显升高(分别为aOR=2.185,95%CI:1.266~3.770;aOR=5.322,95%CI:4.224~6.707;aOR=3.794,95%CI:2.190~6.573),见表 2。

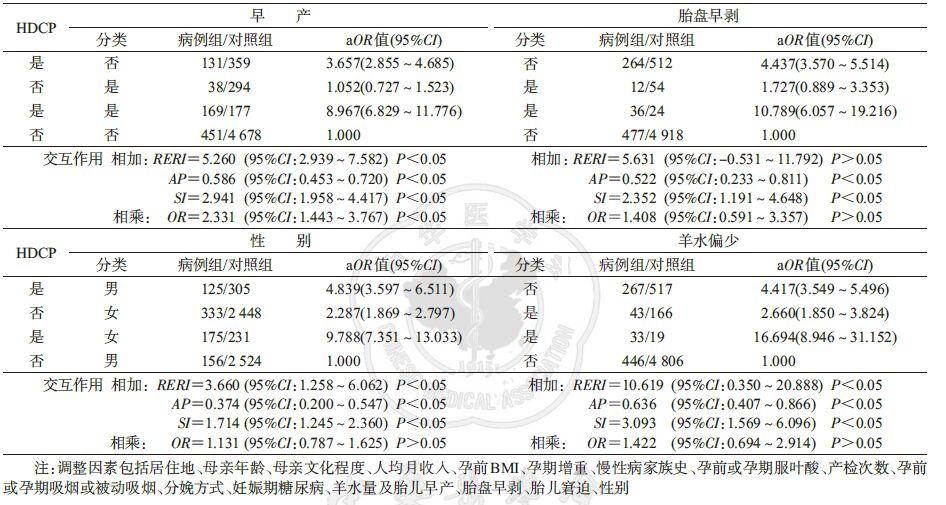
4. HDCP与其他因素的交互作用:分析结果显示,HDCP与早产存在相加交互作用(RERI=5.260,AP=0.586,SI=2.941)和相乘交互作用(OR=2.331,95%CI:1.443~3.767),并与胎盘早剥(RERI=5.631,AP=0.522,SI=2.352)、胎儿性别为女(RERI=3.660,AP=0.374,SI=1.714)、羊水偏少(RERI=10.619,AP=0.636,SI=3.093)均存在相加交互作用,未发现存在相乘交互作用(表 3)。
HDCP可增加低出生体重儿的发生风险[4, 11]。国内外研究显示,HDCP孕妇分娩SGA的发生率高[5-6],但缺乏HDCP临床亚型对SGA影响的研究。Muhammad等[12]研究显示,妊娠期高血压孕妇发生SGA的危险明显升高(OR=3.8,95%CI:1.2~6.9),但其样本例数较少(n=200);Xiong和Fraser[13]研究提示,妊娠期高血压及子痫前期均增加SGA的发生风险,但未控制相关混杂因素及未考虑临床亚型等因素的作用。本研究结果表明,妊娠期高血压孕妇、子痫前期/子痫孕妇和慢性高血压并发子痫前期孕妇均增加SGA的发生危险,而妊娠合并慢性高血压对SGA无影响,其发生机制还有待在大样本人群中进一步探讨。
本研究发现,HDCP和早产存在相加交互作用,两因素同时存在时SGA的发生风险是两者单独存在时风险之和的2.941倍(SI),其中有58.6%(AP)胎儿发生SGA的风险可归因于母亲HDCP与早产的交互作用。同时发现HDCP与早产之间存在相乘交互作用(OR=2.331,95%CI:1.443~3.767),提示患HDCP时,胎儿早产发生SGA的风险增加。Groom等[14]研究也表明,相对于只患HDCP的孕妇,患HDCP合并早产的孕妇更易分娩SGA。
大量研究表明,胎盘早剥增加了SGA的发生风险[15]。本文的交互作用结果显示,HDCP与胎盘早剥间存在相加交互作用,HDCP合并胎盘早剥的孕妇,其胎儿发生SGA的风险是对照组的10.79倍,提示患HDCP且合并胎盘早剥时发生SGA的风险增加。
目前国内外未见HDCP与羊水偏少是否在引起胎儿发生SGA具有交互作用的研究报道。本研究发现,HDCP与羊水偏少存在相加交互作用,两因素同时存在时胎儿发生SGA的风险是两者单独存在时风险之和的3.093倍(SI)。因此,当母亲为HDCP且合并羊水偏少时发生SGA的风险增加。此外,交互作用结果显示,HDCP与胎儿性别为女性存在相加交互作用。
综上所述,HDCP是发生SGA的危险因素,并与胎盘早剥、胎儿性别、羊水偏少均存在相加交互作用,与早产存在相加及相乘交互作用。因此,对有HDCP发病高危因素的孕妇,应综合考虑给予合理的妊娠前指导及妊娠期保健措施,预防SGA的发生。
| [1] | Liu CM, Cheng PJ, Chang SD. Maternal complications and perinatal outcomes associated with gestational hypertension and severe preeclampsia in Taiwanese women[J]. J Formos Med Assoc , 2008, 107 (2) : 129–138 DOI:10.1016/S0929-6646(08)60126-6 |
| [2] | Bjørge T, Sørensen HT, Grotmol T, et al. Fetal growth and childhood cancer:a population-based study[J]. Pediatrics , 2013, 132 (5) : e1265–1275 DOI:10.1542/peds.2013-1317 |
| [3] | Barker DJP, Osmond C, Forsén TJ, et al. Trajectories of growth among children who have coronary events as adults[J]. N Engl J Med , 2005, 353 (17) : 1802–1809 DOI:10.1056/NEJMoa044160 |
| [4] | Rahman LA, Hairi NN, Salleh N. Association between pregnancy induced hypertension and low birth weight:a population based case-control study[J]. Asia Pac J Public Health , 2008, 20 (2) : 152–158 DOI:10.1177/1010539507311553 |
| [5] | Sebastian T, Yadav B, Jeyaseelan L, et al. Small for gestational age births among South Indian women:temporal trend and risk factors from 1996 to 2010[J]. BMC Pregnancy Childbirth , 2015, 15 : 7 DOI:10.1186/s12884-015-0440-4 |
| [6] | 唐新意, 肖作源, 李咏梅, 等. 小于胎龄儿产科危险因素的病例对照研究[J]. 中华流行病学杂志 , 2005, 26 (11) : 915–918 X Y, Xiao ZY, Li YM, et al. A case-control study on small-for-gestational-age in relation to obstetrical risk factors[J]. Chin J Epidemiol , 2005, 26 (11) : 915–918 |
| [7] | 中华医学会妇产科学分会妊娠期高血压疾病学组. 妊娠期高血压疾病诊治指南(2015版)[J]. 中华妇产科杂志 , 2015, 50 (10) : 721–728 DOI:10.3760/cma.j.issn.0529-567x.2015.10.001 Chinese Medical Association Branch of Obstetrics and Gynecology Hypertensive Disorder Complicating Pregnancy Group. Hypertensive disorder complicating pregnancy diagnosis and treatment guidelines (2015 edition)[J]. Chin J Obstet Gynecol , 2015, 50 (10) : 721–728 DOI:10.3760/cma.j.issn.0529-567x.2015.10.001 |
| [8] | Dai L, Deng CF, Li YH, et al. Birth weight reference percentiles for Chinese[J]. PLoS One , 2014, 9 (8) : e104779 DOI:10.1371/journal.pone.0104779 |
| [9] | Graner S, Klingberg-Allvin M, Phuc HD, et al. Adverse perinatal and neonatal outcomes and their determinants in rural Vietnam 1999-2005[J]. Paediatr Perinat Epidemiol , 2010, 24 (6) : 535–545 DOI:10.1111/j.1365-3016.2010.01135.x |
| [10] | Andersson T, Alfredsson I, Källberg H, et al. Calculating measures of biological interaction[J]. Eur J Epidemiol , 2005, 20 (7) : 575–579 DOI:10.1007/s10654-005-7835-x |
| [11] | Sachan R, Patel ML, Sachan P, et al. Outcomes in hypertensive disorders of pregnancy in the North Indian population[J]. Int J Womens Health , 2013, 5 : 101–108 DOI:10.2147/IJWH.S40473 |
| [12] | Muhammad T, Khattak AA, Shafiqur-Rehman, et al. Maternal factors associated with intrauterine growth restriction[J]. J Ayub Med Coll Abbottabad , 2010, 22 (4) : 64–69 |
| [13] | Xiong X, Fraser WD. Impact of pregnancy-induced hypertension on birthweight by gestational age[J]. Paediatr Perinat Epidemiol , 2004, 18 (3) : 186–191 DOI:10.1111/j.1365-3016.2004.00553.x |
| [14] | Groom KM, North RA, Poppe KK, et al. The association between customised small for gestational age infants and pre-eclampsia or gestational hypertension varies with gestation at delivery[J]. BJOG , 2007, 114 (4) : 478–484 DOI:10.1111/j.1471-0528.2007.01277.x |
| [15] | McCowan L, Horgan RP. Risk factors for small for gestational age infants[J]. Best Pract Res Clin Obstet Gynaecol , 2009, 23 (6) : 779–793 DOI:10.1016/j.bpobgyn.2009.06.003 |