 2016, Vol. 37
2016, Vol. 37文章信息
- 王宝华, 王宁, 冯雅靖, 殷鹏, 李镒冲, 刘世炜, 周脉耕.
- Wang Baohua, Wang Ning, Feng Yajing, Yin Peng, Li Yichong, Liu Shiwei, Zhou Maigeng.
- 1990年与2013年中国人群胃癌疾病负担分析
- Disease burden of stomach cancer in the Chinese population, in 1990 and 2013
- 中华流行病学杂志, 2016, 37(6): 763-767
- Chinese Journal of Epidemiology, 2016, 37(6): 763-767
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2016.06.004
-
文章历史
- 投稿日期: 2016-03-04




2. 100050 北京, 中国疾病预防控制中心慢性非传染性疾病预防控制中心生命登记与死因监测室;
3. 100050 北京, 中国疾病预防控制中心慢性非传染性疾病预防控制中心综合防控与评价室;
4. 100050 北京, 中国疾病预防控制中心慢性非传染性疾病预防控制中心
2. Division of Vital Statistics and Death Surveillance, Chinese Center for Disease Control and Prevention, Beijing 100050, China;
3. Division of Integrated Prevention and Evaluation, National Center for Chronic and Noncommunicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 100050, China;
4. National Center for Chronic and Noncommunicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 100050, China
恶性肿瘤已成为严重影响人类健康的疾病,给社会和家庭带来沉重负担。据GLOBOCAN 2012(IARC)估计[1],胃癌居全球恶性肿瘤发病第五位、死亡第三位,超过70%的病例发生在发展中国家,2012年全球胃癌新发病例95.2万,中国占42.5%;同期全球死于胃癌病例共72.3万,中国占44.9%。20世纪70年代至90年代我国胃癌一直位居恶性肿瘤死因顺位首位[2],目前胃癌居所有恶性肿瘤发病第二位、死亡第三位[3, 4]。
本研究利用2013年全球疾病负担研究项目(GBD2013)[5]中国分省数据,应用发病、死亡、伤残调整寿命年(DALY)、过早死亡损失寿命年(YLL)和伤残损失寿命年(YLD)等指标,综合评价1990年与2013年中国及各省份胃癌疾病负担及变化情况。
资料与方法1. 资料来源:中国分省疾病负担研究是GBD 2013的一部分。GBD2013中国死因信息的数据来源:全国疾病监测点系统死因监测、全国妇幼卫生监测网、中国CDC死因登记报告信息系统、全国肿瘤登记数据、澳门地区和香港地区死因数据;肿瘤发病数据来源于全国肿瘤登记数据和文献回顾。GBD2013及中国分省疾病负担研究的详细介绍见文献[6, 7]。本研究选取1990年和2013年中国及各省份胃癌疾病负担指标进行分析。
2. 发病率和死亡率的估计:在全死因结果估计的基础上[6],利用全国肿瘤登记的发病和死亡数据,估算不同省份分年龄组、性别和年份的胃癌死亡发病比(mortality incidence ratio,MI ratio),再通过MI ratio由胃癌死亡数据估算出发病数据,具体计算方法见文献[6, 7, 8, 9]。
3. 疾病负担测量指标:为估算胃癌造成的寿命损失,采用YLL、YLD及DALY作为测量疾病负担的主要指标。利用GBD2010研究中的标准方法[10],将各年龄组死因别死亡人数乘以该年龄组平均死亡年龄上的期望寿命计算寿命损失年,其中DALY=YLL+YLD,YLL和YLD的估算方法详见文献[11, 12]。年龄别YLL率、YLD率和DALY率的计算为各年龄组“损失生命年数”除以该年龄组的人口数。
4. 数据分析:本研究描述2013年我国各年龄段胃癌发病、死亡、死亡构成比、DALY等疾病负担现况,分析2013年与1990 年我国不同性别人群胃癌发病变化情况;比较1990年与2013年全国胃癌疾病负担情况及变化幅度以及各省份胃癌发病、死亡及变化情况。同时为了消除不同年代人口构成的影响,使用GBD2013全球分年龄组标准人口对发病率、死亡率、DALY率、YLL率和YLD率分别进行标化[6] 。
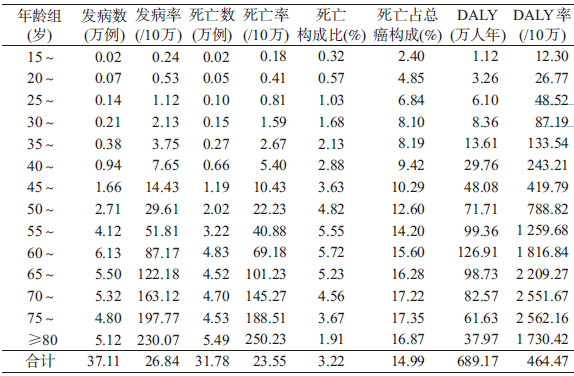
结果1. 胃癌疾病负担现状:2013年我国胃癌发病37.11万例,死亡31.78万例,发病率、死亡率、DALY率分别为26.84/10万、23.55/10万、464.47/10万。55岁及以上人群胃癌死亡率超过40/10万。发病率、死亡率、DALY率有随着年龄增加而逐渐增加的趋势。胃癌死亡人数占总死亡人数3.22%,60~64岁组最高(5.72%);胃癌死亡人数占总癌死亡人数的14.99%,75~79岁组最高(17.35%)。15岁以下人群因发病和死亡极低未列入表中(表 1)。
2. 1990-2013年中国胃癌不同性别标化发病率变化:1990-2013年胃癌标化发病率总体呈下降趋势,从1990年的34.86/10万降至2013年的26.84/10万,降幅为23.02%;23年间中国男性胃癌标化发病率均高于女性(2.03~2.67倍);男女性胃癌发病率均呈下降趋势,女性降幅(17.64%)高于男性(37.36%),见图 1。

|
| 图 1 1990-2013年中国胃癌分性别标化发病率变化 |
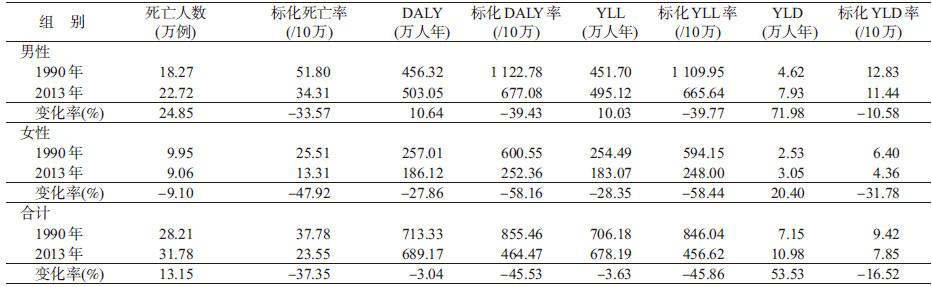
3. 1990与2013年中国不同性别人群胃癌所造成的疾病负担及变化:1990和2013年我国胃癌总死亡数分别为28.21万、31.78万,增加13.15%;标化死亡率分别为37.78/10万、23.55/10万,下降37.35%;标化DALY、标化YLL率、标化YLD率均下降。与1990年相比,2013年我国男性胃癌DALY、YLL、YLD均增加;男女性标化DALY率、YLL率、YLD率下降,女性降幅均大于男性(表 2)。
4. 1990年与2013年各省份胃癌发病、死亡及变化:2013年胃癌标化发病率最高的3个省份为青海(56.16/10万)、安徽(43.42/10万)、甘肃(42.24/10万),较低的有天津(10.32/10万)、北京(11.13/10万)、广东(12.55/10万)。与1990年比较,2013年多数省的胃癌标化发病率下降,降幅大的前三位为天津(64.07%)、上海(49.50%)、浙江(48.06%),而少数省份标化发病率略有升高,如贵州、河北、云南、海南,其中贵州升高达18.70%(表 3)。
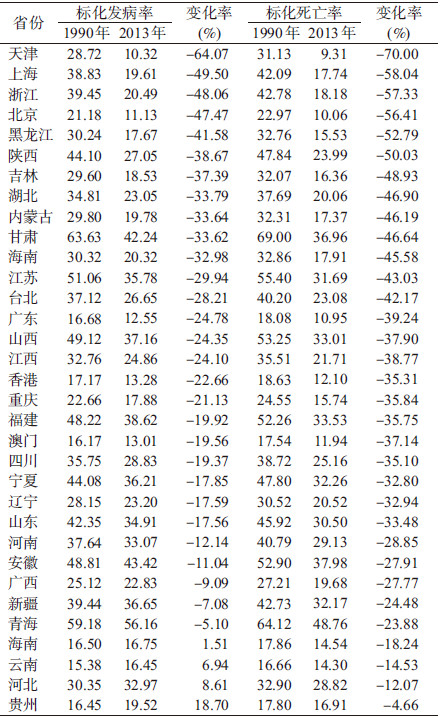
2013年胃癌标化死亡率较高的3个省份:青海(48.76/10万)、安徽(37.98/10万)、甘肃(36.96/10万),较低的有天津(9.31/10万)、北京(10.06/10万)、广东(10.95/10万)。1990年比较,2013年所有省份的胃癌标化死亡率均下降,前三位为天津(70.00%)、上海(58.04%)、浙江(57.33%),贵州、河北、云南、海南降幅低于20%(表 3)。
讨论本研究结果显示,2013年中国胃癌疾病负担处于较高水平,发病和死亡人数均超过30万,约占全国人群总死亡的3%和总癌死亡的15%,与同年全球数据比较[6],中国胃癌分别居全球胃癌发病第五位、死亡第六位,发病数、死亡数、DALY数各占全球胃癌(98.4万、84.1万、1 790万)的37.7%、37.8%、38.5%,中国胃癌发病率和死亡率远远高于全球平均水平(16.1/10万、13.8/10万),提示中国在全球属于胃癌高发国家,胃癌是影响中国人群健康的重要疾病负担。
胃癌的发生和死亡受多种因素影响,不仅与年龄、性别、遗传等个体因素有关,还与当地的经济文化、饮食习惯、生活方式、医疗水平等有关。据世界癌症研究基金会报告[13],胃癌的发病率与当地幽门螺杆菌(Helicobacter pylori,Hp)感染呈正相关,中国人群Hp感染非常普遍,成年人感染率为40%~60%[14],可能是导致胃癌高发的重要原因。研究表明,通过规范药物疗法治愈Hp感染可预防胃癌发生[15],根除Hp将是降低胃癌发病率最有希望的策略[16]。食盐摄入量增加也与胃癌发生相关[13]。从全球来看,传统饮食很咸的地区(如亚洲和拉丁美洲部分地区)其胃癌的发生率较高。据中国居民营养与慢性病状况报告[4],1992、2002、2012年中国18岁及以上居民每日烹调盐摄入量分别为12.9、12.0、10.5 g,明显高于WHO提出的健康成年人每日5 g盐标准。另外,居民的某些不良饮食生活习惯,如吸烟/饮酒、摄入加工肉类及腌熏煎烤炸食物、水果蔬菜摄入不足等,也可增加胃癌发生风险[13];吸烟与胃癌发生风险呈剂量反应关系[17]。调查数据显示,1996、2002、2010年我国15岁以上居民吸烟率分别为35.3%、31.1%、28.1%[4],2010年吸烟人数超过3亿,成年居民有害饮酒率9.3%、红肉摄入过多比例为27.4%、水果蔬菜摄入不足比例为52.8%[18],提示胃癌的高发可能与人群中胃癌危险因素的高暴露密切相关。
近几十年来,随着社会经济发展、饮食条件改善、医疗水平提高,世界上大部分国家胃癌的发病和死亡呈下降趋势。胃癌曾是中国最常见的恶性肿瘤,据全国的三次死因调查显示,20世纪70年代、90年代胃癌死亡率分别为17.40/10万和25.16/10万,居恶性肿瘤死因第一位,2004-2005年胃癌退居第三位,死亡率为24.71/万[2]。本研究结果显示,1990-2013年中国人群胃癌发病率、死亡率、DALY率、YLL率、YLD率均下降,究其原因,一方面,几十年来我国居民经济和生活条件改善、新鲜蔬菜水果摄入增加,人们营养状况改善、机体免疫力提高、胃癌危险因素的暴露减少;另一方面,我国胃癌诊疗技术的进步,特别是内窥镜、Hp检测等人群筛查技术得到不断完善[19],以及在胃癌高发区人群中开展胃癌早诊早治,覆盖人群逐渐增加,对胃癌及癌前疾病的早期发现、及时治疗、降低胃癌发病和死亡起到重要作用。在日本和韩国,因有国家癌症筛查项目,检出的早期胃癌占全部胃癌的50%,而中国的早期胃癌检出病例只占胃癌的5%~20%,在胃癌高危人群中进行筛查和早诊早治是改变我国胃癌诊治严峻形势的高效可行途径[19]。
本研究显示,胃癌发病率、死亡率、DALY率有随着年龄增加而逐渐增加的趋势,55岁及以上人群胃癌发病率超过50/10万、死亡率超过40/10万。50岁以下的人群胃癌发生较低,与国内外相关报道一致[20, 21, 22]。在当前我国人口老龄化趋势下,加强中老年人胃癌防控对减少胃癌疾病负担有重要作用。世界各国胃癌发病率和死亡率均男性高于女性,GLOBOCAN 2012数据显示,男女性胃癌发病比例在不同国家范围为2.6~3.3[1],胃癌发病率高的地区男女性比值也相对较高。本研究结果显示,1990-2013年的各年份间,男性胃癌标化发病率均高于女性(2.03~2.67倍),且女性降幅大于男性,1990年和2013年男性胃癌死亡率、DALY率、YLL率、YLD率均高于女性,男性的DALY、YLL、YLD值增加。造成胃癌发病男高女低的原因可能与吸烟、饮酒等习惯[23]、遗传因素、激素分泌差异[24]、职业暴露等方面不同有关,例如2010年我国15岁及以上男性吸烟率高达52.9%,女性为2.4%;成年男女性有害饮酒率分别为11.1%和2.0%,男性是女性的5.5倍[4]。本研究提示,年龄、性别因素是影响胃癌疾病负担的重要原因,应加强中老年男性等重点人群胃癌防控。
本研究各省份数据显示,多数省份胃癌发病和死亡高于世界平均水平,西北、华北和华东地区明显高于其他地区,东北、中南、西南地区相对较低。2013年胃癌发病率和死亡率最高的前三位均为青海、安徽、甘肃,最低的前三位均为天津、北京、广东,其原因可能与各地区的经济文化条件、生活饮食习惯、自然地理环境不同以及医疗资源不均衡有关。与1990年比较,2013年多数省份胃癌发病率下降、所有省份胃癌死亡率下降,天津、上海、浙江降幅较大。世界上很多发达国家自20世纪以来经历了胃癌发病和死亡呈明显持续下降的过程,很可能与冰箱的使用、饮食结构改变和膳食营养状况提高等环境因素改变有关[25]。在我国胃癌发病和死亡降幅较大的省份,近几十年来经济水平、医疗卫生、蔬菜水果消费等也有较大改善,例如自1980年以来,天津市居民的新鲜蔬菜和水果消费量、冰箱使用率显著增加,而腌制等加工食品的摄入量减少[26]。良好的饮食习惯和生活方式对胃癌的防治有着重要的意义。目前我国人口老龄化趋势、各地区发展不平衡,以及环境中许多未知的致/促癌因素存在,胃癌的防治在较长时间内仍然是卫生工作的一大重点。
综上所述,中国胃癌疾病负担处于较高水平,并随年龄增长而增加,男性疾病负担高于女性;与1990年相比,2013年全国胃癌疾病负担下降,各省份胃癌死亡率均下降,但各地差异较大,少数省份发病率略有升高,应深入研究我国及各地胃癌发病和死亡的影响因素,采取有效干预措施,对胃癌高危人群以及疾病负担高的地区加强防治,进一步降低胃癌疾病负担。
利益冲突 无| [1] International Agency for Research on Cancer, WHO. GLOBOCAN 2012:Estimated cancer incidence,mortality and prevalence worldwide in 2012[DB/OL].[2015-12-29]. http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx. |
| [2] 赵平,孔灵芝. 中国肿瘤死亡报告——全国第三次死因回顾抽样调查[M]. 北京:人民卫生出版社,2010:52-62. Zhao P,Kong LZ. Chinese cancer death report-the third cause of death review sampling survey[M]. Beijing:People's Medical Publishing House,2010:52-62. |
| [3] 赫捷,赵平,陈万青. 2012中国肿瘤登记年报[M]. 北京:军事医学科学出版社,2012:28-30. He J,Zhao P,Chen WQ. 2012 Chinese cancer registry annual report[M]. Beijing:Military Medical Science Press,2012:28-30. |
| [4] 国家卫生和计划生育委员会. 中国居民营养与慢性病状况报告(2015年)[M]. 北京:人民卫生出版社,2015:33-60. National Health and Family Planning Commission. Chinese nutrition and chronic diseases among residents report (2015)[M]. Beijing:People's Medical Publishing House,2015:33-60. |
| [5] GBD 2013 DALYs and HALE Collaborators,Murray CJ,Barber RM,et al. Global,regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries,1990-2013 quantifying the epidemiological transition[J]. Lancet,2015,386(10009):2145-2191. DOI:10.1016/S0140-6736(15)61340-X. |
| [6] Global Burden of Disease Cancer Collaboration,Fitzmaurice C,Dicker D,et al. The global burden of cancer 2013[J]. JAMA Oncol,2015,1(4):505-527. DOI:10.1001/jamaoncol.2015.0735. |
| [7] Zhou MG,Wang HD,Zhu J,et al. Cause-specific mortality for 240 causes in China during 1990-2013:a systematic subnational analysis for the Global Burden of Disease Study 2013[J]. Lancet,2016,387(10015):251-272. DOI:10.1016/S0140-6736(15)00551-6. |
| [8] Murray CJL,Ezzati M,Flaxman AD,et al. GBD 2010:design,definitions,and metrics[J]. Lancet,2012,380(9859):2063-2066. DOI:10.1016/S0140-6736(12)61899-6. |
| [9] GBD 2013 Mortality and Causes of Death Collaborators. Global,regional,and national age-sex specific all-cause and cause-specific mortality for 240 causes of death,1990-2013:a systematic analysis for the Global Burden of Disease Study 2013[J]. Lancet,2015,385(9963):117-171. DOI:10.1016/S0140-6736(14)61682-2. |
| [10] Lozano R,Naghavi M,Foreman K,et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010:a systematic analysis for the Global Burden of Disease Study 2010[J]. Lancet,2012,380(9859):2095-2128. DOI:10.1016/S0140-6736(12)61728-0. |
| [11] Murray CJ,Vos T,Lozano R,et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions,1990-2010:a systematic analysis for the Global Burden of Disease Study 2010[J]. Lancet,2012,380(9859):2197-2223. DOI:10.1016/S0140-6736(12)61689-4. |
| [12] Vos T,Flaxman AD,Naghavi M,et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010:a systematic analysis for the Global Burden of Disease Study 2010[J]. Lancet,2012,380(9859):2163-2196. DOI:10.1016/S0140-6736(12)61729-2. |
| [13] Marmot M,Atinmo T,Byers T,et al. Food,nutrition,physical activity,and the prevention of cancer:a global perspective (WCRF/AICR Expert Report)[R]. Washington,DC:AICR,2007. |
| [14] 张万岱,胡伏莲,萧树东,等. 中国自然人群幽门螺杆菌感染的流行病学调查[J]. 现代消化及介入诊疗,2010,15(5):265-270. DOI:10.3969/j.issn.1672-2159.2010.05.001. Zhang WD,Hu FL,Xiao SD,et al. Prevalence of Helicobacter pylori infection in China[J]. Mod Digest Int,2010,15(5):265-270. DOI:10.3969/j.issn.1672-2159.2010.05.001. |
| [15] Ma JL,Zhang L,Brown LM,et al. Fifteen-year effects of Helicobacter pylori,garlic,and vitamin treatments on gastric cancer incidence and mortality[J]. J Natl Cancer Inst,2012,104(6):488-492. DOI:10.1093/jnci/djs003. |
| [16] Malfertheiner P,Megraud F,O'Morain CA,et al. Management of Helicobacter pylori infection-the Maastricht Ⅳ/Florence Consensus Report[J]. Gut,2012,61(5):646-664. DOI:10.1136/gutjnl-2012-302084. |
| [17] Smyth EC,Capanu M,Janiigian YY,et al. Tobacco use is associated with increased recurrence and death from gastric cancer[J]. Ann Surg Oncol,2012,19(7):2088-2094. DOI:10.1245/s10434-012-2230-9. |
| [18] 中国疾病预防控制中心,中国疾病预防控制中心慢性非传染性疾病预防控制中心. 中国慢性病及其危险因素监测报告2010[M]. 北京:军事医学出版社,2012:34-48. Chinese Center for Disease Control and Prevention,National Center for Chronic and Noncommunicable Disease Control and Prevention. Report on chronic disease risk factor surveillance in China,2010[M]. Beijing:Military Medical Science Press,2012:34-48. |
| [19] 中华医学会消化内镜学分会,中国抗癌协会肿瘤内镜专业委员会. 中国早期胃癌筛查及内镜诊治共识意见(2014年,长沙)[J]. 中华消化杂志,2014,34(7):433-448. DOI:10.3760/cma.j.issn.0254-1432.2014.07.001. The Chinese Medical Association Branch of Digestive Endoscopy,Endoscopic Tumor Professional Committee of China Anti-Cancer Association. The consensus opinion of diagnosis and treatment of early gastric cancer screening and endoscopy (2014,Changsha)[J]. Chin J Digest,2014,34(7):433-448. DOI:10.3760/cma.j.issn.0254-1432.2014.07.001. |
| [20] Stewart BW,Wild CP. World cancer report 2014[M]. Lyon:International Agency for Research on Cancer,2014. |
| [21] 邹小农,孙喜斌,陈万青,等. 2003-2007年中国胃癌发病与死亡情况分析[J]. 肿瘤,2012,32(2):109-114. DOI:10.3781/j.issn.1000-7431.2012.02.006. Zou XN,Sun XB,Chen WQ,et al. Analysis of incidence and mortality of stomach cancer in China from 2003 to 2007[J].Tumor,2012,32(2):109-114. DOI:10.3781/j.issn.1000-7431. 2012.02.006. |
| [22] 裴泓波,蒲宏全,代敏,等. 金昌队列人群胃癌疾病负担研究[J].中华流行病学杂志,2016,37(3):316-320. DOI:10.3760/cma.j.issn.0254-6450.2016.03.004. Pei HB,Pu HQ,Dai M,et al. Disease burden of gastric cancer in Jinchang cohort[J]. Chin J Epidemiol,2016,37(3):316-320. DOI:10.3760/cma.j.issn.0254-6450.2016.03.004. |
| [23] Freedman ND,Derakhshan MH,Abnet CC,et al. Male predominance of upper gastrointestinal adenocarcinoma cannot be explained by differences in tobacco smoking in men versus women[J]. Eur J Cancer,2010,46(13):2473-2478. DOI:10.1016/j.ejca.2010.05.005. |
| [24] Camargo MC,Goto Y,Zabaleta J,et al. Sex hormones,hormonal interventions,and gastric cancer risk:ameta-analysis[J]. Cancer Epidemiol Biomarkers Prev,2012,21(1):20-38. DOI:10.1158/1055-9965.EPI-11-0834. |
| [25] Bertuccio P,Chatenoud L,Levi F,et al. Recent patterns in gastric cancer:a global overview[J]. Int J Cancer,2009,125(3):666-673. DOI:10.1002/ijc.24290. |
| [26] 天津市统计局. 天津统计年鉴1983-2015[M]. 北京:中国统计出版社,1983-2015. Tianjin Municipal Bureau of Statistics (NBS). Tianjin statistical yearbook 1983-2015[M]. Beijing:China Statistics Press,1983-2015. |