 2016, Vol. 37
2016, Vol. 37文章信息
- 曾新颖, 张梅, 李镒冲, 黄正京, 王丽敏.
- Zeng Xinying, Zhang Mei, Li Yichong, Huang Zhengjing, Wang Limin.
- 中国2011年城乡35岁及以上高血压患者社区管理现状及其效果影响因素分析
- Study on effects of community-based management of hypertension patients aged ≥35 years and influencing factors in urban and rural areas of China, 2010
- 中华流行病学杂志, 2016, 37(5): 612-617
- Chinese Journal of Epidemiology, 2016, 37(5): 612-617
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2016.05.005
-
文章历史
- 投稿日期: 2015-12-07




高血压的防控是世界慢病管理领域重要课题之一。近年来,我国城市和农村高血压的患病率均“节节攀升”,且城市和农村高血压患者的知晓率、治疗率和控制率仍处于较低的水平[1, 2],高血压的防控形势不容乐观。2006年国家心血管病研究中心在部分地区建立试点实施高血压社区规范化管理,2009年原卫生部将高血压规范化管理纳入国家基本公共卫生服务项目,免费面向全国高血压患者,社区高血压管理成效显著[3, 4, 5, 6, 7, 8, 9]。本研究通过分析2011年中国慢性病及其危险因素监测的数据,对我国城市和农村地区的社区高血压管理现状和效果进行分析,并进一步探索城市和农村地区影响高血压管理效果的因素,为全面的评估国家基本公共卫生服务社区高血压管理项目提供数据支持。
对象与方法1. 研究对象:2011年中国CDC慢性非传染性疾病预防控制中心对2010年中国慢性病及其危险因素监测人群进行追踪调查。2010年以全国疾病监测系统(DSPs)所覆盖的161个监测县(区)[10]及新疆生产建设兵团农二师为调查点,采用多阶段分层整群随机抽样的方法,抽取≥18岁常住居民(调查时的过去12个月内,在调查地区居住≥6个月)98 712名,其中14 343名被乡镇/社区级或以上医院确诊为高血压,抽样方法参见文献[11]。2011年10月对该人群进行随访,共随访到83 986人(其中高血压患者11 213人),随访率达85%。根据《国家基本公共卫生服务规范》的要求,辖区内≥35岁原发性高血压患者均纳入到高血压患者健康管理服务中。在2011年随访到的被乡镇/社区级或以上医院确诊为高血压的患者中,选取≥35岁且被纳入社区高血压管理的人群为本次研究的对象,共5 120例。
2. 血压测量:调查地区均统一使用由国家质检部门检验合格的欧姆龙HEM-7071或HEM-707A电子血压计。调查对象在测量前避免剧烈的运动、进食及饮用含咖啡因饮料;测量前不能吸烟,保持精神放松,排空膀胱。安静休息5 min,进行三次测量,两次间隔不少于1 min;取后两次测量值的平均值作为最终的血压值。
3. 调查内容:采用入户或集中面对面问卷调查的方法,收集调查对象的一般社会人口特征(年龄、性别、文化程度、婚姻状况、家庭经济收入等),高血压疾病史及并发症,高血压治疗情况,接受门诊、住院治疗情况,高血压患者参加社区高血压管理情况(参加时间、血压测量、用药指导、戒烟限酒指导、身体活动指导、膳食指导等)等内容。集中现场进行血压、身高、体重、腰围的测量。
4. 指标定义:①城乡及地区(东中西部):具体划分方法见文献[11];②高血压患者:被乡镇/社区级或以上医院确诊为高血压的患者;③高血压患者规范化管理[12]:参加社区管理的高血压患者同时得到基层医疗卫生机构医生所提供的每年至少4次的血压测量,及用药、膳食、身体活动、戒烟(从不吸烟者不需提供)和限酒(从不饮酒者不需提供)5个方面的指导建议;④高血压规范化管理率[13]:年内被管理高血压患者中,按规范化管理要求进行高血压管理者所占的比例;⑤高血压控制率[2]:在参加管理的高血压者中,血压得到有效控制者(SBP<140 mmHg和DBP<90 mmHg,1 mmHg=0.133 kPa)所占的比例;⑥超重和肥胖: BMI=体重(kg)/身高(m)2,24.0≤BMI<28.0时为超重,当BMI≥28.0时为肥胖;⑦吸烟者:调查时吸烟和以前曾经吸烟的人;⑧饮酒者:调查时过去12个月内饮酒者;⑨高血压家族史:父母有一方患有高血压;⑩并发症:包括脑卒中、冠心病、高血压性肾病和眼底动脉硬化。
5. 统计学分析:采用描述性分析和多因素分析方法。计量资料采用均数±标准差(x±s)来描述集中趋势和离散趋势,分类资料采用频数和加权构成比(%)来描述分布。计量资料组间差异比较采用复杂抽样设计的方差分析,分类资料组间比较采用复杂抽样设计的Rao-Scott χ2检验。估计不同特征人群的高血压控制率、sx及其95%CI值,采用泰勒级数线性化法,并考虑初级抽样单元的有限总体校正。影响因素分析均采用复杂抽样设计的非条件多因素logistic回归分析,以患者血压控制在SBP<140 mmHg和DBP<90 mmHg的范围为因变量(1=“是”,0=“否”);根据专业知识对自变量进行遴选,并对自变量进行共线性诊断,保证各自变量间不存在共线性,最终纳入模型的自变量有:年龄、性别、教育程度、人均年收入、东中西部地区、体重、腰围、吸烟、饮酒、高血压病程、高血压并发症、高血压合并糖尿病、管理方式、管理时限、血压测量、接受用药指导、接受膳食指导、接受身体活动指导,并计算了β值、OR值及其95%CI和P值。所有统计学检验均为双侧检验,以P<0.05为差异有统计学意义。统计分析使用SAS 9.3软件。
结 果1. 人口学指标及相关心血管病危险因素:调查结果显示,样本中≥35岁参加社区管理的高血压患者共5 120人,经复杂加权计算后,城市所占比例(37.46%)低于农村(62.54%);年龄越大者所占的比例越大,女性多于男性,但不同年龄和性别构成在城乡间的差异无统计学意义(P>0.05);城市高血压患者的教育程度和人均年收入均高于农村患者(P<0.05)。在相关心血管病危险因素方面,腰围为男性≥85 cm/女性≥80 cm的比例高达67.31%,39.05%的患者具有高血压家族史,46.67%的患者的病程在1~4年,13.83%的患者合并糖尿病,33.13%的患者血压控制未达标。腰围、高血压家族史、病程、合并糖尿病在城乡间的分布差异有统计学意义(P<0.05);吸烟、饮酒、体重、伴有并发症在城乡间的分布均差异无统计学意义(P>0.05)。见表 1。

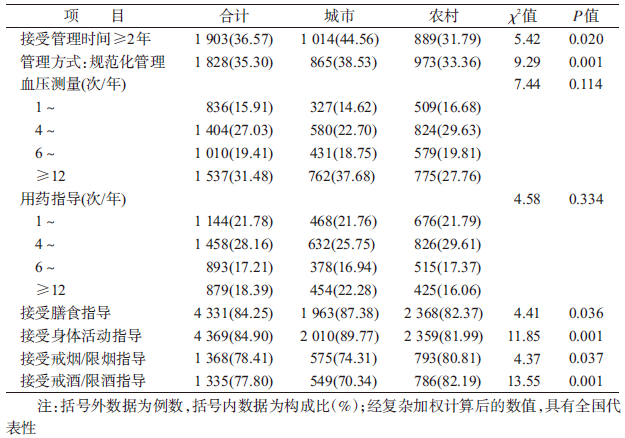
2. 接受管理服务的情况:≥35岁参加社区管理的高血压患者中,36.57%接受管理时间≥2年,35.30%接受规范化管理,均为城市(分别为44.56%和38.53%)高于农村(分别为31.79%和33.36%)(P<0.05)。在接受各项管理服务中,过去12个月内,分别有15.91%和21.78%的患者表示接受血压测量和用药指导服务的次数<4次,接受血压测量和用药指导服务情况的差异在城乡间差异无统计学意义(P>0.05);84.25%和84.90%的患者接受过基层卫生服务机构提供的膳食和身体活动的指导,且接受比例均是城市高于农村(P<0.05);在吸烟患者中,78.41%的患者接受过戒烟/限烟建议指导,在饮酒患者中,77.80%的患者接受过戒酒/限酒建议指导,均是农村高于城市患者(P<0.05),见表 2。
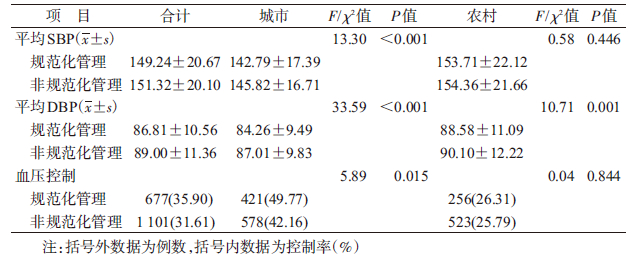
3. 我国城乡间规范化管理与非规范化管理患者的血压值及血压控制情况:参加社区管理的高血压患者中,在城市,接受规范化管理患者的平均SBP(142.79±17.39)mmHg和平均DBP(84.26±9.49)mmHg均低于接受非规范化管理患者(P<0.05);而在农村,不同管理方式对患者的平均SBP无影响(P>0.05),但影响平均DBP(P<0.05)。血压控制方面,在城市接受规范化管理的血压控制率(49.77%)高于接受非规范化管理患者(42.16%)(P<0.05);而在农村患者血压控制率接近(P>0.05),见表 3。
4. 城市、农村社区高血压患者血压控制影响因素的多因素分析:影响城市参加社区管理高血压患者的血压控制的因素包括受教育程度、人均年收入、体重、在过去12个月内接受的管理方式、血压测量次数、用药指导次数和是否接受身体活动指导(P<0.05),见表 4;而影响农村参加社区管理患者的血压控制率的因素包括人均年收入、体重、高血压家族史、服药知晓情况、在过去12个月内接受用药指导次数以及是否接受膳食指导,见表 5。


对社区管理的高血压患者血压控制情况的分析发现,规范化管理的血压控制率为35.90%,其中城市血压控制率(49.77%)远高于农村(26.31%)。2010年我国城市和农村的成年人高血压控制率分别为22.9%和13.7%[2],李园等[14]在中国8省开展的研究显示管理满1年的城市和农村的高血压患者血压控制率分别62.0%和36.6%,2006年加拿大、2009-2010年美国社区高血压患者的控制率均在60%以上[15, 16]。与国外社区高血压控制效果相比较,我国的社区高血压规范化管理措施,特别是在农村地区,并未充分发挥出控制血压的效果。
本研究发现,农村参加社区管理的高血压患者的规范化管理率、接受膳食指导和身体活动指导的比例均低于城市患者,与李园等[14]报道一致。国外开展的人群高血压健康管理的研究显示[17, 18, 19, 20, 21],血压监测、用药和健康生活方式指导可有效改善危险因素水平和血压状况。本研究结果显示,在农村经济收入水平、体重、高血压家族史是影响血压控制的危险因素,这与国外研究一致[22, 23, 24];而在城市社区高血压管理服务成为影响高血压患者血压控制的主要因素,可较好改善血压。农村基层卫生服务机构对社区高血压管理的各项服务的实施力度不够,农村基层医务人员未按照《中国高血压防治指南(基层版)》和《国家基本公共卫生服务规范(2011版)》中的要求向患者提供管理服务,所以与城市相比,农村社区高血压管理服务的质量还有一定差距。
总之,我国城市社区高血压规范化管理的效果明显好于农村,但总体效果不佳。因此,通过多部门参与、多种形式的健康教育和健康促进活动提高高血压患者的健康意识和行为改变,特别是在农村地区,普及科学、高质量的社区高血压管理服务,增加基层卫生服务机构人员编制,加强基层卫生服务机构专业技术人员的慢病管理能力和患者自我管理能力是社区高血压患者管理的当务之急。
利益冲突 无| [1] 李立明. 中国居民营养与健康状况调查报告之四——2002高血压[M]. 北京:人民卫生出社,2008. Li LM. Report of China nutrition and health status Ⅳ:2002 Hypertension[M]. Beijing:People's Medical Publishing House,2008. |
| [2] 中国疾病预防控制中心,中国疾病预防控制中心慢性非传染性疾病预防控制中心. 中国慢性病及其危险因素监测报告(2010)[M]. 北京:军事医学科学出版社,2012. Chinese Center for Disease Control and Prevention,National Center for Chronic and Non-communicable Disease,Chinese Center of Disease Control and Prevention. Report on Chronic Disease Risk Factor Surveillance in China (2010)[M]. Beijing:Military Medical Science Press,2012. |
| [3] 张彦琦,张玲,易东,等. 重庆市高血压和糖尿病患者社区健康管理现状及影响因素研究[J]. 中国全科医学,2015,18(28):3473-3477. DOI:10.3969/j.issn.1007-9572.2015.28.021. Zhang YQ,Zhang L,Yi D,et al. Status of and influencing factors for the community health management of hypertensive and diabetic patients in Chongqing[J]. Chin Gen Pract,2015,18(28):3473-3477. DOI:10.3969/j.issn.1007-9572.2015.28. 021. |
| [4] 王文. 我国基层高血压防治的现状及对策//第二届国际心血管热点论坛论文集[C]. 北京:中华医学会,2010. Wang W. Status and study on prevention and treatment of grass hypertension in China//The second International Forum on the topic of cardiovascular[C]. Beijing:Chinese Medical Association,2010. |
| [5] 应慧星. 社区高血压规范化管理及效果探讨[J]. 上海预防医学,2012,24(6):330-331. DOI:10.3969/j.issn.1004-9231.2012. 06.019. Ying HX. Effect of standardized management of hypertension in community[J]. Shanghai J Prev Med,2012,24(6):330-331. DOI:10.3969/j.issn.1004-9231.2012.06.019. |
| [6] 凌瑞杰,刘烽,徐莲,等. 湖北"高血压社区规范化管理"项目三年工作总结//全国心血管病社区防治工作经验交流会论文集[C]. 北京:中华医学会,2009. Ling RJ,Liu F,Xu L,et al. Work summary about standardized management of hypertension in community for three years in Hubei province//National cardiovascular community prevention and control work experience exchange meeting[C]. Beijing:Chinese Medical Association,2009. |
| [7] 徐亮,李芳健,王文,等. 广州市高血压社区规范化管理项目实施效果初步评价[J]. 中国卫生事业管理,2009,26(8):564-565. DOI:10.3969/j.issn.1004-4663.2009.08.029. Xu L,Li FJ,Wang W,et al. Evaluating the effect of implementing standardized community management project of hypertension control in Guangzhou[J]. Chin Health Serv Manag,2009,26(8):564-565. DOI:10.3969/j.issn.1004-4663.2009. 08.029. |
| [8] 孙纪新,朱俊卿,唐丽娟,等. 河北省高血压社区规范化管理患者血压控制效果[J]. 河北医药,2012,34(19):2998-2999. DOI:10.3969/j.issn.1002-7386.2012.19.076. Sun JX,Zhu JQ,Tang LJ,et al. The effect of community standardized management of hypertension control in Hebei province[J]. Hebei Med J,2012,34(19):2998-2999. DOI:10.3969/j.issn.1002-7386.2012.19.076. |
| [9] Chen XJ,Gao XL,You GY,et al. Higher blood pressure control rate in a real life management program provided by the community health service center in China[J]. BMC Public Health,2014,14:801. DOI:10.1186/1471-2458-14-801. |
| [10] 周脉耕,姜勇,黄正京,等. 全国疾病监测点系统的调整与代表性评价[J]. 疾病监测,2010,25(3):239-244. DOI:10.3784/j.issn.1003-9961.2010.03.023. Zhou MG,Jiang Y,Huang ZJ,et al. Adjustment and representativeness evaluation of national disease surveillance points system[J]. Dis Surveill,2010,25(3):239-244. DOI:10.3784/j.issn.1003-9961.2010.03.023. |
| [11] 赵文华,宁光. 2010年中国慢性病监测项目的内容与方法[J]. 中华预防医学杂志,2012,46(5):477-499. DOI:10.3760/cma.j.issn.0253-9624.2012.05.023. Zhao WH,Ning G. Contents and methods of Chinese chronic disease surveillance program in 2010[J]. Chin J Prev Med,2012,46(5):477-499. DOI:10.3760/cma.j.issn.0253-9624.2012.05. 023. |
| [12] 曾新颖,王丽敏,王临虹,等. 中国35岁以上高血压患者社区管理的现状研究[J]. 中华预防医学杂志,2013,47(11):1014-1019. DOI:10.3760/cma.j.issn.0253-9624.2013.11.010. Zeng XY,Wang LM,Wang LH,et al. The study of management of hypertensive people aged 35 and over in communities in China[J]. Chin J Prev Med,2013,47(11):1014-1019. DOI:10.3760/cma.j.issn.0253-9624.2013.11.010. |
| [13] 卫生部. 国家基本公共卫生服务规范(2011年版)[M]. 北京:中国卫生出版社,2011. Ministry of Health. Norm of national basic public health services (2011)[M]. Beijing:People's Medical Publishing House,2011. |
| [14] 李园,任多富,丁萍飞,等. 中国8省(自治区)高血压和2型糖尿病患者健康管理服务实施现状[J]. 中华流行病学杂志,2014,35(1):35-39. DOI:10.3760/cma.j.issn.0254-6450.2014.01.009. Li Y,Ren DF,Ding PF,et al. Evaluation on programs regarding the community-based management of hypertension and type 2 diabetes mellitus patients in eight provinces,China[J]. Chin J Epidemiol,2014,35(1):35(1):35-39. DOI:10.3760/cma.j.issn.0254-6450.2014.01.009. |
| [15] McInnis NH,Fodor G,Moy Lum-Kwong M,et al. Antihypertensive medication use and blood pressure control:a community-based cross-sectional survey (ON-BP)[J]. Am J Hypertens,2008,21(11):1210-1215. DOI:10.1038/ajh.2008.269. |
| [16] Guo FJ,He D,Zhang W,et al. Trends in prevalence,awareness,management,and control of hypertension among United States adults,1999 to 2010[J]. J Am Coll Cardiol,2012,60(7):599-606. DOI:10.1016/j.jacc.2012.04.026. |
| [17] McAlister A,Puska P,Salonen JT,et al. Theory and action for health promotion illustrations from the North Karelia Project[J]. Am J Public Health,1982,72(1):43-50. DOI:10.2105/AJPH. 72.1.43. |
| [18] Winkleby MA. The future of community-based cardiovascular disease intervention studies[J]. Am J Public Health,1994,84(9):1369-1372. DOI:10.2105/AJPH.84.9.1369. |
| [29] Winkleby MA,Taylor CB,Jatulis D,et al. The long-term effects of a cardiovascular disease prevention trial:the Stanford Five-City Project[J]. Am J Public Health,1996,86(12):1773-1779. DOI:10.2105/AJPH.86.12.1773. |
| [20] Writing Group of the PREMIER Collaborative Research Group. Effects of comprehensive lifestyle modification on blood pressure control:main results of the PREMIER clinical trial[J]. JAMA,2003,289(16):2083-2093. DOI:10.1001/jama.289.16. 2083. |
| [21] Committee on Public Health Priorities to Reduce and Control Hypertension in the U.S. Population,Institute of Medicine. A population-based policy and systems change approach to prevent and control hypertension[M]. New York:National Academies Press,2010. |
| [22] 杨德华,柴云,汪文新,等. 成都市社区卫生服务中高血压控制率及其影响因素分析[J]. 现代预防医学,2010,37(6):1007-1011. Yang DH,Chai Y,Wang WX,et al. Analysis of the factors affecting the control rate of hypertension in community health service in Chengdu[J]. Mod Prev Med,2010,37(6):1007-1011. |
| [23] Hu G,Barengo NC,Tuomilehto J,et al. Relationship of physical activity and body mass index to the risk of hypertension:a prospective study in Finland[J]. Hypertension,2004,43(1):25-30. DOI:10.1161/01.HYP.0000107400.72456.19. |
| [24] Yusuf S,Hawken S,Ôunpuu S,et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study):case-control study[J]. Lancet,2004,364(9438):937-952. DOI:10.1016/S0140-6736(04)17018-9. |