 2016, Vol. 37
2016, Vol. 37文章信息
- 李幸乐, 李懿, 张白帆, 隋美丽, 潘静静, 陈志娟, 程宁宁, 杜燕华, 卫海燕, 许汴利, 黄学勇.
- Li Xingle, Li Yi, Zhang Baifan, Sui Meili, Pan Jingjing, Chen Zhijuan, Cheng Ningning, Du Yanhua, Wei Haiyan, Xu Bianli, Huang Xueyong.
- 河南省2014年手足口病重症病例病原学分析
- Etiology study on severe cases caused by hand-foot-mouth disease in children from Henan province, 2014
- 中华流行病学杂志, 2016, 37(4): 568-571
- Chinese Journal of Epidemiology, 2016, 37(4): 568-571
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2016.04.026
-
文章历史
- 收稿日期: 2015-08-20




2. 450052 郑州大学公共卫生学院
2. College of Public Health, Zhengzhou University, Zhengzhou 450052, China
手足口病(HFMD)是以肠道病毒(EV)71型(EV71)、柯萨奇病毒A组16型(Cox A16)为主的多种肠道病毒引起的全球性常见传染病。自2008年以来在我国内陆地区呈现不同程度的流行态势,近年研究显示HFMD的病原谱结构已然改变,柯萨奇病毒A组6型(Cox A6)和A组10型(Cox A10)感染导致的HFMD在某些地区呈现上升趋势[1, 2, 3, 4]。河南省是我国HFMD影响最为严重的省份之一。为准确掌握河南省HFMD病原谱结构与HFMD间的关系,开展本此研究,结果报告如下。
材料与方法1. 样本采集: 以郑州市某儿童医院作为监测点,采集2014年4-6月诊断为HFMD病例的粪便标本,于24 h内-20 ℃或以下冻存保存,冷链运送至河南省CDC。HFMD诊断标准以国家卫生和计划生育委员会制定的“手足口病诊疗指南(2010年版)”及《全国手足口病监测方案(2014年版)》作为依据。纳入标准:①临床诊断HFMD病例;②年龄≤5岁;③发病时间≤21 d。排除标准:①先天性疾病患儿;②急、慢性肝炎患儿;③其他疾病引起的心脏损害;④合并其他肠道疾病的患儿。
2. 样本处理和病原学检测: 采用含2%青、链霉素,1%氯仿的PBS将粪便标本制成20%的混悬液,825×g离心20 min,吸取上清液用于病原学检测。病毒核酸提取采用德国Qiagen公司的QIAamp Viral mini试剂盒,反转录采用宝生物工程(大连)有限公司的PrimeScript® 1st Strand cDNA Synthesis Kit 试剂盒,核酸检测采用江苏默乐三重荧光PCR检测试剂盒。病毒培养采用RD、Hep-2、Vero细胞,阳性分离物经核酸提取、反转录后采用VP1区特异性引物222~292扩增[5],扩增产物送南京金斯瑞生物科技有限公司测序。
3. 统计学分析: 采用DNAStar 7.0软件拼接、校正测序结果,同时采用Clustal 1.81和Mega 4.1软件进行序列分析;采用Excel表格整理数据,SPSS 17.0软件进行相关统计学分析,采用 χ2检验对HFMD病例病原感染率和构成比进行比较,以P<0.05为差异有统计学意义。
结 果1. 病例概况:2014年4-6月共收治 244例HFMD。其中重症组109例,死亡3例;轻症组135例。重症组和轻症组病例在发病年龄上的差异有统计学意义(P=0.036),重症组病例的发病年龄(1.69岁±0.78岁)小于轻症组病例(2.10岁±1.62岁)。两组在性别上的差异无统计学意义( χ2=2.009,P=0.156),男性155例,女性89例,性别比为1.74:1。
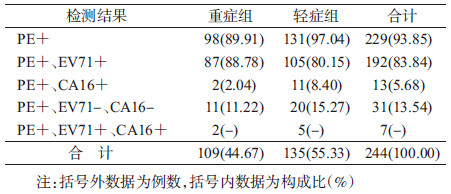
2. 病原学检测:244例中有229例为EV,通用引物RT-PCR阳性。其中EV71阳性者192例,Cox A16阳性者13例,其他EV阳性者31例,其中Cox A10感染19例(表 1)。EV71感染致8例发生心肺功能衰竭,2例死亡;Cox A10感染致1例发生心肺功能衰竭、死亡。重症组和轻症组EV感染率统计学分析结果为χ2=5.312,P=0.021,重症组EV感染率低于轻症组。采用Fisher精确概率法对两组EV71、Cox A16和其他EV感染构成比进行统计学比较,P=0.048,表明两组病例3种病原构成的差异有统计学意义。EV71与Cox A10感染致心肺功能衰竭发生率的差异无统计学意义(χ2=0.051,P=0.821),EV71与Cox A10感染致死率的差异无统计学意义(χ2=2.198,P=0.138)。EV71感染致心肺功能衰竭发生率与EV71感染致死率的差异也无统计学意义(χ2=3.696,P=0.055)。
3. Cox A10分离株遗传进化分析:经NCBI网站筛选有代表性的Cox A10 VP1基因同源区段核苷酸序列和本研究中病例感染的Cox A10 VP1基因核苷酸序列共同进行系统进化分析,以Cox A6(GenBank序列号:JN797598)作为外部组。进化分析结果显示(图 1):Cox A10病毒可以划分为至少6个基因组。河南省2014年分离株位于同一分支,同属于基因6型Cox A10病毒。

|
| 图 1 2014年河南省Cox A10分离株与各型代表株的VP1基因(336 nt)系统发生树 |
2014年河南省Cox A10分离株来自全省,各地均有不同程度的分布,核苷酸和氨基酸同源性分别为94.3%~99.7%和96.3%~100.0%,与2010年河南省Cox A10分离株的核苷酸和氨基酸同源性分别为93.0%~96.9%和96.3%~100.0%。与基因6型其他Cox A10毒株的核苷酸和氨基酸同源性分别为92.3%~100.0%和97.2%~100.0%。
讨 论本文显示重症组病例EV感染率低于轻症组,提示该医疗机构在HFMD临床诊断方面执行标准相对宽松。这种现象的出现是由于HFMD对社会影响大、医疗机构病原学和血清学检测相对临床诊断滞后所致。河南省HFMD以2-7月高发,4-5月发病达全年峰值[6]。该医疗机构在此期间采用的这种执行方式对HFMD病例的诊治具有一定的积极作用。
2014年4-6月HFMD病原学分析显示:EV71感染构成比超过80%,重症组EV71感染构成比达到88.78%,EV71感染致心肺功能衰竭发生率与病死率的差异无统计学意义。既往研究显示:EV71感染的病死率显著下降,而其基因亚型和毒力并未发生改变[1, 2, 3, 4, 6],这是医疗机构诊治水平提高的结果。本文中EV71感染致心肺功能衰竭发生率与病死率的差异无统计学意义与实际情况存在偏差,可能是样本量少统计误差所致。EV71仍然是HFMD尤其是重症病例最主要的病原,且EV71感染致心肺功能衰竭发生率高,因此加快EV71疫苗的生产具有重要的社会价值[7, 8]。
与既往研究相似,现阶段EV71是HFMD病原谱中最为主要的病原,其次为非EV71非Cox A16的其他EV,而Cox A16所占比例减少[9, 10]。本文非EV71非Cox A16的其他EV基因型按感染比依次为Cox A10、Cox A6、Cox A4、Cox B2、Cox B5、ECHO6和EV75。其中,Cox A10的感染构成比仅次于EV71,成为HFMD病原谱中的第二位。Cox A10感染导致1例重症HFMD患儿死亡。对Cox A10 VP1区段的遗传进化分析显示:2014年河南省Cox A10分离株处于同一进化分支,与2010年河南省Cox A10分离株高度同源,与我国内陆大部分地区流行的Cox A10病毒株同属于基因6型。表明基因6型Cox A10病毒在河南省长期存在,广泛分布,与国内其他省份的Cox A10处于共循环状态,未发生大的变异及重组。鉴于Cox A10感染构成比显著升高,且可以导致心肺功能衰竭甚至死亡,对非EV71非Cox A16的其他EV尤其是Cox A10的监测有必要再加强。
利益冲突 无| [1] 王英,何小周,赵俊伟,等. 2008-2010年全国报告手足口病死亡水平及死亡病例分析[J]. 疾病监测,2011,26(6):424-426. DOI:10.3784/j.issn.1003-9961.2011.06.003. Wang Y,He XZ,Zhao JW,et al. Mortality and death cases of hand foot and mouth disease reported in China,2008-2010[J].Dis Surveill,2011,26(6):424-426. DOI:10.3784/j.issn.1003-9961.2011.06.003. |
| [2] Lu QB,Zhang XA,Wo Y,et al. Circulation of coxsackievirus A10 and A6 in hand-foot-mouth disease in China,2009-2011[J]. PLoS One,2012,7(12):e52073. DOI:10.1371/journal.pone.0052073. |
| [3] 查杰,封琦,马智龙. 2010-2013年江苏省泰州市非EV71和非Cox A16型手足口病肠道病毒病原谱及Cox A6 VP1基因特征分析[J]. 中华流行病学杂志,2014,35(10):1181-1182. DOI:10.3760/cma.j.issn.0254-6450.2014.10.024. Zha J,Feng Q,Ma ZL. The pathogenic spectrum of the enteroviruses for non-EV71 and Cox A16 for HFMD in Taizhou between 2010 and 2013 and the VP1 gene character analysis for coxsackievirus A6[J]. Chin J Epidemiol,2014,35(10):1181-1182. DOI:10.3760/cma.j.issn.0254-6450.2014.10.024. |
| [4] Tian HF,Zhang Y,Sun Q,et al. Prevalence of Multiple enteroviruses associated with hand,foot,and mouth disease in Shijiazhuang city,Hebei Province,China:outbreaks of coxsackieviruses A10 and B3[J]. PLoS One,2014,9(1):e84233. DOI:10.1371/journal.pone.0084233. |
| [5] Oberste MS,Nix WA,Maher K,et al. Improved molecular identification of enteroviruses by RT-PCR and amplicon sequencing[J]. J Clin Virol,2003,26(3):375-377. DOI:10. 1016/S1386-6532(03)00004-0. |
| [6] 黄学勇,康锴,许玉玲,等. 2008-2011年河南省手足口病患儿病原学监测结果[J]. 中华预防医学杂志,2012,46(10):883-887. DOI:10.3760/cma.j.issn.0253-9624.2012.10.005. Huang XY,Kang K,Xu YL,et al. Etiology surveillance of hand-foot-mouth disease in Henan province between 2008 and 2011[J]. Chin J Prev Med,2012,46(10):883-887. DOI:10. 3760/cma.j.issn.0253-9624.2012.10.005. |
| [7] Li JX,Mao QY,Liang ZL,et al. Development of enterovirus 71 vaccines:from the lab bench to Phase Ⅲ clinical trials[J]. Expert Rev Vaccines,2014,13(5):609-618. DOI:10.1586/14760584.2014.897617. |
| [8] Zhu FC,Meng FY,Li JX,et al. Efficacy,safety,and immunology of an inactivated alum-adjuvant enterovirus 71 vaccine in children in China:a multicentre,randomised,double-blind,placebo-controlled,phase 3 trial[J]. Lancet,2013,381(9882):2024-2032. DOI:10.1016/S0140-6736(13)61049-1. |
| [9] 杨赫,陶泽新,王海岩,等. 手足口病患儿柯萨奇病毒A10型山东地方株VP1区基因特征分析[J]. 中华传染病杂志,2010,28(7):385-389. DOI:10.3760/cma.j.issn.1000-6680.2010.07.001. Yang H,Tao ZX,Wang HY,et al. The genetic characterization of VP1 region of Coxsackie virus A10 isolated from hand,foot and mouth disease cases in Shandong Province of China[J]. Chin J Infect Dis,2010,28(7):385-389. DOI:10.3760/cma.j.issn.1000-6680.2010.07.001. |
| [10] 甄若楠,张颖,谢华萍,等. 2010-2012年广州市柯萨奇病毒A4、A10型VP1基因特征分析[J]. 中华预防医学杂志,2014,48(6):445-450. DOI:10.3760/cma.j.issn.0253-9624.2014.06.005. Zhen RN,Zhang Y,Xie HP,et al. Sequence analysis of VP1 region of coxsackievirus A4 and coxsackievirus A10 in Guangzhou city,2010-2012[J]. Chin J Prev Med,2014,48(6):445-450. DOI:10.3760/cma.j.issn.0253-9624.2014.06.005. |