 2016, Vol. 37
2016, Vol. 37文章信息
- 陈启才, 肖娟, 张鹏鹏, 陈莉莉, 陈潇潇, 王束玫.
- Chen Qicai, Xiao Juan, Zhang Pengpeng, Chen Lili, Chen Xiaoxiao, Wang Shumei.
- 血清直接胆红素与代谢综合征及其组分关系的研究
- Association between serum direct bilirubin with metabolic syndrome and its components based on a longitudinal health check-up study
- 中华流行病学杂志, 2016, 37(4): 486-490
- Chinese Journal of Epidemiology, 2016, 37(4): 486-490
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2016.04.009
-
文章历史
- 收稿日期: 2015-09-01




2. 250012 济南, 山东大学公共卫生学院流行病学系;
3. 300457 天津出入境检验检疫局;
4. 310051 杭州, 浙江省疾病预防控制中心
2. Department of Epidemiology, School of Public Health, Shandong University, Jinan 250012, China;
3. Tianjin Entry-Exit Inspection and Quarantine Bureau, Tianjin 300457, China;
4. Zhejiang Provincial Center for Disease Control and Prevention, Hangzhou 310051, China
胆红素作为机体内源性抗氧化物质,其水平适量升高可降低动脉粥样硬化、高血压、冠心病等疾病的发病风险[1, 2, 3]。代谢综合征(MS)的发生与机体过氧化导致的慢性系统性炎症反应有关[4]。因此,适量的血清胆红素水平可能一定程度上保护机体并对抗MS的发生。
目前多数研究仅探讨血清总胆红素与MS的关系,而不同的胆红素亚型对MS的发生作用可能不同[5, 6]。由于血清直接胆红素(DBIL)更易于释放并作用于机体靶点,与MS的关系可能更为显著[7]。目前国内外鲜有关于DBIL与MS关系的研究,且已有的多为横断面研究,结果也存在争议[8, 9]。同时,DBIL与MS 的4个组分(超重/肥胖、高血压、高脂血症和高血糖)关系,现有结论并不一致[8, 9]。为此本研究选用山东省某市2006-2011年纵向职工体检资料,构建动态体检队列,采用广义估计方程(GEE)模型[10]分析血清DBIL与MS发生的关系。
对象与方法1. 研究对象:源自2006年1月至2011年12月山东省某三甲医院健康体检资料构建的动态体检队列。纳入标准:①首次体检未患有MS者;②至少有2次完整体检记录者。排除标准:①患严重的系统性疾病如充血性心力衰竭、肾衰竭等;②肝功能异常(AST≥100 U/L或ALT≥100 U/L);③内生肌酐清除率(creatinine clearance rate,Ccr)<50 ml/min或血尿素氮(BUN)水平超过代偿期(BUN>9 mmol/L);④血清总胆红素异常(>20.5 μmol/L)和血清DBIL异常(>6.8 μmol/L);⑤患肝病。本研究5年随访中共纳入5 258名24~75岁研究对象,平均随访次数3.55次。体检时按统一标准询问人口学资料、吸烟和饮酒等日常行为、疾病史(心血管疾病、MS、肾病和肝病等)、药物使用史(抗高血压药物、抗血脂紊乱药物、抗糖尿病药物和肝毒性药物)等。
2. 调查方法:体格检查包括测量身高、体重和计算BMI,静坐血压(SBP和DBP)测定2次,取均值。实验室检测指标测定包括FPG(葡萄糖氧化酶法)、TG(酶化学法)、BUN和血尿酸(UA),采用赖氏法测定ALT、AST和谷酰转肽酶(GGT),使用重氮法测定血清胆红素水平。
3. 定义及诊断标准:每天吸卷烟≥1支,连续或累计吸烟≥6个月,且在调查前30 d内仍吸烟者定义为吸烟[11]。不论是白酒、啤酒、葡萄酒或黄酒等,只要平均每周饮用1次即定义为饮酒者(逢年过节仅饮用1次者除外)[12]。MS诊断标准依据中华医学会糖尿病分会制定版(2004)[13],即具备以下4项组成成分中的3项或全部者即可诊断为MS。①超重和(或)肥胖:BMI≥25.0 kg/m2;②高血糖:FPG≥6.1 mmol/L(110 mg/dl)和(或)餐后2 h血糖≥7.8 mmol/L,和(或)已确诊糖尿病者;③高血压:SBP/DBP≥140/90 mmHg(1 mmHg=0.133 kPa),和(或)已确诊高血压者;④血脂紊乱:空腹TG≥1.7 mmol/L(110 mg/dl),和(或)男性 HDL-C<0.9 mmol/L,女性HDL-C<1.0 mmol/L。
4. 统计学分析:数值变量符合正态分布,采用 x±s表示;分类变量采用百分比表示。采用GEE模型分析随时间变化的DBIL水平与MS发生的关系。将年龄作为GEE模型中的时间尺度变量。在动态体检队列中,将进入队列的时间定义为研究对象第一次体检的年龄,结束时间为研究对象诊断为MS的年龄或研究对象最后一次体检的年龄。将单因素GEE模型筛选P<0.10的变量作为协变量,采用多元GEE模型分析扣除协变量后,获得血清DBIL水平与MS的关系,用RR值及95%CI表达[表示DBIL每升高1 μmol/L,MS发病风险的改变量(%)]。GEE模型采用“Logit”为连接函数。统计学分析采用SAS 9.1软件。
结 果1. 一般特征:该体检队列共有831名新发MS患者,发病率为6.43/100人年,其特征见表 1。

2. DBIL与MS及其组分关系:采用单因素GEE分析血清DBIL水平与MS关系显示,DBIL水平的升高与MS的发生呈负相关;ALT、AST、GGT、BUN、血白细胞计数(WBC)、年龄、吸烟、饮酒和时间与MS的发生呈正相关;与男性相比,女性与MS的RR值为0.332(P<0.001),见表 2。
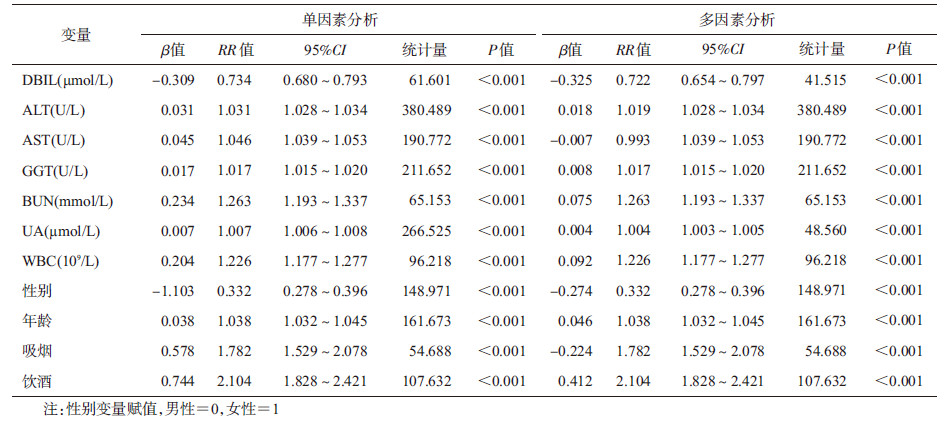
采用多因素GEE模型分析血清DBIL水平与MS的关系(表 2),在调整了年龄、性别、吸烟、饮酒、ALT、AST、GGT、UA、BUN和WBC等相关因素后,在血清DBIL水平正常的调查对象中,DBIL水平的升高与MS的发生呈负相关,血清DBIL每升高1 μmol/L,MS的发病风险降低22.8%(RR=0.772,95%CI:0.654~0.797)。采用多因素GEE模型分析血清DBIL水平与MS的4个组分关系,发现随着血清DBIL水平的升高,超重/肥胖、高脂血症的发病风险也依次降低,RR值分别为0.919(95%CI:0.878~0.962)和0.737(95%CI:0.704~0.772)。而血清DBIL水平与高血压和高血糖无明显相关关系(表 3)。同样采用多因素GEE模型分析不同性别和年龄血清DBIL水平与MS的关系,结果显示:与男性相比,女性的DBIL水平与MS的负相关关系更为显著,女性RR=0.483(95%CI:0.352~0.663),男性RR=0.755(95%CI:0.681~0.837);<55岁者中,血清DBIL水平的升高与MS的发病呈负相关(表 4)。


本研究显示,正常人群血清DBIL水平升高与MS的发生呈负相关,其RR值依性别、年龄不同而有差异。与MS各组分关系分析中,随着DBIL水平的升高,超重/肥胖、高脂血症的发病风险逐渐降低。
本研究采用纵向体检资料,构建动态队列。以往的队列研究多根据基线研究因素的水平将研究对象分为暴露组和非暴露组,并分析其与结局事件发生的关系,可能忽视了随访过程中研究因素水平的波动。而本研究构建动态体检队列,资料包含研究对象多次体检记录,采用常用于重复测量资料GEE模型,将基线及每一随访年的实际DBIL测量水平与MS的关系全部纳入模型分析,充分考虑到DBIL水平随时间的动态变化,更利于准确真实估计血清DBIL与MS发生的关系。
MS是慢性血管性疾病的重要危险因素[14]。已有的研究发现,血清总胆红素水平与MS的发生成负相关[15]。但多数研究仅探讨血清总胆红素与MS的关系,较少涉及其亚型(DBIL和IBIL)与MS的相关性。本研究以DBIL探讨其与MS的关系。Hwang和Kim[8]研究韩国人群发现,血清DBIL水平与MS呈负相关,而IBIL与MS关系的差异无统计学意义。与IBIL相比,DBIL与MS的关系为何更为密切?有研究表明,血清DBIL较之其他胆红素亚型,与清蛋白的结合更为松散,因而更易于分离并作用于靶器官和靶分子[7]。
Boon等[1]的实验研究显示,DBIL可以有效抑制LDL-C的过氧化。本研究亦发现血清DBIL与高脂血症的负相关关系最为显著,这与Choi等[16]和Jo等[9]的研究结果相类似。本研究发现,血清DBIL水平与肥胖/超重的发生呈负相关,Jenko-Pra?nikar等[17]的研究结果也发现肥胖人群中血清DBIL水平低于正常体重者。同时,血清DBIL水平与高血压的发病无明显相关关系,这与Wang和Bautista[18]的研究结论相反,可对此做更深入细致的后续研究。
Lin等[19]发现在儿童青少年中血清胆红素与MS和胰岛素抵抗呈负相关。本研究亦发现较低年龄组(≤54岁)血清DBIL与MS的负相关关系显著,而在高年龄组中(≥55岁)DBIL与MS关系的差异无统计学意义。其可能的原因是,中青年人的MS以肥胖为主(<55岁MS患者中超重/肥胖的比例为95.4%),可能仅增加了血管内皮的氧化应激,未形成既定的胰岛素抵抗和系统性炎症反应。此时,胆红素针对此类早期代谢紊乱的组织可以有效地发挥其抗氧化作用。本研究还发现女性较高水平的DBIL对于MS发生的保护作用强于男性,这可能由不同性别生活方式、性激素和血清DBIL的差异所致。其结果与Troughton等[20]的发现不一致,可能与该研究未排除肝脏疾病患者有关。
本文存在不足。如体检资料无法获取研究对象准确的更年期年龄,研究中对年龄组的划分是依据现有国内流行病学资料[21],后续研究应加以改进。
总之,本研究基于大样本动态体检队列,发现DBIL水平的升高与MS及其组分中的超重/肥胖、高脂血症的负相关关系显著,可使<55岁男女性研究对象MS患病风险降低,并为寻找更为灵敏的MS生物学指标提供依据。
利益冲突 无| [1] Boon AC,Hawkins CL,Coombers JS,et al. Bilirubin scavenges chloramines and inhibits myeloperoxidase-induced protein/lipid oxidation in physiologically relevant hyperbilirubinemicserum[J]. Free RadicalBiol Med,2015,86:259-268. DOI:10.1016/j.freeradbiomed.2015.05.031. |
| [2] Akboga MK,Canpolat U,Sahinarslan A,et al. Association of serum total bilirubin level with severity of coronary atherosclerosis is linked to systemic inflammation[J]. Atherosclerosis,2005,240(1):110-114. DOI:10.1016/j.atherosclerosis.2015.02.051. |
| [3] Targher G,Byrne CD. Circulating markers of liver function and cardiovascular disease risk[J]. Arterioscler Thromb Vasc Biol,2015,35(11):2290-2296. DOI:10.1161/ATVBAHA.115.305235. |
| [4] Liao M,Huang L,Mao Y,et al. Serum osteocalcin is associated with inflammatory factors in metabolic syndrome:a population-based study in Chinese males[J]. Mediators Inflamm,2015,2015:683739. DOI:10.1155/2015/683739. |
| [5] Oda E,Aizawa Y. Total bilirubin is inversely associated with metabolic syndrome but not a risk factor for metabolic syndrome in Japanese men and women[J]. Acta Diabetol,2013,50(3):417-422. DOI:10.1007/s00592-012-0447-5. |
| [6] Wu YH,Li M,Xu M,et al. Low serum total bilirubin concentrations are associated with increased prevalence of metabolic syndrome in Chinese[J]. J Diabetes,2011,3(3):217-224. DOI:10.1111/j.1753-0407.2011.00138.x. |
| [7] Nakagami T,Toyomura K,Kinoshita T,et al. A beneficial role of bile pigments as an endogenous tissue protector:anti-complement effects of biliverdin and conjugated bilirubin[J]. Biochim Biophys Acta,1993,1158(2):189-193. DOI:10.1016/0304-4165(93)90013-X. |
| [8] Hwang HJ,Kim SH. Inverse relationship between fasting direct bilirubin and metabolic syndrome in Korean adults[J]. Clin Chim Acta,2010,411(19/20):1496-1501. DOI:10.1016/j.cca.2010.06.003. |
| [9] Jo J,Yun JE,Lee H,et al. Total,direct,and indirect serum bilirubin concentrations and metabolic syndrome among the Korean population[J]. Endocrine,2011,39(2):182-189. DOI:10.1007/s12020-010-9417-2. |
| [10] Sitlani CM,Rice KM,Lumley T,et al. Generalized estimating equations for genome-wide association studies using longitudinal phenotype data[J]. Stat Med,2015,34(1):118-130. DOI:10.1002/sim.6323. |
| [11] WHO. Guidelines for controlling and monitoring the tobacco epidemic[M]. Geneva:World Health Organization,1998. |
| [12] 马冠生,朱丹红,胡小琪,等. 中国居民饮酒行为现况[J]. 营养学报,2005,27(5):362-365. DOI:10.13325/j.cnki.acta.nutr.sin.2005.05.003. Ma GS,Zhu DH,Hu XQ,et al. The drinking practice of people in China[J]. Acta Nutr Sin,2005,27(5):362-365. DOI:10.13325/j.cnki.acta.nutr.sin.2005.05.003. |
| [13] 中华医学会糖尿病学分会代谢综合征协作组. 中华医学会糖尿病学血分会关于代谢综合征的建议[J]. 中华糖尿病杂志,2004,12(3):156-161. Metabolic Syndrome Cooperative Group of Chinese Diabetes Society. Chinese diabetes society's suggestion on metabolic syndrome definition[J]. Chin J Diabet,2004,12(3):156-161. |
| [14] Abu-Farha M,Behbehani K,Elkum N. Comprehensive analysis of circulating adipokines and hsCRP association with cardiovascular disease risk factors and metabolic syndrome in Arabs[J]. Cardiovasc Diabetol,2014,13:76. DOI:10.1186/1475-2840-13-76. |
| [15] Yoshino S,Hamasaki S,Ishida S,et al. Characterization of the effect of serum bilirubin concentrations on coronary endothelial function via measurement of high-sensitivity C-reactive protein and high-density lipoprotein cholesterol[J]. Heart Vessels,2013,28(2):157-165. DOI:10.1007/s00380-011-0228-z. |
| [16] Choi SH,Yun KE,Choi HJ. Relationships between serum total bilirubin levels and metabolic syndrome in Korean adults[J]. Nutr Metab Cardiovasc Dis,2013,23(1):31-37. DOI:10.1016/j.numecd.2011.03.001. |
| [17] Jenko-Pražnikar Z,Petelin A,Jurdana M,et al. Serum bilirubin levels are lower in overweight asymptomatic middle-aged adults:an early indicator of metabolic syndrome[J]. Metabolism,2013,62(7):976-985. DOI:10.1016/j.metabol.2013.01.011. |
| [18] Wang LN,Bautista LE. Serum bilirubin and the risk of hypertension[J]. Int J Epidemiol,2015,44(1):142-152. DOI:10.1093/ije/dyu242. |
| [19] Lin LY,Kuo HK,Hwang JJ,et al. Serum bilirubin is inversely associated with insulin resistance and metabolic syndrome among children and adolescents[J]. Atherosclerosis,2009,203(2):563-568. DOI:10.1016/j.atherosclerosis.2008.07.021. |
| [20] Troughton JA,Woodside JV,Young IS,et al. Bilirubin and coronary heart disease risk in the Prospective Epidemiological Study of Myocardial Infarction(PRIME)[J]. Eur J Cardiovasc Prev Rehabil,2007,14(1):79-84. DOI:10.1097/01.hjr. 0000230097.81202.9f. |
| [21] Li L,Wu J,Pu DH,et al. Factors associated with the age of natural menopause and menopausal symptoms in Chinese women[J]. Maturitas,2012,73(4):354-360. DOI:10.1016/j.maturitas. 2012.09.008. |