 2016, Vol. 37
2016, Vol. 37文章信息
- 陆芹, 张建辉, 刘永跃, 陆红敏, 田芸凡, 布仁巴图, 周逸鹏, 张永红.
- Lu Qin, Zhang Jianhui, Liu Yongyue, Lu Hongmin, Tian Yunfan, Buren Batu, Zhou Yipeng, Zhang Yonghong.
- 心血管疾病家族史和吸烟对缺血性脑卒中发病的联合效应
- Combined effects of both cardiovascular disease family history and smoking on the incidence of is chemic stroke
- 中华流行病学杂志, 2016, 37(4): 475-479
- Chinese Journal of Epidemiology, 2016, 37(4): 475-479
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2016.04.007
-
文章历史
- 收稿日期: 2015-08-11




2. 028000 内蒙古自治区通辽市医院神经内科;
3. 028000 内蒙古自治区通辽市疾病预防控制中心疾病控制科
2. Department of Internal Medicine-Neurology, Tongliao Municipal Hospital, Tongliao, Inner Mongolia 028000, China;
3. Tongliao Center for Disease Control and Prevention, Tongliao, Inner Mongolia 028000, China
脑卒中在全球居第二位死因,是重要公共卫生问题[1, 2]。但在我国占总死亡的22.45%,已成为第一位死因[3]。缺血性脑卒中约占所有脑卒中的87%[4],是遗传因素[5]、环境因素[6]或两者共同作用[7, 8]的复杂疾病。有研究显示,家族史是缺血性脑卒中的危险因素[9, 10]。吸烟作为环境因素,是公认的缺血性脑卒中的独立危险因素[11, 12]。此外有研究发现,遗传因素与吸烟在缺血性脑卒中的发病过程中起协同作用[13, 14]。目前关于心血管疾病家族史与吸烟的联合作用对缺血性脑卒中事件危险性的前瞻性队列研究报道较少,且鲜有针对蒙古族人群的有关报道。为此本文探讨蒙古族人群心血管疾病家族史与吸烟的联合作用对缺血性脑卒中的影响。
对象与方法1. 调查对象:源自通辽市科左后旗朝鲁吐苏木(乡)和奈曼旗固日班花苏木所属32个村庄年龄≥20岁长期居住当地的蒙古族农牧民,并排除了恶性肿瘤、心肌梗死、脑卒中、慢性肾病、内分泌疾病者。2002-2003年进行基线资料收集、血标本和生化指标采集,2004-2012年8月对其中签署知情同意书并血标本和资料完整者2 589人进行连续随访调查。有6名调查对象因迁出而失访,随访应答率为99.8%。
2. 调查方法:
(1)基线调查:由专业培训人员采用统一编制的调查表收集调查对象的人口统计学资料、个人疾病史、心血管疾病家族史、吸烟和饮酒情况等。心血管疾病家族史定义为一级亲属中至少有1名或二级亲属中至少有2名曾经或现在患有心血管疾病者;吸烟定义为平均每天吸烟不少于1支,并持续1年以上;饮酒定义为平均每天饮白酒不少于50 ml(或相当于酒精含量的其他酒类),并持续1年以上。
采用标准方法测量身高、体重和腰围,并计算BMI(kg/m2)。使用台式汞柱血压计,按国际标准化方法对每名调查对象连续测量3次血压(SBP和DBP),取均值。清晨采血利用Roche 血糖仪测定FPG,全自动生化分析仪检测TC、TG和HDL-C,并依此计算LDL-C。
(2)随访调查:2004-2012 年8月进行连续随访。以缺血性脑卒中(包括脑血栓形成、脑栓塞和腔隙性脑栓塞)的发生作为结局事件。其他原因死亡、观察期内失访或最后一次随访时存活且无脑卒中发生的调查对象均视为截尾数据。缺血性脑卒中的诊断均经县级及其以上医院通过CT和MRI诊断证明。
3. 统计学分析:采用EpiData软件建立数据库,采用双盲法录入,并核查纠错,应用SAS 9.2软件和SPSS软件进行统计学分析。基线资料分析中的计量资料经正态性检验,均为非正态分布(P<0.01),以中位数(M)和四分位数间距(IQR)表示,其组间比较采用非参数秩和检验;计数资料以率表示,其组间比较采用 χ2检验。将调查对象按照心血管疾病家族史与吸烟情况分为无心血管疾病家族史/不吸烟、无心血管疾病家族史/吸烟、心血管疾病家族史/不吸烟与心血管疾病家族史/吸烟4组。以Kaplan-Meier(K-M)方法绘制并比较4组调查对象的缺血性脑卒中事件累积发病率。应用Cox比例回归模型分析心血管疾病家族史与吸烟的联合作用对缺血性脑卒中事件发生的风险比(HR值及其95%CI),采用双侧检验,α=0.05。
结 果1. 基线特征:在2 589名完成基线调查的对象中,有6人因迁出而失访,共2 583人完成随访调查,按有无心血管疾病家族史及是否吸烟情况,分为四组,分析其基线特征。结果显示(表 1),心血管疾病家族史/吸烟组的年龄[50(41~64)岁]、男性率(75.6%,136/180)、饮酒率(61.1%,110/180)以及SBP[140(130~160)mmHg](1 mmHg=0.133 kPa)、DBP[93(84~100)mmHg]、TC[3.77(3.03~4.65)mmol/L]、TG[1.06(0.74~1.79)mmol/L]水平均高于其他三组,差异有统计学意义(P<0.001);心血管疾病家族史/不吸烟与心血管疾病家族史/吸烟两组的男性率、SBP、DBP、TC以及LDL-C的情况明显高于其他两组,差异有统计学意义(P<0.05);无心血管疾病家族史/吸烟、心血管疾病家族史/吸烟两组的年龄、饮酒率明显高于其他两组,差异有统计学意义(P<0.001)。四组间在年龄、男性率、饮酒率以及心率、SBP、DBP、BMI、FPG、TC、TG和LDL-C水平的差异均有统计学意义(P<0.05)。
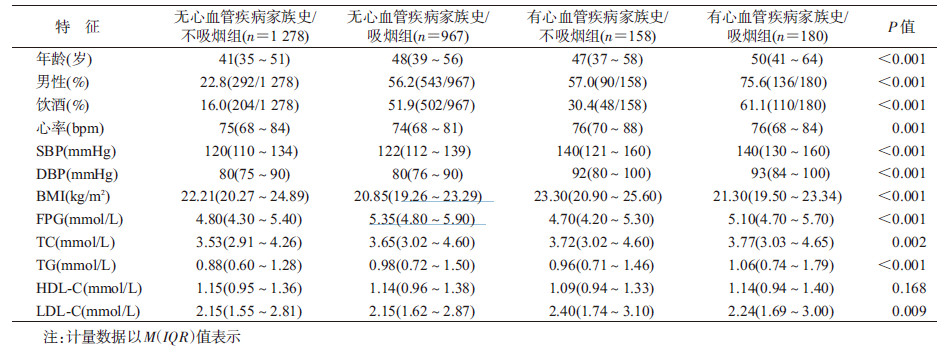
2. 心血管疾病家族史及吸烟联合作用与缺血性脑卒中发病的关系:以K-M方法绘制四组调查对象的缺血性脑卒中事件累积发病率曲线。结果显示(图 1),四组累积发病率均呈现逐渐增长的趋势,各组间累积发病率的差异有统计学意义(P<0.05)。心血管疾病家族史/吸烟组累积发病率(8.33%,15/180)最高,而无心血管疾病家族史/不吸烟组(1.17%,15/1 278)最低,心血管疾病家族史/不吸烟组和无心血管疾病家族史/吸烟组的累积发病率分别为5.70%(9/158)和3.83%(37/967)。在经年龄和性别调整的Cox比例回归模型分析中(表 2),与无心血管疾病家族史/不吸烟组相比,无心血管疾病家族史/吸烟组、有心血管疾病家族史/不吸烟组和有心血管疾病家族史/吸烟组发生缺血性脑卒中的风险性均显著升高,其HR值(95%CI)分别为1.93(1.05~3.55)、2.67(1.16~6.18)和3.32(1.59~6.93),差异有统计学意义(P<0.05)。在经多因素调整的Cox比例回归模型分析后,与无心血管疾病家族史/不吸烟组相比,无心血管疾病家族史/吸烟组和有心血管疾病家族史/吸烟组发生缺血性脑卒中的风险性均显著升高,其HR值(95%CI)分别为2.26(1.19~4.28)和2.45(1.13~5.33),差异有统计学意义(P<0.05),其中有心血管疾病家族史/吸烟组发生缺血性脑卒中的风险性最高。

|
| 图 1 四组调查对象缺血性脑卒中的累积发病率 |
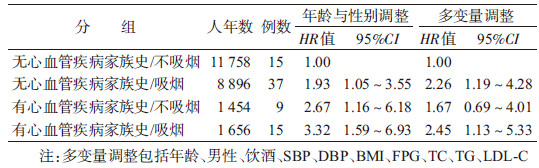
本研究以人口流动性小的内蒙古农牧区蒙古族人群为研究对象,在获得了基线心血管疾病家族史和吸烟状况以及缺血性脑卒中发病结局资料的基础上,将研究对象按照心血管疾病家族史与吸烟情况分为四组进行K-M方法分析,结果显示无心血管疾病家族史并不吸烟组、无心血管疾病家族史并吸烟组、有心血管疾病家族史并不吸烟组和有心血管疾病家族史并吸烟组的累积发病率分别为1.17%(15/1 278)、 3.83%(37/967)、5.70%(9/158)和8.33%(15/180),以有心血管疾病家族史并吸烟组的累积发病率最高。进一步的Cox比例回归分析显示,与无心血管疾病家族史且不吸烟组相比,无心血管疾病家族史并吸烟组和有心血管疾病家族史并吸烟组发生缺血性脑卒中事件的HR值分别为2.26和2.45,以有心血管疾病家族史并吸烟组的危险性最高。由此可见,与既无心血管疾病家族史也不吸烟的人群相比,有心血管疾病家族史人群和吸烟人群均具有较高的发生缺血性脑卒中事件的风险性,其中尤以有心血管疾病家族史并吸烟的人群具有更高的危险性。
已有研究报道,缺血性脑卒中是遗传因素[15]、环境因素[16]或遗传因素与环境因素共同作用[17]的复杂疾病。单独的心血管疾病家族史[18]或吸烟[19- 20]均可能是缺血性脑卒中的危险因素。国内的病例对照研究显示[21, 22],有心血管疾病家族史的人群更易患缺血性脑卒中,一级亲属缺血性脑卒中遗传度可高达47.8%~56.5%,二级亲属患缺血性脑卒中的遗传度可达13.2%~40.95%。研究发现[22, 23],有心血管疾病家族史的人群发生缺血性脑卒中概率显著高于无心血管疾病家族史人群。Silva等[24]研究发现,在中青年缺血性脑卒中患者中,有家族史者占18.4%,成为该人群患缺血性脑卒中第二大危险因素。吸烟是已知的缺血性脑卒中生活方式危险因素[14, 25]。Framingham研究显示,吸烟可显著增加脑卒中的发病危险,且吸烟量越大,危险性越大[26]。另有研究报告,吸烟会导致动脉粥样硬化[27],而动脉粥样硬化又是缺血性脑卒中的重要病理机制[28]。
本文旨在通过队列研究检验心血管疾病家族史和吸烟对缺血性脑卒中的发病危险是否具有联合作用。结果显示四组人群中,具有心血管疾病家族史并吸烟组不仅具有最高的缺血性脑卒中累积发病率,还具有最高的发病风险比,表明有心血管疾病家族史可放大吸烟对缺血性脑卒中发病的危险性效应。刘建平[29]在分析基因与环境的交互作用同缺血性脑卒中关系发现,高血压家族史、糖尿病家族史与吸烟存在正相加交互作用,支持本文的结果。
本文结果具有重要的公共卫生意义,尤其是对我国吸烟率高的农村人群。在缺血性脑卒中的预防控制工作中,除重视一般人群的控烟外,更应强调在有心血管疾病家族史人群中的控烟。
本文存在局限性。如分析时并未考虑年吸烟量和吸烟年限,因此无法探讨吸烟量与缺血性脑卒中结局的关系;调查中发现男女吸烟状况存在差异,由于样本量小,未进行性别分层分析,仅在Cox比例风险模型分析时调整了性别;另外,未系统收集研究对象随访期间吸烟状况的变化,可能对结果有一定影响,但该人群对缺血性脑卒中预防的知晓率低,随访期间整体人群戒烟概率可能也较低。
总之,本研究结果提示在具有心血管疾病家族史的人群中,吸烟可增加其发生缺血性脑卒中的危险性。
利益冲突 无| [1] Hachinski V,Donnan GA,Gorelick PB,et al. Stroke:working toward a prioritized world agenda[J]. Int J Stroke,2010,5(4):238-256. DOI:10.1111/j.1747-4949.2010.00442.x. |
| [2] World Health Organization. The global burden of disease:2004 update[M]. Geneva:World Health Organization,2008:1-146. |
| [3] 陈竺. 全国第三次死因回顾抽样调查报告[M]. 北京:中国协和医科大学出版社,2008. Chen Z. The third cause of death in the country to review the sample survey report[M]. Beijing:Peking Union Medical College Press,2008. |
| [4] Lloyd-Jones D,Adams RJ,Brown TM,et al. Executive summary:heart disease and stroke statistics-2010 update:a report from the American Heart Association[J]. Circulation,2010,121(7):948-954. DOI:10.1161/CIRCULATIONAHA.109. 192666. |
| [5] Jerrard-Dunne P,Cloud G,Hassan A,et al. Evaluating the genetic component of ischemic stroke subtypes:a family history study[J]. Stroke,2003,34(6):1364-1369. DOI:10.1161/01.STR.0000069723.17984.FD. |
| [6] Yao XY,Lin Y,Geng JL,et al. Age-and gender-specific prevalence of risk factors in patients with first-ever ischemic stroke in china[J]. Stroke Res Treat,2012,2012:136398. DOI:10.1155/2012/136398. |
| [7] Ross OA,Worrall BB,Meschia JF. Advancing stroke therapeutics through genetic understanding[J]. Curr Drug Targets,2007,8(7):850-859. DOI:10.2174/138945007781077355. |
| [8] Gao XG,Yang H,Teng ZP. Association studies of genetic polymorphism,environmental factors and their interaction in ischemic stroke[J]. Neurosci Lett,2006,398(3):172-177. DOI:10.1016/j.neulet.2005.12.078. |
| [9] Choi JC,Lee JS,Kang SY,et al. Family history and risk for ischemic stroke:sibling history is more strongly correlated with the disease than parental history[J]. J Neurol Sci,2009,284(1/2):29-32. DOI:10.1016/j.jns.2009.03.015. |
| [10] Yamada Y,Metoki N,Yoshida H,et al. Genetic risk for ischemic and hemorrhagic stroke[J]. Arterioscler Thromb Vasc Biol,2006,26(8):1920-1925. DOI:10.1161/01.ATV.0000229694.97827.38. |
| [11] 马晓萍,李婧,欧文静,等. 吸烟与缺血性脑卒中关系的病例-对照研究[J]. 卫生研究,2014,43(1):32-37. Ma XP,Li J,Ou WJ,et al. A case-control study on the association between cigarette smoking and ischemic stroke[J]. J Hyg Res,2014,43(1):32-37. |
| [12] Hawkins BT,Brown RC,Davis TP. Smoking and ischemic stroke:a role for nicotine?[J]. Trends Pharmacol Sci,2002,23(2):78-82. DOI:10.1016/S0165-6147(02)01893-X. |
| [13] Pezzini A,Grassi M,Zotto ED,et al. Synergistic effect of apolipoprotein E polymorphisms and cigarette smoking on risk of ischemic stroke in young adults[J]. Stroke,2004,35(2):438-442. DOI:10.1161/01.STR.0000112973.00867.98. |
| [14] Ovbiagele B,Weir CJ,Saver JL,et al. Effect of smoking status on outcome after acute ischemic stroke[J]. Cerebrovasc Dis,2006,21(4):260-265. DOI:10.1159/000091224. |
| [15] Della-Morte D,Guadagni F,Palmirotta R,et al. Genetics of ischemic stroke,stroke-related risk factors,stroke precursors and treatments[J]. Pharmacogenomics,2012,13(5):595-613. DOI:10.2217/pgs.12.14. |
| [16] Hankey GJ. Potential new risk factors for ischemic stroke:what is their potential?[J]. Stroke,2006,37(8):2181-2188. DOI:10.1161/01.STR.0000229883.72010.e4. |
| [17] Stankovi S,Majkić-Singh N. Advances in the genetic basis of ischemic stroke[J]. J Med Biochem,2008,27(2):123-134. DOI:10.2478/v10011-008-0004-5. |
| [18] Kastorini CM,Georgousopoulou E,Vemmos KN,et al. Comparative analysis of cardiovascular disease risk factors influencing nonfatal acute coronary syndrome and ischemic stroke[J]. Am J Cardiol,2013,112(3):349-354. DOI:10.1016/j.amjcard.2013.03.039. |
| [19] Xu T,Bu XQ,Li HM,et al. Smoking,heart rate,and ischemic stroke:a population-based prospective cohort study among Inner Mongolians in China[J]. Stroke,2013,44(9):2457-2461. DOI:10.1161/STROKEAHA.111.000648. |
| [20] Park SY,Lee SH,Lee YB,et al. The interaction between eNOS and MTHFR genetic polymorphism modify effect of cigarette smoking on the risk of ischemic stroke[J]. Epidemiology,2006,17(6):S346. |
| [21] 李晓泽,王迎. 脑梗死遗传及环境因素的病例对照研究[J]. 中国药物与临床,2009,9增刊:67-68. DOI:10.3969/j.issn.1671-2560.2009.z1.038. Li XZ,Wang Y. A case-control study on the risk factor and genetic epidemiology of ischemic cerebral stroke[J]. Chin Remedies Clin,2009,9 Suppl:67-68. DOI:10.3969/j.issn.1671-2560.2009.z1.038. |
| [22] 史宝林,张勇,武艳华,等. 脑梗死的遗传流行病学研究[J]. 中华流行病学杂志,2003,24(8):719-721. Shi BL,Zhang Y,Wu YH,et al. A study on genetic epidemiology of cerebral infarction[J]. Chin J Epidemiol,2003,24(8):719-721. |
| [23] Floßmann E,Schulz UGR,Rothwell PM. Systematic review of Methods and Results of studies of the genetic epidemiology of ischemic stroke[J]. Stroke,2004,35(1):212-227. DOI:10.1161/01.STR.0000107187.84390.AA. |
| [24] Silva RD,Gamage R,Wewelwala C,et al. Young strokes in Sri Lanka:an unsolved problem[J]. J Stroke Cerebrovasc Dis,2009,18(4):304-308. DOI:10.1016/j.jstrokecerebrovasdis.2008.11. 004. |
| [25] Du Plooy JN,Buys A,Duim W,et al. Comparison of platelet ultrastructure and elastic properties in thrombo-embolic ischemic stroke and smoking using atomic force and scanning electron microscopy[J]. PLoS One,2013,8(7):e69774. DOI:10.1371/journal.pone.0069774. |
| [26] Wolf PA,D'Agostino RB,Kannel WB,et al. Cigarette smoking as a risk factor for stroke:the framingham study[J]. JAMA,1988,259(7):1025-1029. DOI:10.1001/jama.1988.03720070025028. |
| [27] Howard G,Wagenknecht LE,Burke GL,et al. Cigarette smoking and progression of atherosclerosis:the Atherosclerosis Risk in Communities(ARIC) study[J]. JAMA,1998,279(2):119-124. DOI:10.1001/jama.279.2.119. |
| [28] Rubattu S,Giliberti R,Volpe M. Etiology and pathophysiology of stroke as a complex trait[J]. Am J Hypertens,2000,13(10):1139-1148. DOI:10.1016/S0895-7061(00)01249-8. |
| [29] 刘建平. 缺血性脑卒中易感基因与环境因素交互作用的分子流行病学研究[D]. 武汉:华中科技大学,2008. Liu JP. A molecular epidemiological study of gene polymorphisms and environmental factor associated with ischemic stroke[D]. Wuhan:Huazhong University of Science and Technology,2008. |