 2016, Vol. 37
2016, Vol. 37文章信息
- 崔朋伟, 刘娜, 李静欣, 黄涛, 葛海霞, 武庆斌, 段招军.
- Cui Pengwei, Liu Na, Li Jingxin, Huang Tao, Ge Haixia, Wu Qingbin, Duan Zhaojun.
- 苏州市2007-2013年2岁以下儿童住院肠套叠流行特征
- Epidemiology of intussusception related hospitalizations in children aged <2 years in Suzhou, 2007-2013
- 中华流行病学杂志, 2016, 37(3): 410-414
- Chinese Journal of Epidemiology, 2016, 37(3): 410-414
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2016.03.025
-
文章历史
- 收稿日期: 2015-07-30




2. 215000 苏州大学附属儿童医院消化内科
2. Department of Gastroenterology, Affiliated Children's Hospital of Soochow University, Suzhou 215000, China
Wu Qingbin, Email: qingbin6638@ aliyun.com
轮状病毒是导致全球儿童重症腹泻的主要病原[1]。水质和卫生条件的改善并不会明显降低其发病率,且治疗亦无特效药,而疫苗可能是唯一预防轮状病毒重症腹泻发生及死亡的途径[2, 3]。1998年全球首个轮状病毒疫苗RotaShield应用临床,后因与发生肠套叠相关而撤销[3, 4]。WHO建议将轮状病毒疫苗纳入国家免疫规划且推荐Rotarix和RotaTeq两种疫苗,但两种疫苗是否与肠套叠相关,不同地区研究结果有差异[3, 5, 6, 7, 8]。因此,在我国轮状病毒疫苗大规模使用之前需了解肠套叠发病基线资料,为疫苗的安全性评价提供数据支持。现将2007年1月1日至2013年8月31日苏州市<2岁儿童肠套叠住院病例发病状况及临床特征报道如下。
对象与方法1. 研究对象:回顾性调查苏州大学附属儿童医院2007年1月1日至2013年8月31日年龄<2岁肠套叠住院患儿。数据由病案室提供。
2. 研究内容:使用统一调查表收集数据,包括人口学信息、发病及就诊信息、临床表现、诊断和治疗方法等。
3. 肠套叠确诊标准:按ICD-10:K56.1标准。①手术时确认肠套叠;②空气/液体灌肠发现肠套叠;③腹部超声观察到特定形状(横向:靶征或甜面包圈征;纵向:肾形或三明治征),且在灌肠后减轻或消失;④尸检时发现肠套叠[9]。
4. 统计学分析:2007-2013年苏州市人口资料由苏州市统计局提供。利用EpiData 3.0软件建立数据库,数据分析采用Excel 2010和SPSS 13.0软件。非正态分布资料描述使用M和四分位间距(QR)表示;年龄比较采用Wilcoxon秩和检验;采用简单线性回归分析发病年龄M和发病率随年份变化的趋势;利用Origin 8.0软件对年龄和季节分布进行多项式拟合;Exact Clopper Pearson法估算95%CI。
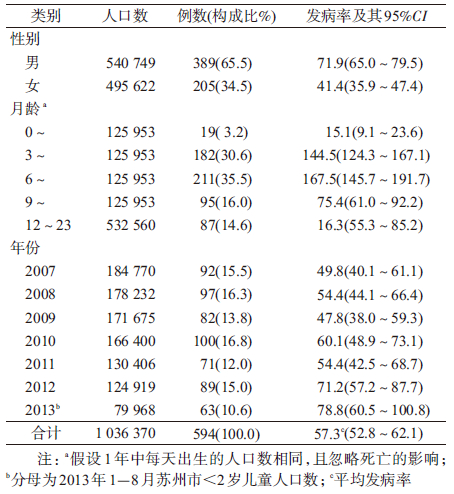
结 果1. 发病率:2007年1月1日至2013年8月31日该医院共收入594例<2岁肠套叠住院病例,无死亡病例。估计<2岁、<1岁和1~2岁儿童住院肠套叠发病率分别为57.3(95%CI:52.8~62.1)/10万、100.6(95%CI:92.1~109.8)/10万和16.3(95%CI:13.1~20.2)/10万。<2岁儿童发病率呈升高趋势,由2007年49.8(95%CI:40.1~61.1)/10万上升至2013年78.8(95%CI:60.5~100.8)/10万;<1岁儿童由91.3(95%CI:72.7~113.2)/10万升高至147.0(95%CI:110.4~191.7)/10万。两组儿童发病情况经简单线性回归拟合,差异有统计学意义(<2岁:F=13.445,P=0.014;<1岁:F=6.250,P=0.054)。见表 1和图 1。

|
| 图 1 2007-2013年苏州市<2岁儿童住院肠套叠 发病率变化趋势 |
以上发病率计算是基于假设苏州市儿童医院卫生服务覆盖了全部(100%)肠套叠病例。当假设覆盖范围为75%时,<2岁、<1岁和1~2岁儿童发病率分别为76.4(95%CI:71.2~81.9)/10万、134.2(95%CI:124.3~144.7)/10万和21.8(95%CI:18.0~22.0)/10万;当假设覆盖范围为50%时,3组儿童发病率分别为114.6(95%CI:108.2~121.3)/10万、201.3(95%CI:189.1~214.0)/10万和32.7(95%CI:28.0~37.9)/10万。
2. 人群分布:
(1)性别:594例中男性389例,女性205例,男女病例数之比为1.90 ∶ 1。估计<2岁和<1岁儿童住院肠套叠男性发病率分别为71.9(95%CI:65.0~79.5)/10万和126.2(95%CI:112.9~140.5)/10万,女性分别为41.4(95%CI:35.9~47.4)/10万和73.1(95%CI:62.7~84.7)/10万。
(2)年龄:<1岁儿童为主要发病人群(85.4%,507/594),其中又以3~8月龄儿童居多(66.2%,393/594),0~2月龄仅占3.2%(19/594),5~8月龄为发病高峰(图 2)。<2岁住院病例的发病年龄为6.8(QR=4.4)月龄,且呈逐年增高趋势,由2007年的6.3(QR=4.2)月龄增至2013年的7.3(QR=4.0)月龄,经简单线性回归拟合,差异有统计学意义(F=10.000,P=0.025)。男童发病年龄为6.9(QR=4.6)月龄,女童为6.6(QR=4.1)月龄,经Wilcoxon秩和检验,差异无统计学意义(Z=-0.829,P=0.407)。

|
| 图 2 2007-2013年苏州市<2岁儿童住院肠套叠病例年龄分布 |
3. 季节:住院病例全年皆有分布,虽然住院例数从3月开始缓慢上升,8月后缓慢下降,但无明显的季节性分布趋势(图 3)。

|
| 图 3 2007-2012年苏州市<2岁儿童住院肠套叠病例发病季节分布 |
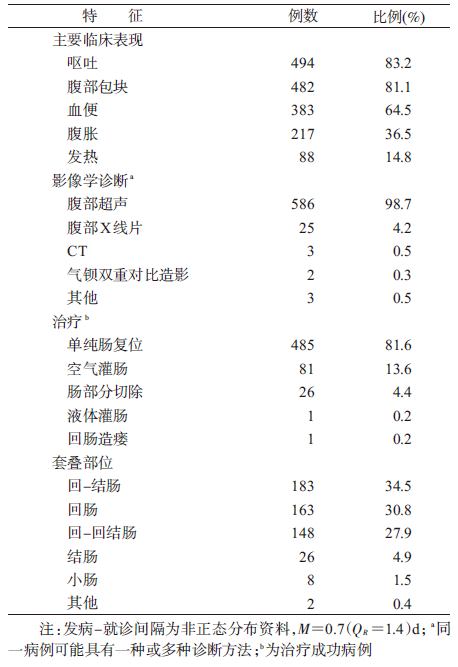
4. 临床特征:主要为肠套叠一般特征,如呕吐、腹部包块、血便(表 2)。发生部位一般以回-结肠型、回肠型、回-回-结肠型常见。影像学诊断方法主要为腹部超声。住院病例以手术治疗为主(86.2%,512/594),其中26例行肠切除术,1例行回肠造瘘术。非手术治疗包括空气灌肠和液体灌肠,分别占13.6%(81/594)和0.2%(1/594)。
本研究显示2007-2013年苏州市<2岁儿童住院肠套叠发病率为57.3/10万,其中<1岁儿童为100.6/10万,高于该地区1999-2003年的结果(<2岁为27.9/10万;<1岁为56.0/10万)。Jiang等[10]报道全球<1岁儿童肠套叠平均发病率为74/10万,本文该年龄组发病率高于全球平均水平,与我国香港地区(108/10万)相当[11],但高于我国台湾地区(70/10万~90/10万)[12]和低于山东省临沂地区(188.28/10万)[13]。
6年间<2岁和<1岁儿童住院肠套叠发病率总体呈升高趋势。其中<2岁儿童由2007年的49.8/10万升高至2013年的78.8/10万,<1岁儿童由91.3/10万升至147.0/10万,增加近1.6倍。而美国、韩国、新加坡等国研究报道多呈下降趋势[14, 15, 16]。一般肠套叠发病除与肠道、淋巴组织等解剖学结构有关外,还可能与感染腺病毒、轮状病毒等以及饮食等因素有关[17]。本研究苏州市儿童住院肠套叠发病率呈升高趋势,推测可能的原因:一是环境或其他因素的改变或相互作用使儿童更加易感[18];二是肠套叠诊断技术提高,如超声等诊断设备普及应用等;三是当地轮状病毒疫苗使用量逐年增加,但与肠套叠发病是否相关仍需进一步观察。
本文大部分病例为<1岁儿童,发病高峰为5~8月龄,0~2月龄较少,与其他报道基本一致[2, 10, 19]。6年间发病年龄M呈增高趋势,由2007年的6.3月龄增至2013年的7.3月龄,美国、新加坡的研究也观察到此种趋势,可能与环境卫生改善导致儿童感染风险降低有关[15, 16]。另外,一般建议在肠套叠发病快速上升前尽早完成轮状病毒疫苗接种 [20]。本文结果可为我国制定儿童轮状病毒疫苗免疫程序提供参考。
关于肠套叠是否存在季节性发病,各国研究存在差异,至今仍无定论[2, 10, 19]。本研究在住院病例中未观察到发病有明显的季节性。
本文肠套叠病例临床表现主要为呕吐、腹部包块和血便,但不同国家或地区的病例主要临床表现不尽相同[14, 21]。腹部超声为主要影像学诊断方法[10]。临床治疗以灌肠为主[2, 10, 13, 22, 23],与本文手术治疗为主不符。究其原因,本文住院病例为门诊灌肠治疗失败或重症病例,故手术治疗为主要方法。本文无死亡病例,而非洲等发展中国家肠套叠平均死亡率高达9.4%(2%~25%)[10],与发病后及时就诊有关(本文发病-就诊间隔0.7 d)[24, 25]。因此,肠套叠发生后应及早就医以减少并发症。
本研究由于缺乏苏州市儿童医院卫生服务覆盖范围相关数据,发病率的计算是基于假设其覆盖了苏州地区全部儿童住院肠套叠病例,以达到与该地区较早研究同质可比[22, 23],且计算了假设覆盖范围为50%和75%时该地区的发病率,以防止发病率被低估。
本文为回顾性调查。初步表明儿童住院肠套叠发病率存在地区、时间差异,而研究方法、病例纳入标准以及年龄构成等因素均影响其结果,故建议建立哨点医院肠套叠主动监测,使结果更可信且可比,尤其在轮状病毒疫苗将纳入国家免疫规划前后。总之,本文为估计肠套叠发病率提供基线数据,也为将来我国新型轮状病毒疫苗上市后安全监测提供数据支持。
利益冲突 无| [1] Parashar UD,Gibson CJ,Bresee JS,et al. Rotavirus and severe childhood diarrhea[J]. Emerg Infect Dis,2006,12(2):304-306. DOI:10.3201/eid1202.050006. |
| [2] World Health Organization. Acute intussusception in infants and children. Incidence,clinical presentation and management:a global perspective[R]. Geneva:World Health Organization,2002. |
| [3] Vesikari T. Rotavirus vaccination:a concise review[J]. Clin Microbiol Infect,2012,18 Suppl 5:57-63. DOI:10.1111/j.1469-0691.2012.03981.x. |
| [4] Zhou WG,Pool V,Iskander JK,et al. Surveillance for safety after immunization:Vaccine Adverse Event Reporting System (VAERS)—United States,1991-2001[J]. MMWR Surveill Summ,2003,52(1):1-24. |
| [5] Patel MM,López-Collada VR,Bulhões MM,et al. Intussusception risk and health benefits of rotavirus vaccination in Mexico and Brazil[J]. N Engl J Med,2011,364(24):2283-2292. DOI:10.1056/NEJMoa1012952. |
| [6] Buttery JP,Danchin MH,Lee KJ,et al. Intussusception following rotavirus vaccine administration:post-marketing surveillance in the National Immunization Program in Australia[J]. Vaccine,2011,29(16):3061-3066. DOI:10.1016/j.vaccine. 2011.01.088. |
| [7] Shui IM,Baggs J,Patel M,et al. Risk of intussusception following administration of a pentavalent rotavirus vaccine in US infants[J]. JAMA,2012,307(6):598-604. DOI:10.1001/jama. 2012.97. |
| [8] Haber P,Patel M,Pan Y,et al. Intussusception after rotavirus vaccines reported to US VAERS,2006-2012[J]. Pediatrics,2013,131(6):1042-1049. DOI:10.1542/peds.2012-2554. |
| [9] Bines JE,Kohl KS,Forster J,et al. Acute intussusception in infants and children as an adverse event following immunization:case definition and guidelines of data collection,analysis,and presentation[J]. Vaccine,2004,22(5/6):569-574. DOI:10.1016/j.vaccine.2003.09.016. |
| [10] Jiang J,Jiang BM,Parashar U,et al. Childhood intussusception:a literature review[J]. PLoS One,2013,8(7):e68482. DOI:10.1371/journal.pone.0068482. |
| [11] Hong Kong Intussusception Study Group. Intussusception trends in Hong Kong children[J]. Hong Kong Med J,2007,13(4):279-283. |
| [12] Hsiao CC,Tsao LY,Lai CH. Nationwide population-based epidemiologic study of childhood and adulthood intussusception in Taiwan[J]. Pediatr Neonatol,2013,54(3):188-193. DOI:10.1016/j.pedneo.2013.01.004. |
| [13] 张荣鹏,张志亮,赵涛. 儿童肠套叠住院趋势分析[J]. 中华小儿外科杂志,2013,34(5):339-341. DOI:10.3760/cma.j.issn.0253-3006.2013.05.005. Zhang RP,Zhang ZL,Zhao T. Epidemiological analysis of childhood intussusception[J]. Chin J Pediatr Surg,2013,34(5):339-341. DOI:10.3760/cma.j.issn.0253-3006.2013.05.005. |
| [14] Jo DS,Nyambat B,Kim JS,et al. Population-based incidence and burden of childhood intussusception in Jeonbuk Province,South Korea[J]. Int J Infect Dis,2009,13(6):e383-388. DOI:10.1016/j.ijid.2009.01.011. |
| [15] Boudville IC,Phua KB,Quak SH,et al. The epidemiology of paediatric intussusception in Singapore:1997 to 2004[J]. Ann Acad Med Singapore,2006,35(10):674-679. |
| [16] Parashar UD,Holman RC,Cummings KC,et al. Trends in intussusception-associated hospitalizations and deaths among US infants[J]. Pediatrics,2000,106(6):1413-1421. DOI:10.1542/peds.106.6.1413. |
| [17] 李仕涛. 儿童肠套叠病因分析[J]. 现代医药卫生,2013,29(9):1344-1345. DOI:10.3969/j.issn.1009-5519.2013.09.033. Li ST. Etiology of intussusception for children[J]. J Mod Med Health,2013,29(9):1344-1345. DOI:10.3969/j.issn.1009-5519. 2013.09.033. |
| [18] van Trang N,Le Nguyen NT,Dao HT,et al. Incidence and epidemiology of intussusception among infants in Ho Chi Minh City,Vietnam[J]. J Pediatr,2014,164(2):366-371. DOI:10.1016/j.jpeds.2013.10.006. |
| [19] Huppertz HI,Soriano-Gabarró M,Grimprel E,et al. Intussusception among young children in Europe[J]. Pediatr Infect Dis J,2006,25(1 Suppl):S22-29. DOI:10.1097/01.inf.0000197713.32880.46. |
| [20] Centers for Disease Control and Prevention (CDC). Rotavirus vaccination coverage among infants aged 5 months-immunization information system sentinel sites,United States,June 2006-June 2009[J]. MMWR Morb Mortal Wkly Rep,2010,59(17):521-524. |
| [21] Khumjui C,Doung-ngern P,Sermgew T,et al. Incidence of intussusception among children 0-5 years of age in Thailand,2001-2006[J]. Vaccine,2009,27 Suppl 5:F116-119. DOI:10.1016/j.vaccine.2009.09.003. |
| [22] 武庆斌,顾红英,唐伟国,等. 婴幼儿肠套叠与轮状病毒性腹泻分布特征分析[J]. 中华实验和临床病毒学杂志,2008,22(3):216-218. DOI:10.3760/cma.j.issn.1003-9279.2008.03.020. Wu QB,Gu HY,Tang WG,et al. Distribution signature analysis between Intussusception and rotavirus diarrhea in young children[J]. Chin J Exp Clin Virol,2008,22(3):216-218. DOI:10.3760/cma.j.issn.1003-9279.2008.03.020. |
| [23] Guo WL,Zhang SF,Li JE,et al. Association of meteorological factors with pediatric intussusception in subtropical China:a 5-year analysis[J]. PLoS One,2014,9(2):e90521. DOI:10.1371/journal.pone.0090521. |
| [24] Mpabalwani EM,Chitambala P,Chibumbya JN,et al. Intussusception incidence rates in 9 Zambian hospitals,2007-2011:prerotavirus vaccine introduction[J]. Pediatr Infect Dis J,2014,33 Suppl 1:S94-98. DOI:10.1097/INF.0000000000000055. |
| [25] Tagbo BN,Mwenda J,Eke C,et al. Retrospective evaluation of intussusception in under-five children in Nigeria[J]. World J Vacc,2014,4(3):123-132. DOI:10.4236/wjv.2014.43015. |