 2016, Vol. 37
2016, Vol. 37文章信息
- 成姝雯, 肖川, 王旻, 王岚, 王娟, 任涛, 王丽萍, 文小华, 张文豪, 袁萍.
- Cheng Shuwen, Xiao Chuan, Wang Min, Wang Lan, Wang Juan, Ren Tao, Wang Liping, Wen Xiaohua, Zhang Wenhao, Yuan Ping.
- 四川省绵阳市成年人HBsAg与HBsAb双阴分布现况
- Distribution of both HBsAg and HBsAb negative adults in Mianyang, Sichuan province
- 中华流行病学杂志, 2016, 37(1): 60-63
- Chinese Journal of Epidemiology, 2016, 37(1): 60-63
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2016.01.012
-
文章历史
- 投稿日期: 2015-06-26




2. 610041 成都, 华西医院呼吸与危重症医学科;
3. 610041 成都, 感染性疾病中心;
4. 621051 四川省绵阳市涪城区疾病预防控制中心;
5. 621700 四川省江油市疾病预防控制中心
2. Respiratory and Critical Care Department, Sichuan University, Chengdu 610041, China;
3. Infectious Disease Center, Sichuan University, Chengdu 610041, China;
4. West China Hospital, Sichuan University, Chengdu 610041, China; Fucheng District Center for Disease Control and Prevention, Mianyang City, Sichuan Province, Mianyang 621051, China;
5. Jiangyou County Center for Disease Control and Prevention, Sichuan Province, Jiangyou 621700, China
我国2012年卫生统计年鉴显示,乙型肝炎(乙肝)发病率为81.54/10万,每年新发乙肝病例105万,乙肝流行形势在我国依然严峻。乙肝疫苗接种是预防HBV感染最经济有效的措施。1992年卫生部将乙肝疫苗(HepB)纳入儿童计划免疫管理,2002年纳入儿童免疫规划,提高了儿童HBsAb水平,使儿童HBV易感性降低[1]。成年人接种HepB则实行自愿、自费原则,成年人基本没有集体接种的机会,因此除特殊人群外,成年人HepB接种率只有25.37%[2]。2006年我国乙肝血清流行病学调查数据表明,我国15~59 岁人群的HBsAg 阳性率高达8.57%,成年人HBsAg与HBsAb双阴率高达37.97%[3]。双阴人群如不采取有效接种措施,可能会成为新的HBV感染者,甚至是HBV慢性携带者[4]。成年人中存在大量的双阴人群是我国总人群乙肝患病率居高不下的重要原因之一。目前我国关于HBsAg与HBsAb双阴者分布的大样本研究较少。本研究对四川省绵阳市≥15岁人群HBsAg与HBsAb双阴分布现况进行描述性分析,旨在为制定和实施成年人接种HepB的免疫策略提供依据。
对象与方法1. 调查对象:“十二五”国家科技重大专项“四川绵阳重大传染病综合防治示范研究信息平台”中,年龄≥15岁的常住居民(在该地居住达≥6个月的居民)。
2. 调查内容:
(1)问卷调查:由经过统一培训合格的调查员负责完成。问卷内容:一般人口学特征(性别、年龄、职业、婚姻状况等)、乙肝家族史等。
(2)乙肝表面标志物检测:按照严格的卫生和安全指南,采集调查对象空腹静脉血5 ml,立即离心血标本进行检测或将其保存于4~8 ℃冰箱内并在24 h内进行检测。采用ELISA检测血清HBsAg、HBsAb。乙肝表面标志物检测值<1者为阴性,HBsAg、HBsAb检测结果均为阴性称为双阴。
3. 统计学分析:应用SPSS 19.0软件进行分析,采用描述性统计学方法对人群基本情况的分布进行描述性分析,采用 χ2检验比较不同特征人群的双阴率,采用 χ2趋势检验分析年龄变化趋势,检验水准为P<0.01。
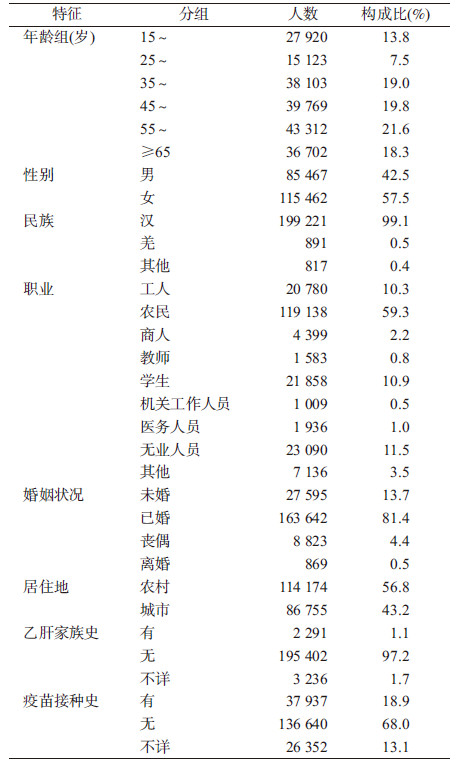
结 果1. 基本情况:共检测200 929名≥15岁人群,HBsAg阳性13 903名(7.0%),HBsAb阳性93 763名(46.6%),HBsAg与HBsAb均阳性141名(0.1%),HBsAg与HBsAb双阴93 122名(46.3%),见表1。
2. 不同年龄人群HBsAg与HBsAb双阴分布:以10岁为间隔,将年龄分为6组,15~24岁人群双阴率最低,为42.9%,≥65岁人群双阴率最高,为50.3%,随年龄增大双阴率有增加的趋势(趋势 χ2=697.336,P<0.01),见表2。
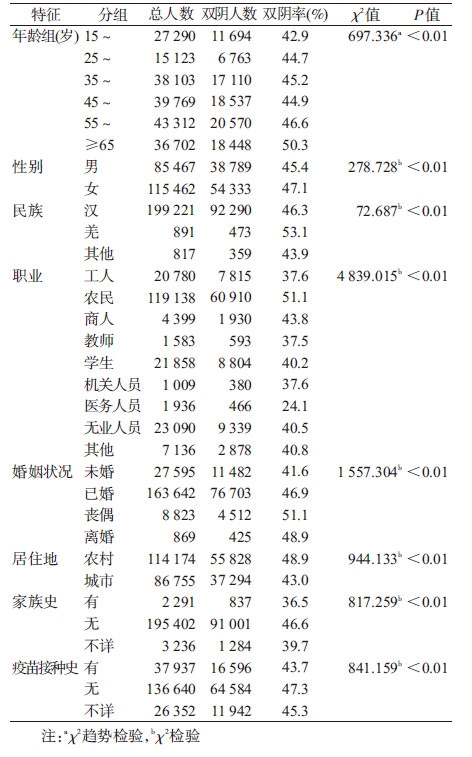
3. 不同性别、民族人群HBsAg与HBsAb双阴分布:女性双阴率(47.1%)高于男性(45.4%),差异有统计学意义(P<0.01),见表2。汉族人群双阴率为46.3%,低于羌族人群(53.1%),高于其他少数民族(43.9%),将羌族与其他少数民族合并后,少数民族双阴率为48.7%,与汉族的双阴率差异有统计学意义(P<0.01),见表2。
4. 不同职业、婚姻状况人群HBsAg与HBsAb双阴分布:农民双阴率最高,为51.1%,其次为商人(43.8%),医务人员双阴率最低,为24.1%,不同职业人群双阴率差异有统计学意义(P<0.01),见表2。丧偶人群双阴率最高,为51.1%,未婚人群双阴率最低,为41.6%,不同婚姻状况人群双阴率差异有统计学意义(P<0.01),见表2。
5. 农村与城市人群HBsAg与HBsAb双阴分布:农村人群双阴率为48.9%,高于城市人群(43.0%),差异有统计学意义(P<0.01),见表2。
6. 不同乙肝家族史、乙肝疫苗接种史人群HBsAg与HBsAb双阴分布:无乙肝家族史人群的双阴率(46.6%)高于有乙肝家族史人群(36.5%),差异有统计学意义(P<0.01),见表2。未接种过乙肝疫苗人群的双阴率(47.3%)高于接种人群(43.7%),差异有统计学意义(P<0.01),见表2。
讨 论HBsAg与HBsAb均为阴性,意味着其未感染过HBV且未受到HepB保护,存在感染HBV的风险[3]。因此,了解人群中HBsAg与HBsAb双阴的分布情况,对分析乙肝易感性现状和防治乙肝感染均具有重要意义。
本研究显示,绵阳市成年人群中HBsAg与HBsAb双阴率为46.3%,低于“四川省绵阳市乙肝与结核、艾滋病规模化现场流调及分级协同综合防治一体化示范研究”获得的结果(55.3%),但仍高于崔富强等[3]2006年对中国15~59岁8.2万人乙肝易感性的调查结果(37.97%)以及土耳其关于人群双阴率(38.4%)的研究[5]。
本研究显示,绵阳市≥15岁人群各年龄组的双阴率均>40%,提示≥15岁人群各年龄段普遍易感,尤其是15~34岁年龄段人群,该年龄段人群社会活动频繁、各种暴露因素较多[3],同时该人群接种HepB后免疫应答水平最高[6],提示应加强对≥15岁人群关于乙肝及乙肝疫苗相关知识的健康教育工作,提高成年人特别是15~34岁年龄段人群HepB接种率。
本研究显示,女性双阴率略高于男性,母婴传播是乙肝的主要传播方式[7],母亲为HBsAg阳性者,其子女感染乙肝的可能性更大[5],提示要提高女性尤其是育龄期女性HepB接种率。此外,有研究发现接种HepB后,男性的HBsAb阳转率和滴度均低于女性[6]。提示成年男性需接种HBsAg诱导量更高的疫苗才能诱导出抗体[8]。
绵阳市是多民族城市,其中主要的少数民族为羌族,研究显示,汉族人群的HBsAg与HBsAb双阴率低于羌族人群,高于其他少数民族人群,可能其与各民族的文化背景、风俗习惯、健康意识有关[9]。提示应针对不同民族文化习俗,开展健康教育,提高各民族的HepB接种率。本研究显示,农民HBsAg与HBsAb双阴率最高,由于农民的文化程度相对较低,健康意识薄弱[10],农村地区卫生条件落后,乙肝疫苗接种质量相对较差[11],所以接种HepB的相对较少。研究显示,有乙肝家族史人群的HBsAg与HBsAb双阴率低于无乙肝家族史人群,由于有乙肝家族史人群与乙肝患者密切接触,其感染HBV的风险更大[4]。提示有乙肝家族史人群更需要接种HepB,使其能有效实现自我保护,此外,还应该定期进行健康体检。
研究结果发现,接种过乙肝疫苗人群HBsAg阳性率为4.3%,明显低于未接种疫苗人群(7.6%),且其HBsAb阳性率(51.4%)高于未接种人群(44.7%)。接种过乙肝疫苗的人群双阴率(43.7%)低于无乙肝疫苗接种史的人群(47.3%),且已有研究表明接种HepB,所获得的成本效益较高,对乙肝防治工作意义重大[12]。提示在认真落实儿童乙肝免疫规划的同时,应提高成年人健康意识,提高HepB接种率,从而推进我国乙肝防控工作的进程。
本研究以HBsAg、HBsAb双阴作为乙肝易感性标志,一般认为HBsAg、HBsAb和HBcAb三阴为乙肝易感[3],但国内外均有研究将HBsAg、HBsAb双阴作为乙肝易感性指标[7, 9],原因在于HBsAg与HBsAb均阴性时,HBcAb阳性率仅占1.46%[13],所占比例很小。且有研究指出,单项HBcAb阳性者接种HepB仍具有免疫保护效果,接种者可具有与HBsAg、HBsAb和HBcAb三阴者相似的免疫特点和保护性抗体[6]。因此,本研究采用HBsAg与HBsAb双阴作为易感指标亦有其科学依据,其与三阴作为易感性标志的意义是否不同,有待进一步研究证实。
利益冲突 无| [1] Liang XF,Bi SL,Yang WZ,et al. Evaluation of the impact of hepatitis B vaccination among children born during 1992-2005 in China[J]. J Infect Dis,2009,200(1) :39-47. DOI:10.1086/599332. |
| [2] 谈逸云,申惠国,赵黎芳,等. 成人乙肝疫苗主动接种影响因素分析[J]. 中国公共卫生,2010,26(2):218-220. Tan YY,Shen HG,Zhao LF,et al. Influencing factors of active vaccination of hepatitis B vaccine in adults[J]. Chin J Public Health,2010,26(2):218-220. |
| [3] 崔富强,张国民,孙校金. 中国15~59岁人群乙型肝炎病毒感染易感性分析[J]. 江苏预防医学,2013,24(4):1-3. DOI:10.3969/j.issn.1006-9070.2013.04.001. Cui FQ,Zhang GM,Sun XJ. Analysis on susceptibility of hepatitis B virus infection among population aged between 15 and 59 in China[J]. Jiangsu J Prev Med,2013,24(4):1-3. DOI: 10.3969/j.issn.1006-9070.2013.04.001. |
| [4] Croagh CM,Lubel JS. Natural history of chronic hepatitis B:Phases in a complex relationship[J]. World J Gastroenterol,2014,20(30):10395-10404. DOI: 10.3748/wjg.v20.i30.10395. |
| [5] Barut HS,Günal Ö,Göral A,et al. Prevalence of hepatitis B virus infection in children of HBsAg positive parents[J]. Mikrobiyol Bul,2011,45(2):359-365. |
| [6] 王吉玲. 成人乙型病毒性肝炎疫苗免疫策略研究[D]. 杭州:浙江大学,2007. Wang JL. Study on immunization strategy for Hepatitis B vaccination in adults[D]. Hangzhou: Zhejiang University,2007. |
| [7] Li ZX,Hou XM,Cao GW. Is mother-to-infant transmission the most important factor for persistent HBV infection?[J]. Emerg Microbes Infect,2015,4(5):e30. DOI: 10.1038/emi.2015.30. |
| [8] 王璐,李辉,王树声,等. 中国乙型肝炎不同流行区最佳免疫策略研究[J]. 中华预防医学杂志,1999,33(2):104-106. DOI:10.3760/j.issn.0253-9624.1999.02.013. Wang L,Li H,Wang SS,et al. Studies on immunization strategies for Hepatitis B in different endemic areas of China[J]. Chin J Prev Med,1999,33(2):104-106. DOI:10.3760/j.issn. 0253-9624.1999.02.013. |
| [9] 王婵娟,单可人,何燕,等. 贵州彝、瑶族及汉族HBV感染与IL-10-819相关性[J]. 中国公共卫生,2011,27(1):54-56. Wang CJ,Shan KR,He Y,et al. Association between IL- 10-819 polymorphism and susceptibility to hepatitis B virus infection in Han,Yi and Yao minority of Guizhou[J]. Chin J Public Health,2011,27(1):54-56. |
| [10] 顾院明. 农村人群乙型肝炎感染现况及生活质量研究[J]. 中国地方病防治杂志,2014,29增刊1:83. Gu YM. Study on the status and quality of life in the rural population[J ]. Chin J Contr Endem Dis,2014,29 Suppl 1:83. |
| [11] 汪娟. 安徽省部分地区乙型肝炎分子流行病学初步研究[D]. 合肥:安徽医科大学,2011. Wang J. Preliminary study of molecular epidemiology on Hepatitis B among certain regions in Anhui Province[D]. Hefei:Anhui Medical University,2011. |
| [12] 中华预防医学会,中国疾病预防控制中心免疫规划中心. 中国成人乙型肝炎免疫预防技术指南[J]. 中国病毒病杂志,2012,2(1):11-16. China Prevention Medicine Association, National Immunization Program,Chinese Center for Disease Control and Prevention. Technical guide for adult immunization hepatitis B immunization in China[J]. Chin J Viral Dis,2012,2(1):11-16. |
| [13] 武新梅,陈华. 健康体检人员13 241例乙型肝炎病毒五项标志物检测及感染模式分析[J]. 中国临床保健杂志,2011,14(5):493-495. DOI:10.3969/J.issn.1672-6790.2011.05.017. Wu XM,Chen H. Hepatitis B virus detection and infection pattern analysis of 13 241 health examination population[J]. Chin J Clin Health,2011,14(5):493-495. DOI: 10.3969/J.issn. 1672-6790.2011.05.017. |