 2015, Vol. 36
2015, Vol. 36文章信息
- 罗瑞丽, 霍丽娟, 张婕, 张倩楠. 2015.
- Luo Ruili, Huo Lijuan, Zhang Jie, Zhang Qiannan. 2015.
- 溃疡性结肠炎病因的Meta分析
- Meta-analysis on causes of ulcerative colitis
- 中华流行病学杂志, 2015, 36(12): 1419-1423
- Chinese Journal of Epidemiology, 2015, 36(12): 1419-1423
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2015.12.023
-
文章历史
- 收稿日期: 2015-03-17




溃疡性结肠炎(UC)是一种发生在直肠和结肠的慢性非特异性炎症性疾病,与克罗恩病(CD)同属于炎症性肠病(IBD)。国内外流行病学统计数据显示,近年来UC发病率和患病率呈明显增高趋势[1, 2, 3, 4, 5],欧洲地区为UC发病率(24.3/10万)及患病率最高的地区(505/10万),其次为北美洲地区[1]。中国、韩国、印度、伊朗等国也呈逐年上升趋势[2],中国UC患病率目前已超过11.6/10万[6]。UC已经成为肠道主要疾病之一,其病因尚不明确,近年来UC相关病因研究取得很大进展,但由于单个研究的样本量限制,说服力较差,且对某些因素的认识仍存在争议。本研究检索近15年国内外公开发表的关于UC病因相关因素的文献,进行统计学分析,阐述UC发病的主要相关因素及关联强度,为UC的发病机制研究以及预防UC提供理论依据。
资料与方法1. 资料来源和检索方法:计算机检索英文数据库PubMed、Cochrane、Embase及中文数据库中国知网(CNKI)、万方数据知识服务平台(Wanfang)、中国生物医学文献服务系统(SinoMed)与维普期刊资源整合服务平台(VIP),并辅以文献追溯、手工检索等方法,收集 2000年1月至2014年10月国内外公开发表的关于UC病因相关因素的研究文献。检索语种包括中文和英文。中文检索词:“溃疡性结肠炎”、“炎症性肠病”、“危险因素”、“相关因素”、“环境因素”,英文检索词:“Ulcerative colitis”、“Inflammatory bowel disease”、“Risk factors”、“Related factors”、“Environmental factors”。
2. 纳入标准:①2000年1月至2014年10月国内外发表的关于UC病因相关因素的病例对照研究、队列研究的原始文献;②UC病例诊断明确(经2名临床医师诊断或住院确诊病例);③样本量≥20; ④文献的研究假设和研究方法相似,暴露的定义基本相似;⑤提供OR值及其95%CI,或无OR值及95%CI但可以通过计算补全。
3. 排除标准:①同一样本的重复研究;②无对照组;③研究方法不准确、数据不完整;④只有单因素分析结果;⑤参照Wells等[7]制定的文献质量评价量表(NOS)标准,<5颗星的低质量文献;⑥病例组为IBD患者,未区分UC与CD患者。
4. 统计学分析:采用Stata 12.0软件完成。①异质性检验:采用Q检验与I2检验,当P<0.05、I2≥50.0%时,认为各研究间存在异质性,采用随机效应模型进行Meta分析,反之则采用固定效应模型分析。②敏感性分析:若各研究间无明显异质性,比较随机效应模型与固定效应模型结果;若各研究间存在异质性,剔除低质量研究后观察合并效应量的变化,未发生大的改变说明结果较为可信。③发表偏倚:采用Egger’s回归法进行评价,以P<0.05为存在发表偏倚。
结 果1. 文献筛选:共纳入病例对照研究24篇(其中巢式病例对照研究2篇),未找到合适的队列研究文献。见图1。

|
| 图 1 文献检索筛选流程 |
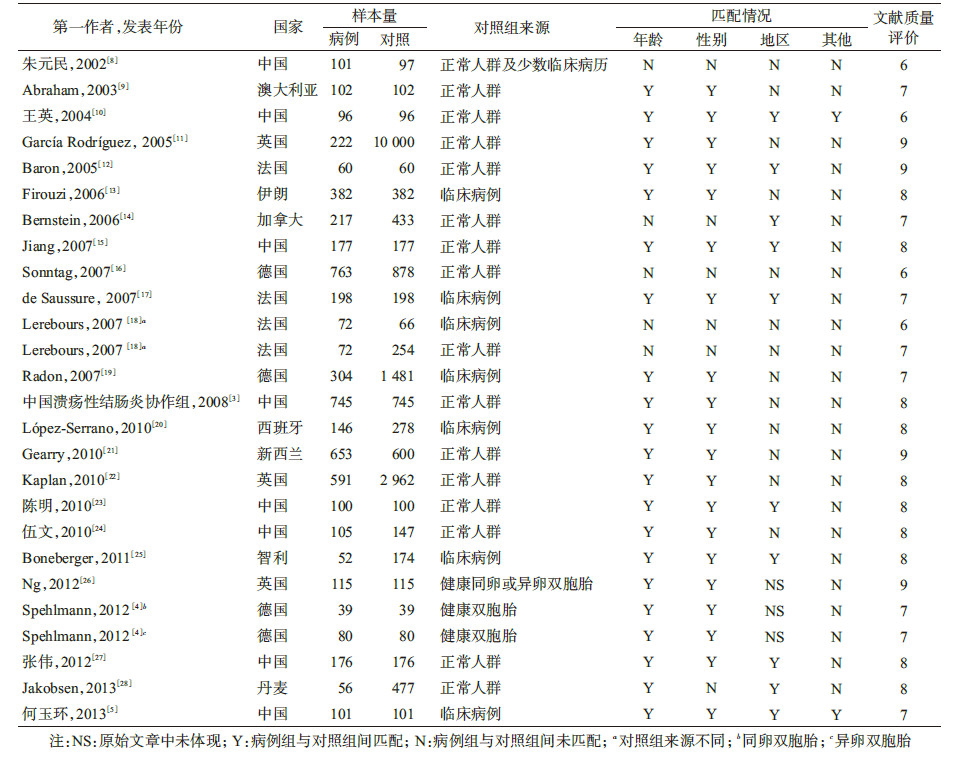
2. 纳入研究特征:共检索到1 580篇文献,按照纳入和排除标准筛选出24篇文献,全部为病例对照研究,其中英文17篇、中文7篇(包括1篇学位论文),累计病例组5 653例、对照组20 218例。文献内容涉及中国、英国、加拿大和澳大利亚等11个国家,分别发表在国内外17种杂志上。见表1。
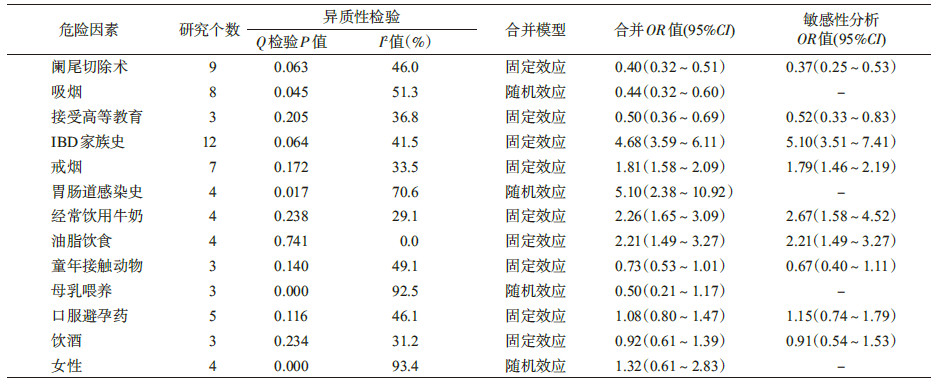
3. 主要病因相关因素的Meta分析:根据纳入文献的研究内容以及各相关因素可参考的文献数,选择阑尾切除术、吸烟、接受高等教育、IBD家族史、戒烟、胃肠道感染史、经常饮用牛奶、油脂饮食、童年接触动物、母乳喂养、口服避孕药、饮酒与女性13个相关因素,其中吸烟、胃肠道感染史、女性、母乳喂养4个因素在不同研究间存在异质性(P<0.05,I2≥50.0%),采用随机效应模型,其余9个因素使用固定效应模型。Meta分析显示,阑尾切除术、吸烟、接受高等教育为UC发病的保护因素,合并OR值(95%CI)分别为0.40(0.32~0.51)、0.44(0.32~0.60)、0.50(0.36~0.69);IBD家族史、戒烟、胃肠道感染史、经常饮用牛奶和油脂饮食为UC发病的危险因素,合并OR值(95%CI)分别为4.68(3.59~6.11)、1.81(1.58~2.09)、5.10(2.38~10.92)、2.26(1.65~3.09)和2.21(1.49~3.27)。见表2。
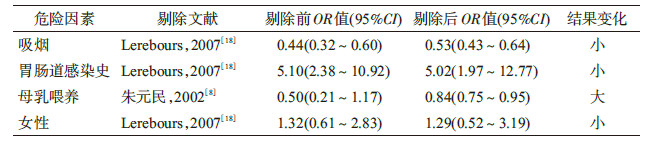
4. 敏感性分析:采用固定效应模型和随机效应模型分别对上述9个异质性检验无统计学意义的因素进行合并效应量计算,结果显示,合并效应量接近(表2);吸烟、胃肠道感染史、母乳喂养及女性4个因素异质性检验结果不同质,剔除文献质量评价较低的研究后,再次对各因素进行Meta分析,结果显示,吸烟、胃肠道感染史与女性因素剔除前后合并效应量无明显差异,说明研究结果相对稳定;而母乳喂养因素剔除前后结果变化较大(表3)。
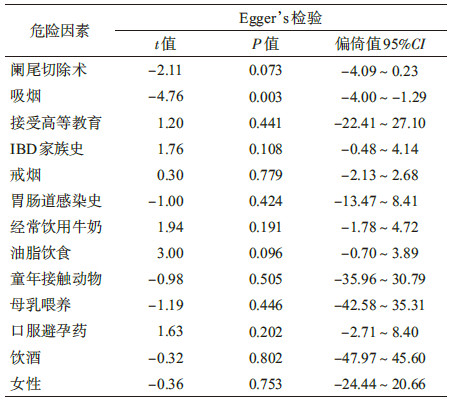
5.发表偏倚评估:采用Stata 12.0软件对UC病因相关因素进行Egger’s检验。结果显示,吸烟因素P=0.003,存在发表偏倚,其余12个相关因素P>0.05,受发表偏倚影响较小。见表4。
UC是一种多病因引起的消化系统常见疾病,其病因和发病机制尚不明确,近年来国内外开展了较多流行病学和病因学研究,以探讨UC发病的相关因素,但研究结果之间存在差异。Ponder和Long[29]在有关UC环境因素的综述中指出吸烟、高纤维饮食可减少患病的危险性,而口服避孕药、胃肠道感染史、油脂饮食、空气污染及城市生活环境则增加患UC的危险。Gearry等[21]开展的以人群为基础的病例对照研究发现IBD家族史与UC的发生显著相关,而吸烟、母乳喂养是UC的保护因素。中国UC协作组在国内一项多中心病例对照研究中发现[3],肠道感染与UC的发病有关,吸烟、饮茶及母乳喂养可减少患UC的风险,而口服避孕药、甜食、油脂饮食、受教育程度、阑尾切除术等与UC发病无关。本研究在整理以往研究结果的基础上,运用循证医学方法,对人群中UC发病的主要相关因素进行了系统评价。
Meta分析显示,胃肠道感染史、IBD家族史、油脂饮食、饮用牛奶与戒烟是UC发病的主要危险因素,其中胃肠道感染史与UC的相关性最强,可使正常人患UC的风险增加5.10倍。提示感染在UC发病机制中起重要作用,可能与微生物直接作用于黏膜免疫系统,启动免疫细胞[23],释放白介素-1、白介素-6、白介素-8和肿瘤坏死因子(TNF)等促炎细胞因子和炎性介质有关,最终引起肠黏膜炎症和损伤;或影响肠道菌群[3],细菌发生异位,破坏肠黏膜屏障功能,使其通透性增强[23],从而引发UC。
IBD家族史与UC也有较强的相关性,与国内外报道基本一致[3, 21]。有文献显示,UC与遗传因素的关系更密切,一级亲属的UC发病风险要远高于二、三级亲属[21]。因此应将IBD家族史的患者视为UC的高危人群,定期进行随访。
饮食结构与UC发病关系密切。目前普遍认为油脂饮食是UC发病的危险因素,但是牛奶与UC的关系还存在争议。本次Meta分析显示,油脂饮食与经常饮用牛奶均为UC发病危险因素。油脂饮食可以影响胆固醇代谢,使血液处于高凝状态,引起血管痉挛,影响结肠黏膜血液供应而造成结肠黏膜损伤[23]。但同时有研究提出,n-3多不饱和脂肪酸摄入可能减少UC发生的风险[30]。由于经常饮用牛奶的Meta分析纳入相关文献较少且均为国内研究,其结论比较片面,所以亟待开展大样本、多中心前瞻性研究。
近年来研究表明吸烟是UC发病的保护性因素,同时发现戒烟后2~5年发生UC的风险明显增加[31]。在对其机制的研究中发现烟碱可使活动期UC诱导缓解[32],并有学者提出对药物不敏感的UC患者可试行轻度吸烟作为治疗UC的替代疗法[30],但由于吸烟可能引起血管、呼吸道等疾病,所以替代疗法尚存争议。此外,本次Meta分析显示,吸烟与UC的关系可能存在发表偏倚,故该结论有待于今后进一步研究证实。
阑尾切除术可减少UC的发生[9, 15, 20, 24],是目前公认UC的保护因素。有研究发现在20岁之前进行阑尾切除术能够使UC的发病概率降低70%[24];在1篇17项病例对照研究的Meta分析中发现10岁之前行阑尾切除术减少UC发生的作用更显著[33]。其机制可能是减少促炎因子并上调白介素-10 和转化生长因子-β(TGF- β)等抗炎因子水平,抑制UC相关不良免疫反应。同时本次Meta分析发现接受高等教育与UC发病呈负相关,可能与这部分人群更注重健康生活方式及合理饮食结构等因素有关。
此外,母乳喂养、口服避孕药、饮酒、女性、童年接触动物在本次Meta分析中无统计学意义,其对UC的作用尚不能确定。原因可能是纳入研究文献样本量的限制难以达到统计学显著水平,或者相关研究因素自身差异较大,致使研究结果分歧较大。其中,母乳喂养与女性两个因素的异质指数均在90%以上,考虑与母乳喂养时间不一致、未区分女性患儿与成年女性患者、单篇文献结果对结论影响较大等相关。
本次Meta分析存在不足:①纳入文献都是公开发表,且大部分多因素数据分析文献只发表统计学有意义的结果,不能排除潜在的发表偏倚;②语种仅局限中文和英文,可能会漏检其他语种的相关文献;③部分因素纳入文献较少,结果不稳定,仍需进一步研究;④本文仅针对主要相关因素进行了Meta分析,对有些研究资料少的其他因素,无法进行综合分析。所以,结论的有效性尚需更多相关研究证实。
| [1] Molodecky NA,Soon IS,Rabi DM,et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time,based on systematic review[J]. Gastroenterology,2012,142(1):46-54. |
| [2] Ng SC,Bernstein CN,Vatn MH,et al. Geographical variability and environmental risk factors in inflammatory bowel disease[J]. Gut,2013,62(4):630-649. |
| [3] China Ulcerative Colitis Collaborative Group. A case-control study on the risk factors of ulcerative colitis[J]. Chin J Dig,2008,28(2):108-110. (in Chinese) 中国溃疡性结肠炎协作组. 溃疡性结肠炎危险因素的病例对照研究[J]. 中华消化杂志,2008,28(2):108-110. |
| [4] Spehlmann ME,Begun AZ,Saroglou E,et al. Risk factors in German twins with inflammatory bowel disease:results of a questionnaire-based survey[J]. J Crohn's Colitis,2012,6(1):29-42. |
| [5] He YH,Gao F,Lu JJ,et al. Analysis of risk factors of ulcerstive colitis in Xinjiang[J]. J Pract Med,2013,29(18):3070-3073. (in Chinese) 何玉环,高峰,卢加杰,等. 新疆地区溃疡性结肠炎发病的相关危险因素分析[J]. 实用医学杂志,2013,29(18):3070-3073. |
| [6] Inflammatory Bowel Disease Collaborative Group in Chinese Society of Gastroenterology. Consensus on the diagnosis and treatment specification of inflammatory bowel disease in In China[J]. Mod Digest Intervent,2008,13(2):139-145. (in Chinese) 中华医学会消化病学分会炎症性肠病协作组. 对我国炎症性肠病诊断治疗规范的共识意见[J]. 现代消化及介入诊疗,2008,13(2):139-145. |
| [7] Wells GA,Shea B,O'Connell D,et al. Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in Meta-analyses[EB/OL]. (2014-09-16)[2015-03-10]. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. |
| [8] Zhu YM,Wang QH,Liu YL,et al. Environmental risk factors in ulcerative colitis[J]. J Clin Intern Med,2002,19(5):350-352. (in Chinese) 朱元民,王勤河,刘玉兰,等. 溃疡性结肠炎环境因素致病作用的研究[J]. 临床内科杂志,2002,19(5):350-352. |
| [9] Abraham N,Selby W,Lazarus R,et al. Is smoking an indirect risk factor for the development of ulcerative colitis?An age-and sex-matched case-control study[J]. J Gastroenterol Hepatol,2003,18(2):139-146. |
| [10] Wang Y,Chen YD,Dang T,et al. A case-control study on the risk factors of ulcerative colitis[J]. Chin J Dig,2004,24(5):305. (in Chinese) 王英,陈言东,党彤,等. 溃疡性结肠炎危险因素的病例对照研究[J]. 中华消化杂志,2004,24(5):305. |
| [11] García Rodríguez LA,González-Pérez A,Johansson S,et al. Risk factors for inflammatory bowel disease in the general population[J]. Aliment Pharmacol Ther,2005,22(4):309-315. |
| [12] Baron S,Turck D,Leplat C,et al. Environmental risk factors in paediatric inflammatory bowel diseases:a population based case control study[J]. Gut,2005,54(3):357-363. |
| [13] Firouzi F,Bahari A,Aghazadeh R,et al. Appendectomy,tonsillectomy,and risk of inflammatory bowel disease:a case control study in Iran[J]. Int J Colorectal Dis,2006,21(2):155-159. |
| [14] Bernstein CN,Rawsthorne P,Cheang M,et al. A population-based case control study of potential risk factors for IBD[J]. Am J Gastroenterol,2006,101(5):993-1002. |
| [15] Jiang L,Xia B,Li J,et al. Risk factors for ulcerative colitis in a Chinese population:an age-matched and sex-matched case-control study[J]. J Clin Gastroenterol,2007,41(3):280-284. |
| [16] Sonntag B,Stolze B,Heinecke A,et al. Preterm birth but not mode of delivery is associated with an increased risk of developing inflammatory bowel disease later in life[J]. Inflamm Bowel Dis,2007,13(11):1385-1390. |
| [17] de Saussure P,Clerson P,Prost PL,et al. Appendectomy,smoking habits and the risk of developing ulcerative colitis:a case control study in private practice setting[J]. Gastroenterol Clin Biol,2007,31(5):493-497. |
| [18] Lerebours E,Gower-Rousseau C,Merle V,et al. Stressful life events as a risk factor for inflammatory bowel disease onset:A population-based case-control study[J]. Am J Gastroenterol,2007,102(1):122-131. |
| [19] Radon K,Windstetter D,Poluda AL,et al. Contact with farm animals in early life and juvenile inflammatory bowel disease:a case-control study[J]. Pediatrics,2007,120(2):354-361. |
| [20] López-Serrano P,Pérez-Calle JL,Pérez-Fernández MT,et al. Environmental risk factors in inflammatory bowel diseases. Investigating the hygiene hypothesis:a Spanish case-control study[J]. Scand J Gastroenterol,2010,45(12):1464-1471. |
| [21] Gearry RB,Richardson AK,Frampton CM,et al. Population-based cases control study of inflammatory bowel disease risk factors[J]. J Gastroenterol Hepatol,2010,25(2):325-333. |
| [22] Kaplan GG,Hubbard J,Korzenik J,et al. The inflammatory bowel diseases and ambient air pollution:a novel association[J]. Am J Gastroenterol,2010,105(11):2412-2419. |
| [23] Chen M,Wang CD. A case-control study on the risk factors of ulcerative colitis in Fujian province[J]. Chin J Gastroenterol Hepatol,2010,19(5):390-393. (in Chinese) 陈明,王承党. 福建省溃疡性结肠炎患病危险因素的病例对照研究[J]. 胃肠病学和肝病学杂志,2010,19(5):390-393. |
| [24] Wu W. Case-control study on the risk factors of Ulcerative colitis and UC-related polyps formation[D]. Wuhan:The Huazhong University of Science and Technology,2010. (in Chinese) 伍文. 溃疡性结肠炎发病及息肉形成危险因素的病例对照研究[D]. 武汉:华中科技大学,2010. |
| [25] Boneberger A,Weiss EH,Calvo M,et al. Environmental factors in infancy and ulcerative colitis in the Central South of Chile:a case-control study[J]. J Crohn's Colitis,2011,5(5):392-396. |
| [26] Ng SC,Woodrow S,Patel N,et al. Role of genetic and environmental factors in British twins with inflammatory bowel disease[J]. Inflamm Bowel Dis,2012,18(4):725-736. |
| [27] Zhang W,Liu ZZ,Han S,et al. A case-control study on the risk factors of ulcerative colitis in Shaanxi population[J]. J New Med,2012,22(2):110-113. (in Chinese) 张伟,刘真真,韩霜,等. 陕西地区人群溃疡性结肠炎发病危险因素的病例对照研究[J]. 医学新知杂志,2012,22(2):110-113. |
| [28] Jakobsen C,Paerregaard A,Munkholm P,et al. Environmental factors and risk of developing paediatric inflammatory bowel disease—a population based study 2007-2009[J]. J Crohn's Colitis,2013,7(1):79-88. |
| [29] Ponder A,Long MD. A clinical review of recent findings in the epidemiology of inflammatory bowel disease[J]. Clin Epidemiol,2013,5:237-247. |
| [30] Ananthakrishnan AN,Khalili H,Konijeti GG,et al. Long-term intake of dietary fat and risk of ulcerative colitis and Crohn's disease[J]. Gut,2014,63(5):776-784. |
| [31] Higuchi LM,Khalili H,Chan AT,et al. A prospective study of cigarette smoking and the risk of inflammatory bowel disease in women[J]. Am J Gastroenterol,2012,107(9):1399-1406. |
| [32] Bastida G,Beltrán B. Ulcerative colitis in smokers,non-smokers and ex-smokers[J]. World J Gastroenterol,2011,17(22):2740-2747. |
| [33] Koutroubakis IE,Vlachonikolis IG,Kouroumalis EA. Role of appendicitis and appendectomy in the pathogenesis of ulcerative colitis:a critical review[J]. Inflamm Bowel Dis,2002,8(4):277-286. |