 2015, Vol. 36
2015, Vol. 36文章信息
- 彭晓旻, 杨鹏, 吴双胜, 卢桂兰, 石伟先, 赵佳琛, 崔淑娟, 张代涛, 潘阳, 郭靖, 王全意.2015.
- Peng Xiaomin, Yang Peng, Wu Shuangsheng, Lu Guilan, Shi Weixian, Zhao Jiachen, Cui Shujuan, Zhang Daitao, Pan Yang, Guo Jing, Wang Quanyi.2015.
- 北京地区2011-2014年致儿童猩红热A组链球菌emm基因型别变化特征分析
- emm types of mutation in scarlet-fever-related group A streptococcal, among children in Beijing, 2011-2014
- 中华流行病学杂志, 2015, 36(12): 1397-1400
- Chinese Journal of Epidemiology, 2015, 36(12): 1397-1400
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2015.12.018
-
文章历史
- 投稿日期: 2015-03-17




猩红热是由A组链球菌(GAS)引起的急性呼吸道传染病,为我国法定报告乙类传染病。2011年4月香港地区出现猩红热暴发,其中2例儿童因中毒休克综合征死亡[1],同年在北京、上海等地也出现病例大幅增加和猩红热暴发[2, 3]。 M蛋白是GAS的主要毒力因子,决定GAS型特异性。编码M蛋白的emm基因(encoding mature M protein gene)具有5′端可变、3′端保守的特点,经PCR扩增及测序获emm基因的5′端可变区序列,通过与相关数据库比对,可确定emm型及亚型,以了解当地GAS的emm 型别分布和流行趋势及其调整应对的控制策略。为此本研究分析2011-2014年北京地区致猩红热GAS菌株emm型别分布及变化特点。
资料与方法1. 菌株和病例来源:自2011年起于北京市每年猩红热高发的5-7月在全市范围内开展病原学监测。16个区/县每个至少选取2家报告猩红热病例较多的医院作为监测哨点,共计36家医院,采集儿科门/急诊临床诊断为猩红热病例(按中华人民共和国卫生行业标准 WS 282-2008)咽拭子标本。病例监测数据选取中国疾病预防控制中心《疾病监测信息报告管理系统》中北京市2011-2014年1-12月的猩红热病例报告数据。
2. 菌株分离鉴定:将咽拭子标本接种哥伦比亚血琼脂平板,划线分离,37 ℃ 5% CO2孵箱中培养过夜,挑取具有β溶血可疑菌分纯后进行革兰染色,VETEK-2仪器及GP生化卡生化鉴定为酿脓链球菌,A~F血清分群试剂鉴定为A群。
3. emm分型:分离的GAS菌株按照美国疾病预防控制中心网站(http://www.cdc.gov/streplab/protocol- emm-type.html)方法,提取待测菌DNA后经通用引物PCR扩增,扩增产物测序,测序序列通过与网站数据库比对实现GAS的emm分型。通用引物序列:上游引物1:5′-TATT (C/G) GCTTAGAAAATTAA-3′,下游引物:5′-GCAAGTTCTTCAGCTTGTTT-3′。反应体系为50 μl,包括水37 μl,缓冲液5 μl ,dNTP 1.5 μl,引物1、2各0.5 μl,Taq酶0.5 μl,5 μl DNA模板。PCR反应条件: 95 ℃预变性5 min,95 ℃变性20 s,50 ℃退火45 s,72 ℃延伸90 s,30个循环;72 ℃延伸5 min。PCR产物纯化及测序委托上海英潍捷基生物技术有限公司完成。
4. 统计学分析:数据分析采用SPSS 16.0软件,Excel 2007软件绘制图表。显著性分析采用χ2检验,以P<0.05为差异有统计学意义。
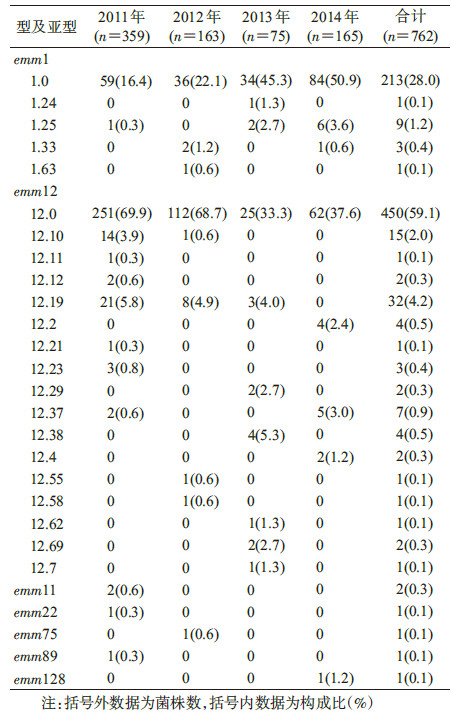
结 果1. 一般特征:2011-2014年北京市报告猩红热病例数分别为6 152、2 908、2 048和3 918例,最高为2011年,其次为2014年,2013年最低。2014年病例数较2013年增加91.31%,高于2007-2010年(非流行年份)平均水平,低于病例大幅增加的2011年。36家医院共采集疑似猩红热咽拭子样本2 161份,分离GAS菌株762株,阳性率为35.3%(762/2 161),2011-2014年分别为359、163、75和165株(表1)。

2. emm基因型别及分布:762株GAS共分为7个(1、11、12、22、75、89和128)emm基因型别。其中99.2%(756/762)为emm1(227株)和emm12 (529株),其他emm基因型别占0.8%(6/762),分别为emm11(2株)及emm22、75、89、128(各1株)。emm亚型22种,其中emm1型下5种亚型,emm12型下17种亚型。主要亚型为emm1.0(213株)和emm12.0(450株)占87.0%(663/762);其他emm亚型占12.2%(93/762)。不同年份亚型型别有变化,每年出现3~8种emm亚型,以emm12型下的亚型型别较多(表2)。
3. 不同年份emm型别构成及变化:2011年emm12占82.2%(295/359),emm1占16.7%(60/359),emm11、22、89占1.1%(4/359);2012年emm12占77.3%(123/163),emm1占23.9%(39/163),emm75占0.6%(1/163);2013年emm12占50.7%(38/75),emm1占49.3%(37/75),无其他型别;2014年emm12占44.2%(73/165),emm1占55.2%(91/165),emm128占0.6%(1/165)。2011-2014年emm基因型别构成比变化差异有统计学意义(P<0.001)。见图1。

|
| 图 1 2011-2014年北京地区致猩红热GAS菌株 emm基因型别构成 |
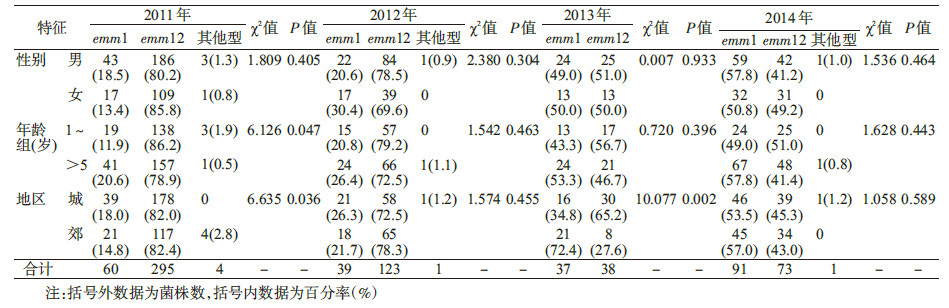
4. 不同年份emm型别感染人群特征分布:监测期间只有2011年emm基因型存在年龄差异,1~5岁组感染emm12型高于>5岁组,差异有统计学意义(P<0.05);2011年城区人群感染emm1型高于郊区,而2013年城区人群感染emm1型又低于郊区,两年份不同地区人群间的差异有统计学意义(P<0.05),2012和2014年emm基因型别差异无统计学意义(P>0.05);2011-2014年emm基因型分布的性别差异无统计学意义(P>0.05)。见表3。
基于PCR的emm基因分型技术已成为GAS分型金标准[4]。emm基因数据库已命名200余种emm基因型和1 000多种emm基因亚型。尽管emm基因型别多,但一个国家和地区不同年份出现的主要流行型别不会太多,且各国和地区流行的型别也不尽相同[5, 6, 7, 8]。本研究2011-2014年北京地区致猩红热GAS菌株emm基因型别少而相对集中,主导型别仅为emm12、emm1两种,占99.2%;其他5种型别(11、22、75、89、128)仅占0.8%,与我国既往报道emm1、emm12为主要优势基因型相同[9, 10, 11],但与国外报道不同[12],说明emm基因型分布存在地理差异。
北京地区2011年emm12为主导基因型,2014年主导型别转换,emm1成为主导基因型。台湾地区2001-2012年在不同年间emm12、emm1、emm4变换成为主导基因型[13],本文监测结果与其相似。猩红热的传染源是其病例和带菌者,当2011年猩红热以emm12基因型作为主导菌株流行时,人群对该型别菌株免疫力逐渐增加,此时 emm1基因型菌株被抑制,但针对emm1基因型菌株的易感人群却逐渐累积增多,由于易感人群未接种疫苗,经过一定时间,造成emm1主导基因型的猩红热再次发病,即本文分析中出现的2011-2014年emm12基因型流行逐渐减少,而emm1基因型流行逐渐增加。这也在一定程度上解释了既往报道北京地区猩红热发病具有周期性和在某个时间出现病例异常增高的现象[14]。但目前emm基因主导型别转换的时间周期尚不清楚。
本次分析发现2011-2014年北京地区emm基因型别构成比变化与相关年份猩红热病例变化存在一定关系。当2011年病例大幅增加达最高峰时,emm12(82.2%,相比emm1型仅占16.7%)以绝对优势作为主导流行菌型;随着2012年病例数下降,emm12下降至77.3%(emm1相对上升至23.9%);2013年病例数降至最低时,emm12和emm1构成比基本持平; 随着2014年病例数增加(超过2012年但不及2011年),emm型别转换,emm1型成为主导菌型。发现当猩红热高流行年份或病例数增多时,一种emm基因型占据优势主导地位,如2011年北京、香港、上海等地区报道猩红热流行和暴发,均是以emm12为主导基因型[1, 2, 3]。低流行年份或病例低水平时,如2013年,emm型别构成比趋于基本平衡,台湾地区一项研究也表明emm主导型别变化与猩红热流行变化趋势有关[13]。
分析中还发现2011年北京地区1~5岁组emm12高于>5岁组,除了与2011年当地以emm12高流行年份有关外,也证实了既往报道的emm12型随年龄增加呈下降趋势,低年龄组人群来源的GAS更容易表现emm12型[15]。2011年和2013年出现城、郊区来源上emm基因型别差异,除该两年份分别是当地病例数最高和最低年份外,是否存在其他因素还有待商榷。
综上所述,2011-2014年北京地区致猩红热流行GAS菌株优势菌型为emm12和emm1;不同年份emm12、emm1变换成为主导菌型;emm主导菌型变化与猩红热病例变化趋势有关。
| [1] Hsieh YC,Huang YC. Scarlet fever outbreak in Hong Kong,2011[J]. J Microbiol Immunol Infect,2011,44(6):409-411. |
| [2] Yang P,Peng X,Zhang D,et al. Characteristics of group A Streptococcus strains circulating during scarlet fever epidemic,Beijing,China,2011[J]. Emerg Infect Dis,2013,19(6):909-915. |
| [3] Chen M,Yao W,Wang X,et al. Outbreak of scarlet fever associated with emm12 type group A Streptococcus in 2011 in Shanghai,China[J]. Pediatr Infect Dis,2012,31(9):158-162. |
| [4] Zheng MH,Zhang JZ. A review on the advancement and application of group A Streptococcus genotyping[J]. Chin J Epidemiology,2008,29(8):840-842. (in Chinese) 郑明寰,张建中. A组链球菌基因分型方法最新进展及应用[J].中华流行病学杂志,2008,29(8):840-842. |
| [5] Shulman ST,Tanz RR,Dale JB,et al. Seven-year surveillance of North American pediatric group A streptococcal pharyngitis isolates[J]. Clin Infect Dis,2009,49(1):78-84 |
| [6] Tanaka D,Gyobu Y,Kodama H,et al. emm typing of group A Streptococcus clinical isolates:identification of dominant types for throat and skin isohtes[J]. Microbiol Immunol,2002,46(7):419-423. |
| [7] Ho PL,Johnson DR,Yue AW,et al. Epidemiologic analysis of invasive and noninvasive group A streptococcal isolates in Hong Kong[J]. J Clin Microbiol,2003,41(3):937-942. |
| [8] O'Brian KL,Beall B,Barrett NL,et al. Epidemiology of invasive group A Streptococcus disease in the United States,1995-1999[J]. Clin Infect Dis,2002,35(3):268-276. |
| [9] Wu PC,Lo WT,Chen SJ,et al. Molecular characterization of group A streptococcal isolates causing scarlet fever and pharyngitis among young children:a retrospective study from a northern Taiwan medical center[J]. J Microbiol Immunol Infect,2014,47(4):304-310. |
| [10] Liang Y,Liu X,Chang H,et al. Epidemiological and molecular characteristics of clinical isolates of Streptococcus pyogenes collected between 2005 and 2008 from Chinese children[J]. J Med Microbiol,2012,61(Pt 7):975-983. |
| [11] Liang Y,Shen X,Huang G,et al. Characteristics of Streptococcus pyogenes strains isolated from Chinese children with scarlet fever[J]. Acta Paediatr,2008,97(12):1681-1685. |
| [12] Shea PR,Ewbank AL,Gonzalez-Lugo JH,et al. Group A Streptococcus emm gene types in pharyngeal isolates,Ontario,Canada,2002-2010[J]. Emerg Infect Dis,2011,17(11):2010-2017. |
| [13] Chiou CS,Wang YW,Chen PL,et al. Association of the shuffling of Streptococcus pyogenes clones and the fluctuation of scarlet fever cases between 2000 and 2006 in central Taiwan[J]. BMC Microbiol,2009,9:115. |
| [14] Qian HK,Yang P,Zhang Y,et al. Spatial-temporal scan statistic on scarlet fever cases in Beijing,2005-2010[J]. Dis Surveill,2011,26(6):435-438. (in Chinese) 钱海坤,杨鹏,张奕,等. 2005-2010 年北京市猩红热发病时空扫描分析[J]. 疾病监测,2011,26(6):435-438. |
| [15] Jaggi P,Tanz RR,Beall B,et al. Age influences the emm type distribution of pediatric group A streptococcal phary isolates [J].Pediatr Infect Dis,2005,24(12):1089-1092. |