 2015, Vol. 36
2015, Vol. 36文章信息
- 冯一冰, 王棵, 王定明, 董芬, 余杨文, 潘利, 李凌, 刘涛, 曾宪嘉, 孙良先, 朱广瑾, 冯逵, 平波, 许可, 庞兴龙, 陈婷, 潘慧, 马瑾, 钟勇, 王璐, 单广良.
- Feng Yibing, Wang Ke, Wang Dingming, Dong Fen, Yu Yangwen, Pan Li, Li Ling, Liu Tao, Zeng Xianjia, Sun Liangxian, Zhu Guangjin, Feng Kui, Ping Bo, Xu Ke, Pang Xinglong, Chen Ting, Pan Hui, Ma Jin, Zhong Yong, Wang Lu, Shan Guangliang.
- 贵州地区汉族居民糖尿病患病情况及相关危险因素研究
- Prevalence and associated risk factors of diabetes among ethnic Han residents in Guizhou
- 中华流行病学杂志, 2015, 36(11): 1220-1225
- Chinese Journal of Epidemiology, 2015, 36(11): 1220-1225
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2015.11.008
-
文章历史
- 投稿日期: 2015-05-21




2. 北京协和医学院基础学院流行病与卫生统计学系;
3. 贵州省疾病预防控制中心;
4. 贵州省龙里县疾病预防控制中心;
5. 北京协和医院
2. Peking Union Medical College and Chinese Academy of Medical Science;
3. Guizhou Provincial Center for Disease Control and Prevention;
4. Longli County Center for Disease Control and Prevention;
5. Peking Union Medical College Hospital
糖尿病是由多种病因引起的代谢紊乱。全球范围内,约9%的18岁以上成年人患有糖尿病[1],至2035年全球糖尿病患者将达到5.92亿人[2]。2030年糖尿病将成为第七大主要死因[3]。据统计,由糖尿病直接导致的死亡中,80%以上发生在低收入和中等收入国家[4]。我国是糖尿病疾病负担较重的国家[5],2002年我国18岁以上城市人口糖尿病患病率为4.5%,农村为1.8%;2010年研究发现中国18岁以上人群糖尿病患病率达到9.7%[若同时以糖化血红蛋白(HbA1c)作为诊断指标,则患病率为11.6%][6],再次证实我国可能成为世界上糖尿病患者数最多的国家之一。FPG是衡量人群中糖尿病患病状况的直接指标。本研究调查贵州地区20~80岁汉族居民FPG水平分布及糖尿病相关影响因素。
对象与方法1. 研究对象:2012年10-12月年龄在20~80岁、在调查地居住一年及以上的汉族居民。
2. 研究方法:
(1)抽样方法:采用现况研究,在贵州地区结合当地经济发展水平,采用整群抽样,城镇以居委会为单位,农村以自然村为单位,按照当地提供调查地区的居委会和自然村名单,随机抽取一定数量的居委会和自然村;按照当地人口性别、年龄构成,计算各年龄人口应调查人数,在随机抽出的居委会/自然村中抽取符合条件的研究对象。获得被调查对象的知情同意后,在社区卫生服务中心或乡镇卫生院进行问卷调查和体格检查。
(2)调查内容:包括问卷调查、体格检查和实验室检测。问卷调查内容包括:人口学特征、社会经济状况、家族疾病史、个人疾病史、行为因素等;体格检查指标包括:身高、体重和血压;实验室检测:FPG、血脂生化指标检测(TC、TG、HDL-C、LDL-C)。
(3)诊断标准:①糖尿病:根据ADA 2014年糖尿病诊断标准[7, 8],将糖尿病患者定义FPG≥7.0 mmol/L或既往由县级以上医院诊断为糖尿病者。②高血压:根据JNC 2014版[9],将高血压定义为,SBP≥140 mmHg和/或DBP≥90 mmHg(1 mmHg=0.133 kPa),或既往由县级以上医院诊断为高血压者。③血脂异常:根据《中国成人血脂异常防治指南(2007版)》,将TG≥2.26 mmol/L定义为高TG血症;TC≥6.22 mmol/L定义为高TC血症;HDL-C<1.04 mmol/L定义为低HDL-C血症;LDL-C≥4.14 mmol/L定义为高LDL-C血症;符合上述其中1项及以上者即为血脂异常。④BMI:参照1999年WHO分类标准[10],按BMI(kg/m2)水平将人群分为偏瘦(BMI<18.5)、正常(18.5≤BMI<25)、超重(25≤BMI<30)和肥胖(BMI≥30)。
(4)其他相关指标的定义:①吸烟:调查时连续或累计吸烟半年及以上定义为“吸烟”。②饮酒:平均每周饮用一次,定义为“饮酒”[11]。③体力劳动情况:“轻体力劳动”指以静坐伏案少量走动为主的工作,如办公室工作人员等;“中体力劳动”指在校学习、机动车驾驶、电工安装等有一定活动量;“重体力劳动”指手工农业劳动、炼钢、伐木等活动量很大。④身体锻炼:以平均每次锻炼20 min及以上(包括跑步、游泳、健身和步行等)为标准,“经常”指每周锻炼3~7 d;“偶尔”指每周≤2 d;“从不”指从不锻炼。⑤糖尿病家族史:指祖父母、外祖父母、父母和兄弟姐妹中有人患糖尿病。⑥糖尿病知晓率=调查时已知自己患病的患者例数/本次调查符合诊断标准的所有糖尿病患者例数。⑦糖尿病治疗率=参与治疗的糖尿病患者例数/调查时已知晓自己患病的糖尿病患者例数。⑧糖尿病控制率=参与治疗的糖尿病患者中血糖得到控制(FPG<7.0 mmol/L)的患者数/参与治疗的患者数。
3. 统计学分析:采用SAS 9.2软件进行统计学分析。以性别、年龄和城乡为分层因素,根据2010年全国人口普查数据对患病率进行标化。计量资料用x±s表示,组间比较用t检验。计数资料用n(%)表示,组间比较用χ2检验。患病率的变化趋势采用趋势χ2检验,用logistic逐步回归法分析糖尿病的危险因素。
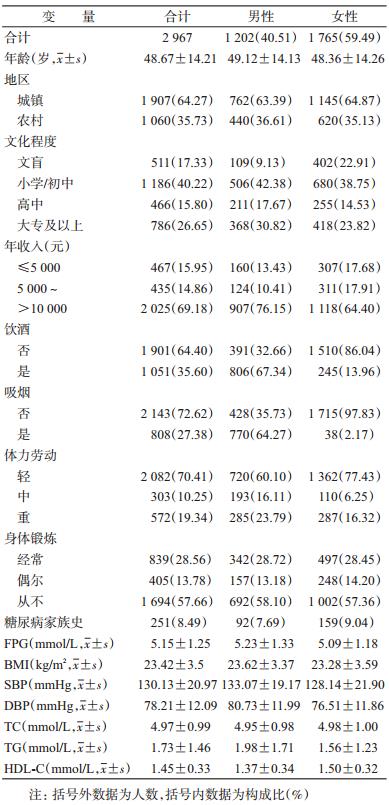
结 果1. 基本情况:本研究共调查城镇居民1 907人(64.27%)和农村居民1 060人(35.73%);男性1 202人(40.51%),女性1 765人(59.49%);平均年龄(48.67±14.21)岁;57.55%文化程度为初中及以下;69.18%家庭年收入超过10 000元;FPG平均值为(5.15±1.25) mmol/L。见表 1。
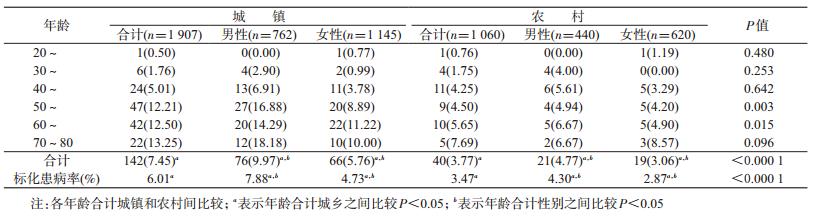
2. 患病情况:①城镇居民糖尿病标化患病率为6.01%(粗率7.45%),其中男性标化患病率7.88%(粗率9.97%)显著高于女性4.73%(粗率5.76%),P<0.001;相同性别下随年龄增长患病率升高,相同年龄组男性患病率与女性差异明显。②农村居民标化患病率为3.47%(粗率3.77%),其中男性标化患病率4.30%(粗率4.77%),女性2.87%(粗率3.06%),差异无统计学意义;相同性别居民随着年龄增长患病率均升高,相同年龄组不同性别间患病率差异不明显。③相同年龄性别下,≥40岁城镇居民患病率高于农村居民。见表 2。
3. 糖尿病知晓率、治疗率和控制率:调查结果显示,182名患者知晓自己患有糖尿病的知晓率为56.59%,知晓糖尿病治疗率为84.47%,控制率为41.38%。知晓率女性患者高于男性(P=0.039),城镇患者高于农村(P<0.001)。城乡不同性别糖尿病患者的治疗率和控制率的差异无统计学意义。见表 3。

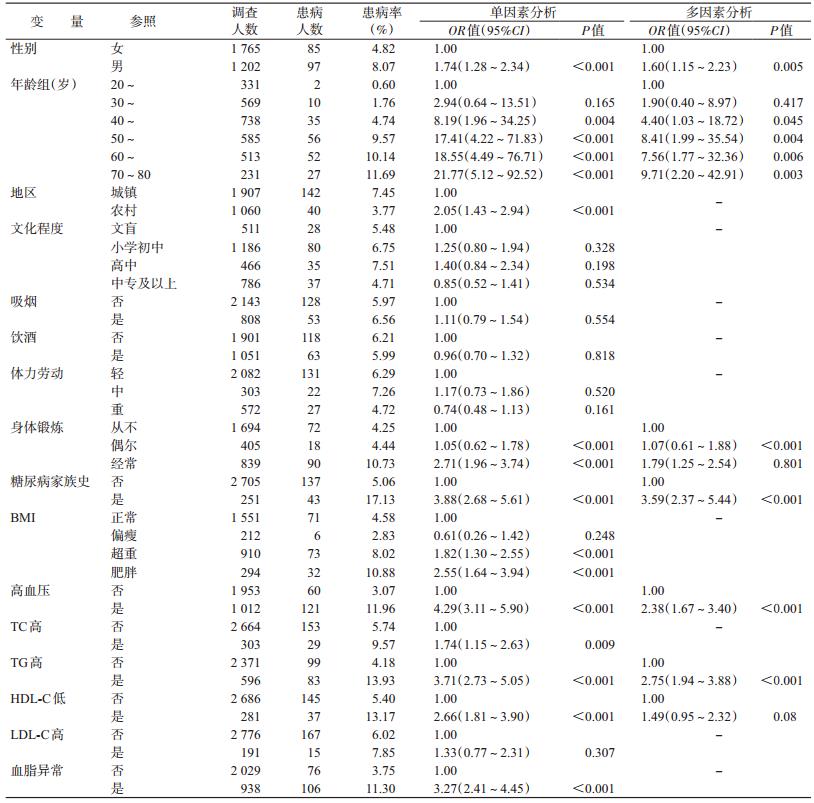
4. 糖尿病危险因素:多因素分析采用logistic逐步回归法,对全部变量进行筛选,入选标准α入=0.10,剔除标准α出=0.15。结果显示,男性发病风险是女性的1.60倍、年龄≥40岁发病风险升高、有糖尿病家族史(OR=3.59)、偶尔进行身体锻炼、高血压(OR=2.38)、高TG(OR=2.75)者糖尿病的发病风险增加(表 4)。
糖尿病已经成为我国重要的公共卫生问题,患病率在不断升高,疾病负担也已超过发达国家[12]。2002年我国18岁及以上居民糖尿病患病率仅为2.6%[13],2010年迅速上升到11.6%[6]。Yang等[5]报道我国20岁及以上成年人糖尿病患病率为9.7%,与本研究结果有差异。原因可能为:①调查地区、对象、抽样方法和数据分析方法不同;②本研究采用FPG值和既往诊断作为糖尿病诊断标准,上述调查采用了OGTT一步法;③近年糖尿病的防治工作加强,居民健康意识提高,可能导致横断面调查结果显示患病率降低。本研究中城镇居民患病率高于农村,男性患病率高于女性,患病率随着年龄增长呈上升趋势,这与以往研究 结果一致[13, 14, 15, 16, 17],提示应该针对人群的不同特点,积极开展相应的糖尿病筛查、防治工作。
知晓率、治疗率和控制率是反映糖尿病防治状况的有效指标。本研究中糖尿病患者知晓率、治疗率和控制率均高于2008年全国水平[18],但是低于近年国内外其他地区的研究[19]。提示调查地区糖尿病的防治工作可以围绕如何提高这三个有效指标开展,制定出切实有效的策略措施。
多因素分析显示:男性发病风险高于女性,年龄增加发病风险增加,有糖尿病家族史、高血压、高TG者糖尿病发病风险增加,进行身体锻炼糖尿病发病风险也高。男性患病风险高于女性,可能是因为调查中男性平均年龄大、BMI高、血脂异常率高,而以往研究表明[20],老龄化、脂代谢异常和肥胖是我国糖尿病流行的原因。另有研究表明[21, 22, 23],糖尿病合并高血压、血脂异常的发生率高,本研究中66.85%的糖尿病患者合并患有高血压,与以往研究结果相似。杨晨光和汪芳[24]研究发现,正常人血压升高糖尿病发病风险增加,高血压患者的血压得到控制糖尿病发病风险降低。有两种假说:①微血管功能异常是高血压和糖尿病共同的病理基础,这种异常在初期更容易表现为血压升高,所以高血压会早于糖尿病出现,也可以通过控制血压得到纠正[25]。②控制血压时使用的ACEI或ARB降压药物,能够对抗过度激活的RAS系统而缓解胰岛素抵抗,有效控制血糖,从而降低糖尿病的患病风险[26]。McGarry[27]提出,脂代谢异常是糖尿病及其并发症的原发性病理生理改变,可加重糖尿病危害程度[28]。本研究中血脂代谢异常者糖尿病患病率高,与既往研究结果一致[16, 29, 30]。本研究显示高TG增加糖尿病的发病风险,另有研究发现[31, 32],TG水平升高是糖尿病发病的独立危险因素,它通过游离脂肪酸干扰胰岛素在周围组织中与受体的结合,使其作用减弱。上述结果提示,糖尿病的防治应与高血压、血脂异常同时进行,糖尿病患者在控制血糖的同时也应注意血压和血脂等指标的变化。
适当的运动可以提高胰岛素敏感性[33]。但本研究显示偶尔进行身体锻炼糖尿病的患病风险高,这与张京等[34]研究结果相似,与其他研究 结果相悖[35, 36]。原因可能是,患者知晓自己病情后,对疾病的认识不断提高、更加注重身体锻炼和健康,所以患者中进行锻炼的比例高于正常人群,从而造成了身体锻炼增加发病风险的结果。
本研究存在一定的局限性。第一,横断面研究对危险因素与糖尿病因果关联的论证强度较弱;第二,本研究未采用OGTT法,会有一部分糖尿病患者漏诊[37],因此可能低估了调查地区的糖尿病患病率。
综上所述,调查地区20~80岁汉族居民糖尿病患病率较高,患者知晓率较低,半数以上患者治疗后血糖未达到控制水平。应在调查地区扩大人群糖尿病早期筛查,早发现、早治疗,并加强糖尿病防治知识的宣传教育,倡导健康的生活方式,在防控糖尿病的同时预防肥胖、高血压及血脂异常等代谢相关的疾病。
| [1] WHO. Global status report on noncommunicable diseases 2014[R]. Geneva:World Health Organization,2014. |
| [2] Guariguata L,Whiting DR,Hambleton I,et al. Global estimates of diabetes prevalence for 2013 and projections for 2035[J]. Diabetes Res Clin Pract,2014,103(2):137-149. |
| [3] WHO. Global status report on noncommunicable diseases 2010[R]. Geneva:World Health Organization,2011. |
| [4] WHO. Global health estimates:deaths by cause,age,sex and country,2000-2012[R]. Geneva:World Health Organization,2014. |
| [5] Yang WY,Lu JM,Weng JP,et al. Prevalence of diabetes among men and women in China[J]. N Engl J Med,2010,362(12):1090-1101. |
| [6] Xu Y,Wang LM,He J,et al. Prevalence and control of diabetes in Chinese adults[J]. JAMA,2013,310(9):948-959. |
| [7] WHO. Definition,diagnosis and classification of diabetes mellitus and its complications:report of a WHO consultation. Part 1,Diagnosis and classification of diabetes mellitus[R]. Geneva:World Health Organization,1999. |
| [8] American Diabetes Association. Diagnosis and classification of diabetes mellitus[J]. Diabetes Care,2014,37 Suppl 1:S81-90. |
| [9] James PA,Oparil S,Carter BL,et al. 2014 evidence-based guideline for the management of high blood pressure in adults:report from the panel members appointed to the Eighth Joint National Committee (JNC8)[J]. JAMA,2014,311(5):507- 520. |
| [10] WHO. Obesity:Prevention and managing the global epidemic:Report of a WHO consultation[R]. Geneva:World Health Organization,2000. |
| [11] Ma GS,Zhu DH,Hu XQ,et al. The drinking practice of people in China[J]. Acta Nutr Sin,2005,27(5):362-365. (in Chinese) 马冠生,朱丹红,胡小琪,等. 中国居民饮酒行为现况[J]. 营养学报,2005,27(5):362-365. |
| [12] Li YC,Liu XT,Hu N,et al. Disease burden on diabetes in China,2010[J]. Chin J Epidemiol,2013,34(1):33-36. (in Chinese) 李镒冲,刘晓婷,胡楠,等. 中国2010年糖尿病疾病负担[J]. 中华流行病学杂志,2013,34(1):33-36. |
| [13] Li LM,Rao KQ,Kong LZ,et al. A description on the Chinese national nutrition and health survey in 2002[J]. Chin J Epidemiol,2005,26(7):478-484. (in Chinese) 李立明,饶克勤,孔灵芝,等. 中国居民2002年营养与健康状况调查[J]. 中华流行病学杂志,2005,26(7):478-484. |
| [14] Guo JX,Zhu KX,Zhuang XX,et al. Study on the epidemiological characteristics and risk factors of diabetes among residents (≥15 years old) in Haizhu district of Guangzhou in 2010[J]. Chin J Prev Contr Chron Dis,2014,22(6):697-700. (in Chinese) 郭钜旋,朱凯星,庄晓霞,等. 2010年广州市海珠区15岁及以上居民糖尿病流行特征及危险因素分析[J]. 中国慢性病预防与控制,2014,22(6):697-700. |
| [15] Cheng GP,Dai TT,Liu Y,et al. Prevalence and related risk factors among residents with diabetes in urban and rural areas in Chengdu[J]. Chin J Epidemiol,2014,35(4):386-389. (in Chinese) 程改平,戴婷婷,柳园,等. 成都市城乡居民糖尿病患病率及影响因素研究[J]. 中华流行病学杂志,2014,35(4):386-389. |
| [16] Chen M,Li L,Zhao FX,et al. Analysis of relationship between type 2 diabetes and dyslipidemia in adults over 18 years old in Guizhou province[J]. Chin J Diabetes,2015,23(1):15-18. (in Chinese) 陈敏,李凌,赵否曦,等. 贵州省18岁以上成人2型糖尿病和血脂异常的关系分析[J]. 中国糖尿病杂志,2015,23(1):15-18. |
| [17] Zhao JB,Zhao YJ,Fu SY,et al. A cross-sectional study on impaired fasting glycaemia and diabetes mellitus in residents from Nangang district,Harbin city[J]. Chin J Epidemiol,2009,30(2):110-114. (in Chinese) 赵景波,赵玉娟,傅世英,等. 哈尔滨市南岗区社区居民空腹血糖受损和糖尿病的横断面研究[J]. 中华流行病学杂志,2009,30(2):110-114. |
| [18] Hu DS,Fu PY,Xie J,et al. Increasing prevalence and low awareness,treatment and control of diabetes mellitus among Chinese adults:the Inter ASIA study[J]. Diabetes Res Clin Pract,2008,81(2):250-257. |
| [19] Wang C,Yu YQ,Zhang XY,et al. Awareness,treatment,control of diabetes mellitus and the risk factors:survey results from Northeast China[J]. PLoS One,2014,9(7):e103594. |
| [20] Chinese Diabetes Association. Diagnosis and classification of type 2 diabetes mellitus for China(2013)[J]. Chin J Endocrinol Metab,2014,30(10):893-942. (in Chinese) 中华医学会糖尿病学分会. 中国2型糖尿病防治指南(2013年版)[J]. 中华内分泌代谢杂志,2014,30(10):893-942. |
| [21] Yang C,Guo ZR,Hu XS,et al. A prospective study on the association between control of blood pressure and incidence of type 2 diabetes mellitus[J]. Chin J Epidemiol,2010,31(3):260-263. (in Chinese) 杨晨,郭志荣,胡晓抒,等. 血压控制与糖尿病发病关系的前瞻性研究[J]. 中华流行病学杂志,2010,31(3):260-263. |
| [22] Williams B. The Hypertension in Diabetes Study (HDS):a catalyst for change[J]. Diabetic Med,2008,25 Suppl 2:13-19. |
| [23] Wang ZH,Wang LH,Li YC,et al. Current status of diabetes,hypertension and dyslipidemia among older Chinese adults in 2010[J]. Chin J Prev Med,2012,46(10):922-926. (in Chinese) 王志会,王临虹,李镒冲,等. 2010年中国60岁以上居民高血压和糖尿病及血脂异常状况调查[J]. 中华预防医学杂志,2012,46(10):922-926. |
| [24] Yang CG,Wang F. Blood pressure control strategy for hypertension and diabetes[J]. Chin J Clin Cardiol,2011,27(2):85-88. (in Chinese) 杨晨光,汪芳. 高血压伴糖尿病的血压控制策略[J]. 临床心血管病杂志,2011,27(2):85-88. |
| [25] Annerén C,Welsh M,Jansson L. Glucose intolerance and reduced islet blood flow in transgenic mice expressing the FRK tyrosine kinase under the control of the rat insulin promoter[J]. Am J Physiol Endocrinol Metab,2007,292(4):E1183-1190. |
| [26] Lembo G,Napoli R,Capaldo B,et al. Abnormal sympathetic overactivity evoked by insulin in the skeletal muscle of patients with essential hypertension[J]. J Clin Invest,1992,90(1):24- 29. |
| [27] McGarry JD. Banting lecture 2001:Dysregulation of fatty acid metabolism in the etiology of type 2 diabetes[J]. Diabetes,2002,51(1):7-18. |
| [28] Jin Y,Wang W. The influence of dyslipidemia on the diabetes onset and its associated risk factors[J]. Chin J Lab Diag,2011,15(5):860-862. (in Chinese) 金晔,王炜. 血脂异常对糖尿病发病及相关危险因素的影响[J]. 中国实验诊断学,2011,15(5):860-862. |
| [29] Zhang XJ,Li M,Gao S,et al. Relationship between metabolic syndrome and adipokines on diabetes among high-risk populations[J]. Chin J Epidemiol,2012,33(4):418-422. (in Chinese) 张秀娟,黎明,高珊,等. 糖尿病高危人群脂肪细胞因子与代谢综合征关系的研究[J]. 中华流行病学杂志,2012,33(4):418-422. |
| [30] Peng J,Xiong JF,Zhou H,et al. The control study on risk factors of high-risk population in diabetes[J]. Chin J Epidemiol,2004,25(6):506-508. (in Chinese) 彭绩,熊静帆,周华,等. 糖尿病高危人群风险因素对照研究[J]. 中华流行病学杂志,2004,25(6):506-508. |
| [31] Sane T,Taskinen MR. Does familial hypertriglyceridemia predispose to NIDDM?[J]. Diabetes Care,1993,16(11):1494- 1501. |
| [32] Wang F,Xin SN,Zhao SL,et al. Hyperlipemia as a risk factor of non-insulin dependent diabetes—An eight year prospective study of 137 cases of non-diabetic population[J]. Chin J Health Care Med PLA,2002,4(2):90-91. (in Chinese) 王峰,辛苏宁,赵淑兰,等. 高脂血症是非胰岛素依赖型糖尿病发病的危险因素——137例非糖尿病人群8年前瞻性观察[J]. 解放军保健医学杂志,2002,4(2):90-91. |
| [33] Zhao SX,Dong P,Gu Y. Diabetes melitus and physical activity[J]. Chin J Prev Contr Chron Dis,2004,12(1):46-48. (in Chinese) 赵守香,董鹏,顾湲. 糖尿病与运动[J]. 中国慢性病预防与控制,2004,12(1):46-48. |
| [34] Zhang J,Dong Z,Li G,et al. A cross-sectional study on risk factors of associated type 2 diabetes mellitus among adults in Beijing[J]. Chin J Epidemiol,2011,32(4):357-360. (in Chinese) 张京,董忠,李刚,等. 北京市居民2型糖尿病现况调查和危险因素研究[J]. 中华流行病学杂志,2011,32(4):357-360. |
| [35] Orozco LJ,Buchleitner AM,Gimenez-Perez G,et al. Exercise or exercise and diet for preventing type 2 diabetes mellitus[J]. Cochrane Database Syst Rev,2008(3):CD003054. |
| [36] Wang ZR. Evaluation of exercise interferential effects on diabetic patients in community[J]. Chin J Clin Rehabil,2002,6(15):2214-2215. (in Chinese) 王正荣. 运动干预社区2型糖尿病患者效果评估[J]. 中国临床康复,2002,6(15):2214-2215. |
| [37] Zhou XH,Ji LN. Fasting plasma glucose and HbA1c as a screening test for diabetes mellitus[J]. Chin J Diabetes,2005,13(3):203-205. (in Chinese) 周翔海,纪立农. 空腹血糖和糖化血红蛋白用于筛查糖尿病的研究[J]. 中华糖尿病杂志,2005,13(3):203-205. |