 2015, Vol. 36
2015, Vol. 36文章信息
- 王醴湘, 吕筠, 郭彧, 卞铮, 余灿清, 周汇燕, 谭云龙, 裴培, 陈君石, 陈铮鸣, 李立明.
- Wang Lixiang, Lyu Jun, Guo Yu, Bian Zheng, Yu Canqing, Zhou Huiyan, Tan Yunlong, Pei Pei, Chen Junshi, Chen Zhengming, Li Liming.
- 中国慢性病前瞻性研究:10个项目地区成年人超重/肥胖现况分析
- Regional specific differences in prevalence of overweight/obesity in China: findings from China Kadoorie Biobank study in 10 areas in China
- 中华流行病学杂志, 2015, 36(11): 1190-1194
- Chinese Journal of Epidemiology, 2015, 36(11): 1190-1194
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2015.11.002
-
文章历史
- 投稿日期: 2015-08-17




2. 中国医学科学院;
3. 国家食品安全风险评估中心;
4 .英国牛津大学临床与流行病学研究中心
2. Chinese Academy of Medical Sciences;
3. National Center for Food Safety Risk Assessment of China;
4. Clinical Trial Service Unit and Epidemiological Studies Unit (CTSU), Nuffield Department of Population Health, University of Oxford, UK
至2014年,全球超过19亿成年人超重,其中6亿以上处于肥胖状态[1]。近年来开展的中国人群肥胖水平调查大部分只报告调查对象总体或分城乡和人口社会学特征的指标水平,不同地区人群体格指标及肥胖水平特征比较相关研究较少[2, 3, 4, 5, 6, 7, 8]。本研究利用中国慢性病前瞻性研究(CKB)项目的基线调查(2004-2008年)数据描述项目覆盖的10个地区自然人群在不同体格指标下超重/肥胖现况的地区差异。
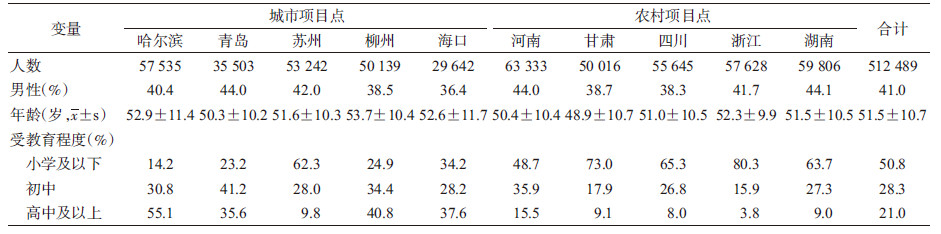
对象与方法1. 研究对象:CKB项目包括5个城市和5个农村地区。项目以街道或乡镇行政区为调查单位,根据当地社区户籍底册或登记确定调查点内所有符合入选要求的居民:年龄30~79岁,调查点内常住居民户口,无严重肢体残疾,能正常交流,自愿参加项目并签署知情同意书,且个体疾病及死亡登记报告归属当地卫生部门管理,具体参见文献[9, 10, 11]。为简化表述且方便识别,本研究以城市名称表示城市项目点,以省份名称表示农村项目点。有完整基线调查数据的调查对象共512 891人,剔除BMI值异常(BMI<15.0 kg/m2或BMI>50.0 kg/m2)的402人,最终纳入512 489人进入分析。
2. 研究内容:一般人口社会学信息(性别、年龄、受教育程度)通过调查员面对面询问获得。身高(身高仪)、体重(TANITA TBF-300GS体质构成分析仪)和WC(软皮尺)等体格指标由经过统一培训的调查员采用统一工具测量获得。测量WC时,皮尺置于髂前上嵴和第12肋下缘连线的中点水平环绕腹部。上述指标测量读数分别以cm或kg为单位,具体数值精确到0.1。进一步计算BMI(kg/m2)。本研究参考2006年《中国成人超重和肥胖症预防控制指南》[12]对体重和中心性肥胖进行判定:①根据BMI(kg/m2)进行体重分类:低体重(<18.5)、正常体重(18.5~)、超重(24.0~)、肥胖(≥28.0);②根据WC(cm)判定中心性肥胖:男性WC≥85.0,女性WC≥80.0。
3. 统计学分析:分性别和地区描述人群的体格指标特征,采用General linear model调整年龄,报告调整后的频数、百分比或均数、标准误。10个地区频数和均数间多重比较使用Bonferroni法。为方便与国内其他研究结果进行比较,以2010年全国人口普查数据作为标准人口,对总体结果进行年龄(10岁1组,共5组)标准化处理。分析使用SAS 9.3软件。
结 果1. 一般情况:共纳入分析512 489人,平均年龄(51.5±10.7)岁,男性占41.0%,农村地区个体占45.0%。研究对象基本特征见表 1。各地研究对象的性别(P<0.001)、年龄(P<0.001)、受教育程度(P<0.001)分布差异有统计学意义。
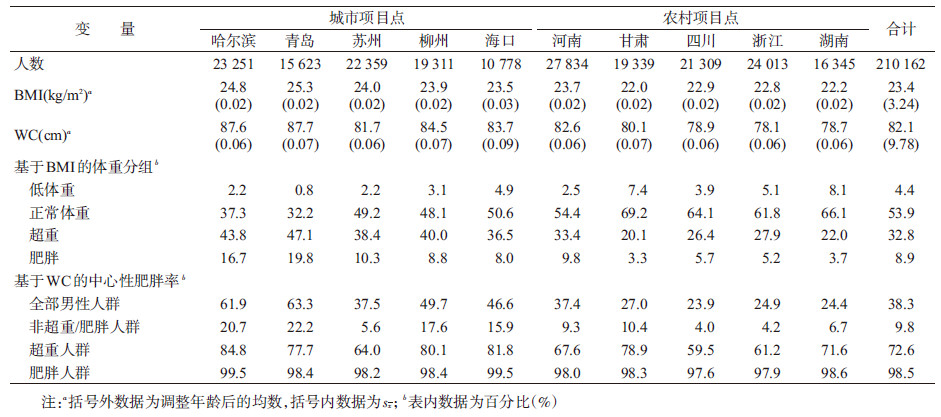
2. 体格指标:男性WC(82.1 cm)高于女性(79.1 cm),女性BMI(23.8 kg/m2)略高于男性(23.4 kg/m2)。10个地区中无论男女性,青岛项目点人群BMI均值最高(P<0.001),哈尔滨项目点人群WC均值最高(P<0.001);浙江和湖南项目点人群2个体格指标普遍较低(P<0.001),见表 2、3和图 1。
 |
| 注:U为城市项目点;R为农村项目点 图 1 10个CKB项目地区分性别BMI和WC平均水平 |
3. 基于BMI的超重/肥胖率:根据我国肥胖定义标准,10个地区中41.7%的男性和45.3%的女性处于超重/肥胖状态(表 2、3)。青岛项目点人群超重/肥胖率(男性为66.9%,女性为67.5%)高于其他项目点(P<0.001)。除河南省以外的4个农村项目点的超重/肥胖率普遍较低(表 2、3和图 2)。对年龄进行直接标准化后,10个地区人群总超重率为32.4%,肥胖率为10.4%。

 |
| 注:同图1 图 2 10个CKB项目地区人群基于BMI的超重/肥胖情况 |
4. 基于WC的中心性肥胖率:女性中心性肥胖率(44.6%)高于男性(38.3%)。各个项目点中,仍以青岛项目点人群中心性肥胖率最高(男性为63.3%,女性为64.9%)(P<0.001)。相比之下,四川、浙江和湖南项目点人群中心性肥胖率相对较低(P<0.001);其他项目点水平接近。标准化后10个地区人群总中心性肥胖率为40.0%。
5. 不同体重组人群的中心性肥胖率:在肥胖和超重人群中,男、女性中心性肥胖率分别为98.5%、98.3%和72.6%、73.5%。值得一提的是,在非超重/肥胖人群(BMI<24.0 kg/m2)中,仍有9.8%的男性和15.3%的女性达到中心性肥胖的标准;青岛和哈尔滨男性(P<0.001)以及青岛和甘肃女性(P<0.001)中心性肥胖更加突出(>20%),见表 2、3。在分析各个项目点中心性肥胖人群中不同体重组的构成情况时,男性中的14.9%和女性中的18.8%为非超重/肥胖人群(图 3)。
 |
| 注:同图1 图 3 10个CKB项目地区人群基于WC的中心型肥胖情况及其中不同体重组的构成 |
本研究显示,10个地区人群的BMI和WC以及基于这2个体格指标判定的超重/肥胖率和中心性肥胖率存在明显的地区差异。作为一项前瞻性队列研究,CKB项目并未采用概率抽样法选择研究地区和人群[10];其分析结果仅用以展示CKB项目募集到的队列成员在体格指标和超重/肥胖状况上的大体水平及存在的明显的地区差异。结果显示,CKB项目点人群的BMI和WC平均水平及超重/肥胖率与其他同类研究结果近似[1, 3, 7]。
在CKB的10个地区中,无论男女,青岛项目点人群的超重/肥胖问题都显得格外突出,近2/3的人群达到超重/肥胖和中心性肥胖标准。除此之外,超重/肥胖问题的地区差异在男性中更为明显;最高项目点和最低项目点可以相差近2倍。地区差异总体表现为,北方城市项目点人群最高,其次是南方城市项目点,除河南以外的农村项目点相对较低。在女性中,青岛和河南的超重/肥胖情况相比其他项目点更为突出一些。超重/肥胖的地区差异可能与地区经济发展水平、居民膳食习惯、体力活动类型、遗传背景等相关[8, 13, 14, 15, 16, 17]。
近年来的研究显示,相比用BMI判别的超重/肥胖,用WC、腰臀比或腰高比判别的中心性肥胖与胰岛素抵抗、代谢综合征、2型糖尿病以及心血管疾病等更为相关[18, 19, 20, 21, 22, 23, 24]。尤其是对于包括中国人在内的亚洲人群,相对身材较高的西方人而言,其腹部更容易堆积脂肪[8];因此亚洲人群基于BMI的超重/肥胖水平虽低于西方人群,其中心性肥胖情况却是一个不可忽略的问题[25]。本研究分析可见,即使是BMI属于非超重/肥胖的人群,仍有一定比例的个体达到中心性肥胖;尤其是在女性人群中,这一比例更高。换个角度来看,如湖南和甘肃项目点,其达到中心性肥胖标准的女性人群中,近1/3的个体的体重不超标。
本研究并未采用概率抽样法选择研究地区和人群,极端体重类型(过胖或过瘦)的人由于身体原因(伴有多种疾病或行动不便等原因)可能不会参加现场调查,使得调查人群可能存在一定的选择偏倚,对体重极端的人群代表不足。不过,考虑到我国极端体重(尤其是极端肥胖)的人相对较少,加之本研究分析时剔除了BMI为极端值的研究对象,对本研究结果造成的影响有限。本次分析的体格指标为测量而得,可能存在测量误差;但10个地区采用统一的测量工具和操作规程,可一定程度上控制测量误差。
本研究描述了CKB队列人群在体格指标和超重/肥胖情况上存在的明显地区差异。部分地区的人群超重/肥胖问题已经成为重要的公共卫生问题;而一些地区的女性虽然表现为体重平均水平较低,但中心性肥胖问题仍相对突出,也值得进一步关注。通过对这样超大规模的队列人群开展长期随访,将有机会深入探讨不同体格指标与众多健康结局的关联及其剂量反应关系。
| [1] WHO. Global Health Observatory (GHO) data[EB/OL]. [2015-08-01]. http://apps.who.int/gho/data/node.main.A896lang=en. |
| [2] Wang HJ, Wang ZH,Li Y,et al. The prevalent trend analysis of centricity obesity of nine provinces in China between 1993 and 2004 [J]. Food Nutr China,2007(6):47-50. (in Chinese) 王惠君,王志宏,李园,等. 1993-2004年中国九省成人中心性肥胖流行趋势分析[J]. 中国食物与营养,2007(6):47-50. |
| [3] Jiang Y,Zhang M,Li YC,et al. Prevalence of central obesity and distribution of waistline among Chinese adults in 2010[J]. Chin J Prev Contr Chron Dis,2013,21(3):288-291. (in Chinese) 姜勇,张梅,李镒冲,等. 2010年我国中心型肥胖流行状况及WC分布特征分析[J]. 中国慢性病预防与控制,2013,21(3):288-291. |
| [4] Yang XL,Zhang B,Zhang JG,et al. Trends of the changes in waist circumference distribution of Chinese adults in nine provinces:from 1993 to 2011[J]. Acta Nutr Sinica,2014,36(3):212-217. (in Chinese) 杨欣丽,张兵,张继国,等. 1993-2011年中国9省区成年人WC分布变化趋势[J]. 营养学报,2014,36(3):212-217. |
| [5] Yang XL,Wang HJ. The prevalence and influence factors of central obesity in adults[J]. Chin J Health Educ,2014,30(7):634-636. (in Chinese) 杨欣丽,王惠君. 成年人中心型肥胖的流行趋势及其影响因素[J]. 中国健康教育,2014,30(7):634-636. |
| [6] Li X,Wu J,Zuo SY,et al. Epidemiology of abdominal obesity[J]. Chin J Gerontol,2012,32(18):4105-4108. (in Chinese) 李欣,武静,左斯尧,等. 中心性肥胖的流行特征研究现状[J]. 中国老年学杂志,2012,32(18):4105-4108. |
| [7] Jiang Y,Zhang M,Li XY,et al. Prevelance of central obesity among adults with normal body weight in 2010[J]. Chin Prev Med,2013,14(6):449-453. (in Chinese) 姜勇,张梅,李晓燕,等. 2010年我国正常体重成年人中心型肥胖流行状况分析[J]. 中国预防医学杂志,2013,14(6):449-453. |
| [8] Ni GH,Zhang J,Zheng FT. Status and trends of Chinese obesity epidemic[J]. Food Nutr China,2013,19(10):70-74. (in Chinese) 倪国华,张璟,郑风田. 中国肥胖流行的现状与趋势[J]. 中国食物与营养,2013,19(10):70-74. |
| [9] Chen ZM,Lee LM,Chen JS,et al. Cohort profile:the kadoorie study of chronic disease in China (KSCDC)[J]. Int J Epidemiol,2005,34(6):1243-1249. |
| [10] Li LM,Lv J,Guo Y,et al. The China Kadoorie Biobank:related methodology and baseline characteristics of the participants[J]. Chin J Epidemiol,2012,33(3):249-255. (in Chinese) 李立明,吕筠,郭彧,等. 中国慢性病前瞻性研究:研究方法和调查对象的基线特征[J]. 中华流行病学杂志,2012,33(3):249-255. |
| [11] Chen Z,Chen J,Collins R,et al. China Kadoorie Biobank of 0.5 million people:survey methods,baseline characteristics and long-term follow-up[J]. Int J Epidemiol,2011,40(6):1652- 1666. |
| [12] Division of Disease Control,Ministry of Health of the People's Republic of China. The guideline for prevention and control of overweight and obesity in Chinese adults[M]. Beijing:People's Medical Publishing House,2006. (in Chinese) 中华人民共和国卫生部疾病控制司. 中国成人超重和肥胖症预防控制指南[M]. 北京:人民卫生出版社,2006. |
| [13] Wang H,Wang J,Liu MM,et al. Epidemiology of general obesity,abdominal obesity and related risk factors in urban adults from 33 communities of Northeast China:the CHPSNE study[J]. BMC Public Health,2012,12:967. |
| [14] Ogden CL,Yanovski SZ,Carroll MD,et al. The epidemiology of obesity[J]. Gastroenterology,2007,132(6):2087-2102. |
| [15] Dasgupta S,Salman M,Siddalingaiah LB,et al. Genetic variants in leptin:determinants of obesity and leptin levels in south indian population[J]. Adipocyte,2015,4(2):135-140. |
| [16] Saeed S,Bonnefond A,Manzoor J,et al. Genetic variants in LEP,LEPR,and MC4R explain 30% of severe obesity in children from a consanguineous population[J]. Obesity,2015,23(8):1687-1695. |
| [17] Locke AE,Kahali B,Berndt SI,et al. Genetic studies of body mass index yield new insights for obesity biology[J]. Nature,2015,518(7538):197-206. |
| [18] Macias N,Quezada AD,Flores M,et al. Accuracy of body fat percent and adiposity indicators cut off values to detect metabolic risk factors in a sample of mexican adults[J]. BMC Public Health,2014,14:341. |
| [19] Lee BJ,Kim JY. Predicting visceral obesity based on facial characteristics[J]. BMC Complement Altern Med,2014,14:248. |
| [20] Yusuf S,Anand S. Body-mass index,abdominal adiposity,and cardiovascular risk[J]. Lancet,2011,378(9787):226-227. |
| [21] Boggs DA,Rosenberg L,Cozier YC,et al. General and abdominal obesity and risk of death among black women[J]. N Engl J Med,2011,365(10):901-908. |
| [22] Du SM,Ma GS,Li YP,et al. Relationship of body mass index,waist circumference and cardiovascular risk factors in chinese adult[J]. Biomed Environ Sci,2010,23(2):92-101. |
| [23] Pischon T,Boeing H,Hoffmann K,et al. General and abdominal adiposity and risk of death in Europe[J]. N Engl J Med,2008,359(20):2105-2120. |
| [24] Wildman RP,Gu D,Reynolds K,et al. Are waist circumference and body mass index independently associated with cardiovascular disease risk in chinese adults?[J]. Am J Clin Nutr,2005,82(6):1195-1202. |
| [25] WHO Expert Consultation. Appropriate body-mass index for asian populations and its implications for policy and intervention strategies[J]. Lancet,2004,363(9403):157-163. |