 2015, Vol. 36
2015, Vol. 36文章信息
- 金霞, 熊燃, 毛宇嵘. 2014.
- Jin Xia, Xiong Ran, Mao Yurong. 2014.
- 2008-2013年我国医疗机构检测发现艾滋病病例情况分析
- HIV/AIDS cases detection in medical institutions from 2008 to 2013 in China
- 中华流行病学杂志, 2015, 36(4): 323-326
- Chinese Journal of Epidemiology, 2015, 36(4): 323-326
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2015.04.006
-
文章历史
- 投稿日期:2014-10-09




WHO 及联合国艾滋病规划署(UNAIDS)于 2007 年5 月联合发布《医疗机构医务人员主动提供 的检测与咨询(Provider-initiated HIV testing and counseling,PITC)指南》,要求医疗机构的医务人员 在遵循知情不拒绝(Opt-out)原则的前提下,主动向 就诊者提供艾滋病(Acquired immunodeficiency syndrome,AIDS)检测及咨询服务[1]。为发现更多的 艾滋病病毒感染者(Human immunodeficiency virus,HIV)和患者,我国于2008 年开始进一步在医疗机构 中推动PITC 策略。本研究根据2008-2013 年医疗 机构艾滋病检测和发现病例情况,分析我国医疗机 构开展该项工作的效果。 对象与方法
1. 调查对象:医疗机构检测人群包括术前检测、 受血(制品)前检测、性病门诊检测、其他就诊者检测 和孕产期检查的5 类就诊者。术前检测指各种手术 前开展的检查。受血(制品)前检测指除手术前开展 的检查以外的,对计划接受血或血液制品治疗者的 检查。性病门诊检测指来自性病门诊的样品。其他 就诊者检测指除性病门诊以外的其他门诊、住院患 者等的样品。孕产期检查指孕产期间的检查。
2. 调查方法:全国各级医疗机构医务人员对以 上5 类就诊者按照“知情不拒绝”的原则动员检测, 并做好检测前后的信息登记、咨询、上报和转介工 作。HIV 抗体检测工作按《全国艾滋病检测技术规 范(2009 年修订版)》执行。
3. 统计学分析:医疗机构检测发现数据来源于 国家艾滋病综合防治数据信息管理系统。使用 SAS 9.2 软件进行统计学分析。 结果
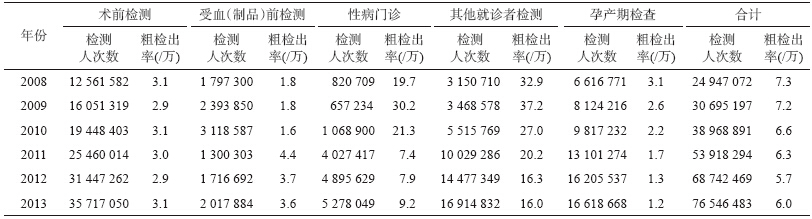
医疗机构通过主动提供艾滋病检测,每年检测 不断扩大,检测发现病例数相应增多。我国医疗机 构开展HIV抗体检测人次数从2008 年的2 494 万增 加至2013 年的7 654 万,增加了206.8%;检测发现病 例数从2008 年的18 241 例增加至2013 年的45 560 例,增加了149.8%;检测发现阳性率略有下降,2008 年为7.3/万,2013 年为6.0/万,见表 1。2008-2013年全国医疗机构HIV检测发现阳性率及检测发现病 例情况见图 1、2。
 |
| 图 1 2008-2013年全国医疗机构HIV检测发现阳性率情况 |
 |
| 图 2 2008-2013年全国医疗机构检测发现病例的构成情况 |
2008-2013 年医疗机构检测发现病例的CD4+T 淋巴细胞检测比例分别为19.7%、47.3%、55.5%、 66.1% 、74.7% 和81.5% ;医疗机构检测发现病例 CD4+T 淋巴细胞检测结果<350 cell/μl 的比例分别 为48.4%、68.1%、66.4%、65.5%、62.8%和61.2%。
1. 术前检测:2008-2013 年医疗机构通过术 前检测开展HIV 抗体检测人次数从1 256 万增加到 3 571 万,增加了184.3%;检测发现病例数从3 873 例 增加至10 944 例,增加了182.6%;2013 年的粗检出 率与2008 年持平,均为3.1/万。术前检测发现病例 占医疗机构发现病例的比例从2008 年的21.2%上升 至2013 年24.0%。
2. 受血(制品)前检测:2008-2013 年医疗机构 通过受血(制品)开展HIV抗体检测人次数从179 万 增加至201 万,增加了12.3%;检测发现病例数从329 例增加到724 例,增加了120.1%;粗检出率从2008年的1.8/万增加至2013 年的3.6/万。受血(制品)前 检测发现病例占医疗机构发现病例的比例从2008 年的1.8%下降至2013 年1.6%。
3. 性病门诊:2008-2013 年医疗机构通过性病 门诊开展HIV 抗体检测人次数从82 万增加到527 万,增加了543.1%;检测发现病例数从1 619 例增加 到4 830 例,增加了198.3%;粗检出率前两年出现上 升,随后略有下降后稳定于一个较高水平状态。性 病门诊检测发现病例占医疗机构发现病例的比例从 2008 年的8.9%上升至2013 年10.6%。
4. 其他就诊者检测:2008-2013 年医疗机构通 过其他就诊者检测开展HIV 抗体检测人次数从315 万增加到1 691 万,增加了436.9%;检测发现病例数 从10 376 例增加到27 143 例,增加了161.6%;粗检 出率前两年出现上升,随后下降并稳定于一个较高 水平状态。其他就诊者检测发现病例占医疗机构发 现病例的比例从2008 年的56.9% 上升至2013 年 59.6%。
5. 孕产期检查:2008-2013 年医疗机构通过孕 产期检查开展HIV抗体检测人次数从661 万增加到 1 661 万,增加了151.2%;检测发现病例数从2 044 例 下降为1 919 例,下降了6.1%;粗检出率从2008 年的 3.1/万下降至2013 年的1.2/万。孕产期检查发现病 例占医疗机构发现病例的比例从2008 年的11.2%下 降至2013 年4.2%。 讨论 WHO对17 个国家的调查显示,平均只有11% 的女性和10%的男性曾经接受过HIV 抗体检测并 获知检测结果[2],在中低收入国家,估计仅有20% 的HIV 感染者和患者知晓自己的感染状况[2, 3]。这 些结果促使PITC 策略的产生。对于在医疗机构实 施PITC 策略的效果,国内外有多项研究均表明, PITC 可有效提高HIV 检测咨询服务的可及性和覆 盖面[4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14]。此外,PITC 策略还有利于HIV 感染者的 早期发现[7, 12, 15, 16, 17]。
本研究显示,开展PITC 服务以后,医疗机构 HIV 检测人次数明显增加,发现病例数也显著增 加。医疗机构已经成为发现HIV感染者和患者的主 要来源,2008-2013 年,医疗机构检测发现病例占 全国检测发现病例的比例逐年上升,并稳定在较高 水平,依次为32.4%、36.0%、40.2%、45.3%、47.9%和 50.6%。其中,其他就诊者检测发现病例的比例维持 在50%以上,术前检测维持在20%以上。
研究结果还提示,2009 年全面铺开PITC服务以 后,性病门诊和其他就诊者检测病例阳性率出现上 升,随后稳定于一个较高水平状态,提示性病门诊和 其他就诊者检测扩大检测后,发现病例的效果较 好。而术前检测、受血(制品)前检测和孕产期检查 发现病例的阳性率,在2008-2013 年,一直相对平 稳,与多数省份已将此三类检测列为必检项目相 关。此外,2009 年开展PITC 后,医疗机构检测发现 病例的CD4+T淋巴细胞检测比例逐年上升,但 CD4+T淋巴细胞检测结果<350 cell/μl 的比例仍然 较高,维持在50%左右,提示医疗机构患者检测发现 晚,需进一步探讨促进艾滋病早检测的工作模式。
医疗机构主动为就诊者提供艾滋病检测咨询服 务,使筛查对象扩大至可能的高危人群,让更多隐匿 的感染者得到早期发现,进而获得及时的随访管理 和合理的抗病毒治疗,有效降低了死亡。然而,即使 医疗机构主动提供艾滋病检测咨询服务,如果就诊 者拒绝,依然不能落实检测。另外,由于传统的“症 状就医”观念,很多有过高危行为的人不在高危行为 后尽早就医检查,直至出现艾滋病相关症状,导致病 例晚发现比例高,影响治疗甚至由于错失治疗时机 而失去生命。因此,需要在医疗机构的重点科室中 积极推行HIV 常规检测服务,尤其艾滋病疫情严重 地区的医疗机构应尽早开展。
| [1] WHO. Guidance on Provider-initiated HIV testing and counselling in health facilities[R]. WHO, 2007. |
| [2] WHO. Towards universal access: scaling up priority HIV/AIDS interventions in the health sector:progress report[R]. 2008. Available at:http://www.who.int/hiv/pub/towards_universalaccess_report_2008.pdf. |
| [3] Demographic and Health Surveys[R]. Available at:http://www.measuredhs.com/. |
| [4] Ivers LC, Freedberg KA, Mukherjee JS. Provider-initiated HIV testing in rural Haiti:low rate of missed opportunities for diagnosis of HIV in a primary care clinic[J]. AIDS Research and Therapy. 2007, 4:28. |
| [5] Dalal S, Lee CW, Farirai T, et al. Provider-Initiated HIV Testing and Counseling:Increased Uptake in Two Public Community Health Centers in South Africa and Implications for Scale-Up[J]. PLoS One, 2011, 6(11):e27293. |
| [6] Natalie L, Pren N, Catherine M, et al. The impact of provider-initiated (opt-out) HIV testing and counseling of patients with sexually transmitted infection in Cape Town, South Africa:a controlled trial[J]. Implement Sci, 2010, 5:8. |
| [7] Silvestri DM, Modjarrad K, Blevins ML, et al. A comparison of HIV detection rates using routine opt-out provider-initiated HIV testing and counseling versus a standard of care approach in a rural African setting[J]. J Acquir Immune Defic Syndr, 2011, 56(1):e9-32. |
| [8] Kennedy CE, Fonner VA, Sweat MD, et al. Provider-initiated HIV testing and counseling in low-and middle-income countries:a systematic review[J]. AIDS Behav, 2012, 17(5):1571-1590. |
| [9] Hensen B, Baggaley R, Wong VJ, et al. Universal voluntary HIV testing in antenatal care settings:a review of the contribution of provider-initiated testing & counselling[J]. Trop Med Int Health 2012, 17(1):59-70. |
| [10] Roura M, Watson-Jones D, Kahawita TM, et al. Provider initiated testing and counselling programmes in sub-Saharan Africa:a systematic review of their operational implementation[J]. AIDS, 2013, 27(4):617-626. |
| [11] Wu J, Huang LF, Liu P, et al. Effect analysis of provider initiated testing and counseling in Zhangjiagang[J]. Jiangsu J Prev Med, 2013, 24(6):53-54. (in Chinese)吴洁, 黄莉芳, 刘萍, 等. 张家港市医务人员主动提供艾滋病检测咨询效果分析[J]. 江苏预防医学, 2013, 24(6):53-54. |
| [12] Zeng G, Lyu F, Luo X, et al. Comparison of effectiveness between two HIV screening strategies in outpatient setting[J]. Chin J Prev Med, 2013, 47(11):1010-1013. (in Chinese)曾刚, 吕繁, 罗夏, 等. 医疗机构门诊艾滋病筛查策略实施效果比较[J]. 中华预防医学杂志, 2013, 47(11):1010-1013. |
| [13] Sun Y, Wang QX, Liu P, et al. Acceptability and relevant impact factors of provider initiated testing counseling in Liangshan Yi autonomous prefecture of Sichuan province[J]. Chin J Epidemiol, 2012, 33(2):177-180. (in Chinese)孙研, 王启兴, 刘鹏, 等. 凉山彝族地区由医务人员主动提供艾滋病检测与咨询的可接受性及其影响因素调查[J]. 中华流行病学杂志, 2012, 33(2):177-180. |
| [14] Zeng G, Lyu F, Huang AL, et al. Study on the feasibility and effectiveness of strategy to provide HIV test for all outpatients with blood withdrawn for other tests in healthcare settings[J]. Pract Prev Med, 2012, 19(6):810-813. (in Chinese)曾刚, 吕繁, 黄爱林, 等. 门诊全部抽血患者艾滋病检测策略可行性及效果研究[J]. 实用预防医学, 2012, 19(6):810-813. |
| [15] Haukoos JS, Hopkins E, Conroy AA, et al. Routine opt-Out rapid HIV screening and detection of HIV infection in emergency department patients [J]. JAMA, 2011, 304(3):284-292. |
| [16] Kiene SM, Bateganya M, Wanyenze R, et al. Initial outcomes of provider-initiated routine HIV testing and counseling during outpatient care at a rural Ugandan hospital:risky sexual behavior, partner HIV testing, disclosure, and HIV care seeking[J]. AIDS Patient and STDs, 2010, 24(2):117-126. |
| [17] Kharsany AB, Karim QA, Karim SSA. Uptake of provider-initiated HIV testing and counseling among women attending an urban sexually transmitted disease clinic in South Africa-missed opportunities for early diagnosis of HIV infection[J]. AIDS Care, 2010, 22(5):533-537. |