 2015, Vol. 36
2015, Vol. 36文章信息
- 甘正凯, 李靖欣, 孟繁岳, 胡月梅, 姚学君, 张雪峰, 朱凤才. 2014.
- Gan Zhengkai, Li Jingxin, Meng Fanyue, Hu Yuemei, Yao Xuejun, Zhang Xuefeng, Zhu Fengcai. 2014.
- 肠道病毒71型所致疾病及其流行病学特征
- Epidemiological characteristics of enterovirus type 71 diseases
- 中华流行病学杂志, 2015, 36(1): 45-48
- Chinese Journal of Epidemiology, 2015, 36(1): 45-48
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2015.01.011
-
文章历史
- 投稿日期:2014-07-10




2. 江苏省疾病预防控制中心;
3. 南京医科大学公共卫生学院
2 Jiangsu Provincial Center for Disease Control and Prevention;
3 School of Public Health, Nanjing Medical University
肠道病毒(EV)71型(EV71)可引起手足口病、 疱疹性咽峡炎、非特异性发热及无菌性脑膜炎、脑 炎、肺炎、心肌炎等[1, 2, 3, 4],致残及病死率较高。以往关 于EV71的研究主要是针对手足口病常规监测、重症 患者分析或手足口病暴发调查,缺乏对EV71感染所 致疾病的全面系统了解。为此本研究对江苏省赣榆 县、射阳县、泰兴市、东海县、邳州市、宝应县及北京 市朝阳区部分6~35月龄儿童进行EV71感染所致 疾病的监测,了解EV71感染所致疾病的流行情况, 为综合防治提供依据。 对象与方法
1.样本来源:本研究是在EV71灭活疫苗Ⅲ期临 床试验监测阶段的基础上进行[5, 6],在研究现场建立 了涉及15个县/市级医院、64个镇卫生院、1115个村 卫生室的EV感染疾病监测系统,采取监护人主动报 告和被动就医相结合的方式,自2012年3月至2013 年2月对同期入组的10158名6~35月龄安慰剂组 受试者进行为期1年的队列随访,以研究人群的观 察人年以及确诊EV71感染所致疾病的病例数,计算 发病密度作为主要研究指标,系统调查EV71所致疾 病及其流行病学特征。本研究经江苏省疾病预防控 制中心伦理审查委员会审查批准,并经研究对象监 护人知情同意。
2. 标本采集:由于EV所致疾病临床表现复杂, 为保证检测的灵敏度,采用排除诊断方法,即在监测 期间,凡监测对象出现除外科疾病、先天性疾病、肿 瘤、精神行为障碍等有明确诊断的疾病外,其他未能 明确诊断或病因的症状、体征或疾病者均作为筛查 对象。由专业人员及时采集咽、肛拭子,进行EV71、 柯萨奇病毒A组16型(CA16)和肠道病毒通用型 (EV-G)特异性核酸检测。对于检测为EV71阳性病 例,采集症状期内粪便标本1份,症状期内每3天采 集1次咽拭子和肛拭子,症状结束后每7天采集1次 咽拭子和肛拭子,进行EV71特异性核酸检测,至连 续2次检测EV71均为阴性;同时收集该次病程观察 期内所有发病资料和流行病学资料。
3.实验室检测:
(1)病毒核酸检测:使用江苏默乐生物科技有限 公司提供的EV71、CA16及EV-G核酸检测试剂盒 (荧光PCR法)[注册证号:国食药监械(准)字2010 第3401300号]提取、检测病毒RNA。按说明书进行 操作及结果判定。
(2)病毒分离与鉴定:选择EV敏感细胞系RD 细胞(来源于人横纹肌肉瘤细胞)和Hep-2细胞(来 源于人喉癌上皮细胞),应用MEM生长液进行细胞 传代及培养。记录接种管和对照管细胞发生特征 性的细胞病变(CPE),对出现CPE标本,进行病毒 鉴定。
4. EV71病例定义:EV71感染所致疾病包括手 足口病、疱疹性咽峡炎、呼吸系统疾病、消化系统疾 病以及其他。病例诊断参照我国卫生部《手足口病 诊疗指南(2010版)》和《肠道病毒71型(EV71)感染 重症病例临床救治专家共识(2011年版)》,以及 WHO《Guidance for the clinical management of HFMD》和相关文献[7]。分类及临床诊断依据见表 1。在临床诊断的基础上各类病例确诊至少满足以 下条件之一:①EV71特异性核酸检测阳性;②分离 出EV,并鉴定为EV71。

5. 统计学分析:采用EpiData3.1软件进行数据 双录入,SPSS18.0软件进行统计学分析,分类资料 的比较采用χ2检验或Fisher确切概率法,非正态分布 的计量资料比较采用秩和检验,以P<0.05为差异 有统计学意义。 结 果
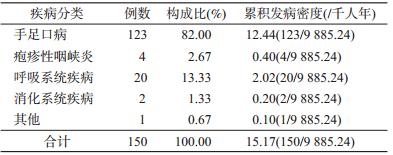
1. 病例概况:在1年的随访中,10158名监测对 象有566人存在不同程度的失访,累积观察9885.24 人年,共计报告150例EV71感染病例,其发病密度 为15.17/千人年(150/9885.24人年),其中手足口病 123例(82.00%,123/150)、疱疹性咽峡炎4例 (2.67%,4/150)、呼吸系统疾病20例(13.33%,20/ 150)、消化系统疾病2例(1.33%,2/150)、其他疾病1 例(0.67%,1/150),见表 2。报告重症病例9例,占总 发病儿童的6.00%(9/150),均为手足口病病例。
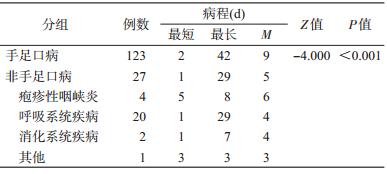
2. 临床特征:呼吸系统疾病主要包括上呼吸道 感染、流涕、咳嗽、咽痛,比例分别占65.0%(13/20)、 15.0%(3/20)、15.0%(3/20)、5.0%(1/20);消化系统疾 病主要包括腹泻、呕吐,比例分别占50.0%(1/2)、 50.0%(1/2);其他疾病包括单纯发热1例。EV71所 致疾病的病程为1~42(M=9)d;其中手足口病病 程为3~42(M=9)d,非手足口病病程为1~29(M= 6)d。手足口病与非手足口病病程的M值差异有统 计学意义(Z=-4.000,P<0.001),见表 3。
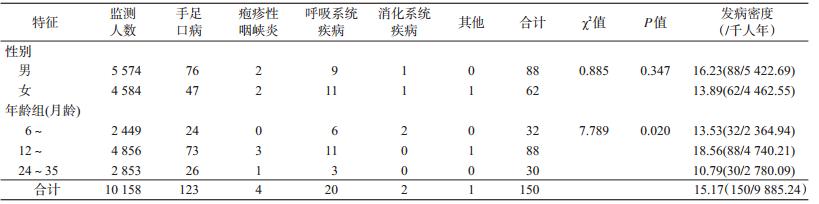
3. 流行病学特征:4、5、6月EV71感染所致疾 病的累积发病密度较高,分别为29.94/千人年(50/ 1669.84人年)、36.37/千人年(91/2501.98人年)、 33.91/千人年(113/3332.48人年),见图 1。所有的重 症病例均发生在此期间,分别占当月发病儿童的 5.88%(2/34)、12.20%(5/41)、9.09%(2/22)。EV71感 染所致疾病男童88例,女童62例,发病密度分别为 16.23/千人年(88/5422.69人年)、13.89/千人年(62/ 4462.55人年),差异无统计学意义(χ2=0.885,P= 0.347);6~、12~、24~35月龄3个年龄段儿童感染 EV71所致疾病分别为32、88、30例,发病密度分别 为13.53/千人年(32/2364.94人年)、18.56/千人年 (88/4740.21人年)、10.79/千人年(30/2780.09人 年),差异有统计学意义(χ2=7.789,P=0.020),见 表 4。重症病例男童7例,女童2例,分别占男女发 病儿童的7.95%(7/88)、3.23%(2/62),差异无统计学 意义(χ2=1.442,P=0.230)。3个月龄段重症病例分 别为1、7、1例,分别占各月龄段发病儿童的3.13% (1/32)、7.95%(7/88)、3.33%(1/30),差异无统计学意 义(χ2=1.443,P=0.486)。
 |
| 图 1 EV71感染发病风险的时间分布 |
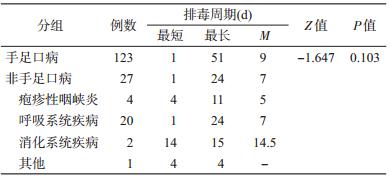
4. 排毒周期:所有病例排毒周期为1~51(M= 8)d。其中手足口病病例为1~51(M=9)d,非手足 口病病例1~24(M=11)d,两者排毒周期M值的差 异无统计学意义(Z=-1.647,P=0.103),见表 5。
Chang等[8]和Liu等[9]发现:EV71感染疾病以手 足口病(50%)、疱疹性咽峡炎(10%)、中枢神经系统 疾病(25.0%~45.0%)为主。Chen等[10]的研究显示, EV71感染疾病主要包括手足口病(78.4%)、疱疹性 咽峡炎(16.5%)和呼吸系统疾病(3.1%),与广东地 区的研究结果相似[11]。本研究发现EV71感染所致 疾病除大部分(82%)为手足口病外,还包括疱疹性 咽峡炎、呼吸系统疾病、消化系统疾病及其他疾病, 所占比例分别为2.67%、13.33%、1.33%、0.67%。据 此推测目前国家传染病网络报告和监测系统仅报告 手足口病可能会低估EV71所致疾病的发病风险。
本研究EV71感染所致疾病的发病密度为 15.17/千人年,6~11、12~23、24~35月龄3个年龄 段儿童发病密度分别为13.53/千人年、18.56/千人 年、10.79/千人年,以前2个年龄段儿童发病风险较 高,与台湾、广东、香港地区的报道类似[8, 12, 13, 14]。 EV71感染所致疾病的高发期为4~6月,与其他研 究报告相似[13, 14],重症病例的流行高峰与EV71感染 所致疾病的流行高峰基本一致。3个年龄段重症病 例在患儿中构成比的差异无统计学意义,但大部分 重症病例均出现在中低年龄组,与台湾地区报道 75%的重症病例发生在2周岁以下儿童的结论基本 一致[15]。因此,在EV71感染流行季节其防控重点应 关注中低年龄儿童及重症病例。
本研究EV71感染所致疾病的病程为1~42 (M=9)d,与台湾[16]、广东[13]及西安地区[17]报告的病 程有较大差异。手足口病与非手足口病病例病程的 M值差异有统计学意义,提示手足口病临床症状较 为严重,且所有重症病例均为手足口病,因此临床诊 疗过程中应重点关注手足口病,特别是重症病例。
本研究EV71感染所致疾病最长排毒周期与相 关文献报告相似[18, 19, 20]。Han等[21]随访观察34例 EV71感染的手足口病患儿排毒周期,发现在发病后 37~40d,20%的患儿粪便标本病毒核酸检测仍呈阳 性,粪便最长排毒时间为42d。潘浩等[22]报道EV71 临床感染病例的粪便排毒最长周期为8周,与张慎 荣等[23]的观察相似。手足口病与非手足口病病例排 毒周期M值的差异无统计学意义,提示除了手足口 病病例外,非手足口病病例同样也是EV71感染重要 传染源之一,目前尚未给予足够的重视。
| [1] | Roohandeh A, Rahimi P, Sohrabi A, et al. Frequency of human enterovirus 71 in children under 8 years old with aseptic menengitis in Tehran [J]. Clin Lab, 2012, 59(7/8):915-920. |
| [2] | Hao B, Gao D, Tang DW, et al. Distribution of human enterovirus 71 in brainstem of infants with brain stem encephalitis and infection mechanism [J]. J Forensic Med, 2012, 28(2):85-88, 91. (in Chinese)郝博, 高迪, 汤大为, 等. 肠道病毒71型在脑干脑炎婴幼儿脑干中的分布及感染机制[J]. 法医学杂志, 2012, 28(2):85-88, 91. |
| [3] | Chang LY, Lin TY, Hsu KH, et al. Clinical features and risk factors of pulmonary oedema after enterovirus-71-related hand, foot, and mouth disease[J]. Lancet, 1999, 354(9191):1682-1686. |
| [4] | Chan KP, Goh KT, Chong CY, et al. Epidemic hand, foot and mouth disease caused by human enterovirus 71, Singapore [J]. Emerg Infect Dis, 2003, 9(1):78. |
| [5] | Zhu FC, Meng FY, Li JX, et al. Efficacy, safety, and immunology of an inactivated alum-adjuvant enterovirus 71 vaccine in children in China:a multicentre, randomised, double-blind, placebo- controlled, phase 3 trial[J]. Lancet, 2013, 381:2024-2032. |
| [6] | Zhu F, Xu W, Xia J, et al. Efficacy, safety, and immunogenicity of an enterovirus 71 vaccine in China[J]. N Engl J Med, 2014, 370:818-828. |
| [7] | World Health Organization. A guide to clinical management and public health response for hand, foot and mouth disease (HFMD) [M]. World Health Organization, 2011:35-38. |
| [8] | Chang LY , Lin TY, Huang YH, et al. Comparison of enterovirus 71 and coxsackievirus A16 clinical illnesses during the Taiwan enterovirus epidemic, 1998[J]. J Pediatr Infect Dis, 1999, 18(12):1092-1096. |
| [9] | Liu CC, Tseng HW, Wang SM, et al. An outbreak of enterovirus 71 infection in Taiwan, 1998:epidemiologic and clinical manifestations [J]. J Clin Virol, 2000, 17(1):23-30. |
| [10] | Chen SP, Huang YC, Li WC, et al. Comparison of clinical features between coxsackievirus A2 and enterovirus 71 during the enterovirus outbreak in Taiwan, 2008:a children's hospital experience [J]. J Microbiol Immunol Infect, 2010, 43(2):99-104. |
| [11] | Sun LM, Zheng HY, Zheng HZ, et al. An enterovirus 71 epidemic in Guangdong province of China, 2008:epidemiological, clinical, and virogenic manifestations [J]. Jpn J Infect Dis, 2011, 64(1):13-18. |
| [12] | Lee MS, Chiang PS, Luo ST, et al. Incidence rates of enterovirus 71 infections in young children during a nationwide epidemic in Taiwan, 2008-09[J]. PLoS Neglect Trop Dis, 2012, 6(2):e1476. |
| [13] | Wu WH, Kuo TC, Lin YT, et al. Molecular epidemiology of enterovirus 71 infection in the central region of Taiwan from 2002 to 2012[J]. PLoS One, 2013, 8(12):e83711. |
| [14] | Ma E, Chan KC, Cheng P, et al. The enterovirus 71 epidemic in 2008—public health implications for Hong Kong[J]. Int J Infect Dis, 2010, 14(9):e775-780. |
| [15] | Chen KT, Chang HL, Wang ST, et al. Epidemiologic features of hand-foot-mouth disease and herpangina caused by enterovirus 71 in Taiwan, 1998-2005[J]. Pediatrics, 2007, 120(2):e244-252. |
| [16] | Chang LY. Enterovirus 71 in Taiwan [J]. Pediatr Neonatol, 2008, 49(4):103-112. |
| [17] | Nie XJ, Zhang GC, Li SX, et al. Clinical characteristics of enterovirus 71-associated hand-foot-mouth disease in Xi'an area [J]. J Clin Pediatr, 2010, 28(6):546-548. (in Chinese)聂晓晶, 张国成, 李思袖, 等. 西安地区EV71感染手足口病的临床特征[J]. 临床儿科杂志, 2010, 28(6):546-548. |
| [18] | Zhou LL. The research progress of enterovirus type 71 and hand, foot and mouth disease [J]. Chin Mater Child Health Care, 2013, 28(3):562-564. (in Chinese)周丽玲. 肠道病毒71型与手足口病的研究进展[J]. 中国妇幼保健, 2013, 28(3):562-564. |
| [19] | Li SJ. Entervirus 71 infective disease [J]. J Appl Clin Pediatr, 2008, 23(22):1780-1782. (in Chinese)李双杰. 肠道病毒71型感染性疾病[J]. 实用儿科临床杂志, 2008, 23(22):1780-1782. |
| [20] | Chung PW, Huang YC, Chang LY, et al. Duration of enterovirus shedding in stool [J]. J Microbiol Immunol Infect, 2001, 34(3):167-170. |
| [21] | Han J, Ma XJ, Wan JF, et al. Long persistence of EV71 specific nucleotides in respiratory and feces samples of the patients with Hand-Foot-Mouth Disease after recovery [J]. BMC Infect Dis, 2010, 10:178. |
| [22] | Pan H, Zhu YF, Qi X, et al. Analysis on the epidemiological and genetic characteristics of enterovirus type 71 and Coxsackie A16 virus infection in Jiangsu, China, 2008[J]. Chin J Epidemiol, 2009, 30(4):339-343.(in Chinese)潘浩, 朱叶飞, 祁贤, 等. 江苏省2008年某福利院手足口病暴发的流行病学和病原学特征研究[J]. 中华流行病学杂志, 2009, 30(4):339-343. |
| [23] | Zhang SR, Jia LH, Li GQ, et al. Clinical analysis and follow-up of 8 children who have hand, foot and mouth disease and acute flaccid paralysis [J]. Mod Pract Med, 2013, 25(7):806-808. (in Chinese)张慎荣, 贾黎红, 李光乾, 等. 手足口病合并急性弛缓性瘫痪患儿8例临床分析及随访[J]. 现代实用医学, 2013, 25(7):806-808. |