 2015, Vol. 36
2015, Vol. 36文章信息
- 邢爱君, 季春鹏, 施继红, 杜鑫, 黄喆, 林黎明, 熊海亮, 吴寿岭. 2014.
- Xing Aijun, Ji Chunpeng, Shi Jihong, Du Xin, Huang Zhe, Lin Liming, Xiong Hailiang, Wu Shouling. 2014.
- 理想心血管健康行为和因素与非酒精性脂肪肝的相关性研究
- Relationship between ideal cardiovascular behaviors/factors and the prevalence of nonalcoholic fatty liver disease
- 中华流行病学杂志, 2015, 36(1): 40-44
- Chinese Journal of Epidemiology, 2015, 36(1): 40-44
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2015.01.010
-
文章历史
- 投稿日期:2014-09-17




2. 河北联合大学研究生院
2 Graduate School, Hebei United University
非酒精性脂肪肝(NAFLD)是一种以无过量饮 酒史的肝实质细胞脂肪变性和贮积为特征的临床 病理综合征。随着肥胖和代谢综合征在全球的广 泛流行,其患病率逐年增长,已成为中国除病毒性 肝炎外的另一威胁人类健康的慢性肝病。有研究 显示,心血管疾病与NAFLD具有共同的危险因素 (如胰岛素抵抗、肥胖、脂代谢紊乱、不良生活行为 方式等)[1, 2]。2010年美国心脏病协会(AHA)提出 了心血管健康行为和因素的定义[3],包括4个行为指 标(吸烟、体育锻炼、BMI、饮食)和3个因素指标(血 脂、血 压、血 糖)。本 研 究 依 据 开 滦 研 究 资 料 (ChiCTR-TNC-11001489)分析理想心血管健康行 为和因素与NAFLD的关系。 对象与方法
1. 研究对象:2006年7月至2007年10月由开滦 医院、林西医院、赵各庄医院、唐家庄医院、范各庄医 院、吕家坨医院、荆各庄医院、林南仓医院、钱家营医 院、马家沟医院、开滦医院分院11家医院参加,对开 滦在职及离退休职工进行健康体检,共有101510名 职工(男81110名,女20400名)参加本次健康体 检。入选标准:①参加2006-2007年度健康体检者; ②无饮酒史者;③心血管各健康行为和因素指标完 整者;④同意参加本研究并签署知情同意书者。排 除以下病史者:①既往有心肌梗死;②既往有脑卒 中;③恶性肿瘤;④HBsAg阳性;⑤已诊断为肝硬化。
2.研究方法:
(1)一般资料:流行病学调查及人体测量方法 见文献[4]。心肌梗死病史、脑卒中史、恶性肿瘤史 定义为既往有二级甲等及以上医院的诊断依据。
(2)实验室检查:体检当日抽取调查对象空腹肘 静脉血5ml于EDTA真空管内,室温离心取上层血 清在4h内进行生化指标测量,方法见文献[4]。
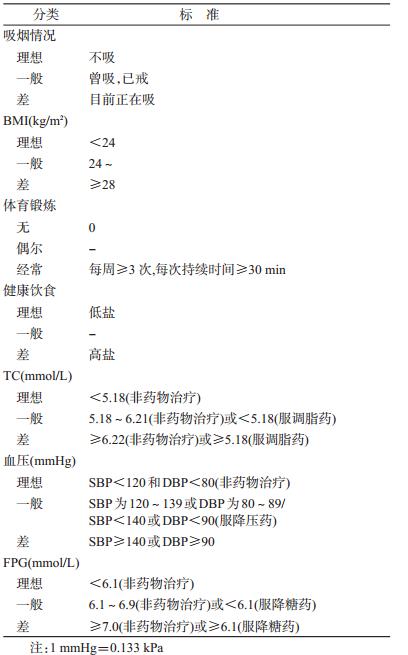
(3)心血管健康行为与因素定义:由于开滦研究 始于2006年,问卷中没有蔬菜摄入量,考虑到食盐 对中国人群心血管疾病的影响及胡大一教授提出的 心血管健康标准[5],研究将AHA健康行为定义中的 蔬菜摄入量改为食盐摄入量;问卷中有关运动的定 义与AHA定义略有不同,见表 1。
(4)NAFLD诊断标准:参照文献[6]。
3. 统计学分析:2006-2007年度健康体检数据 由各医院终端录入,通过网络上传至开滦医院计算 机室服务器,形成oracle10.2g数据库。由程序导出 形成DBF格式文件,采用SPSS13.0软件进行统计 学分析。所有正态分布的计量资料以x±s表示,多 组间比较采用单因素方差分析(两两比较用LSD 法)。因C反应蛋白(CRP)呈偏态分布,经对数转换 后再用方差分析进行组间比较,并用M(Q1~Q3)表 示。计数资料用百分率表示,组间比较应用χ2检 验。采用多因素logistic回归分析理想心血管健康 行为和因素与NAFLD的关系。以P<0.05(双侧检 验)为差异有统计学意义。 结 果
1. 一般情况:参加2006-2007年度健康体检的 研究对象共101510名,其中男性81110名,女性 20400名,心血管各健康行为和因素指标不完整者 4753名,饮酒者39350名,按入选标准共入选57407 名。排除既往心肌梗死病史者616例、既往脑卒中 病史者982例、恶性肿瘤者178例、肝硬化者22例。 最终纳入统计学分析的研究对象共54303例,其中 男性36777例,女性17526例。
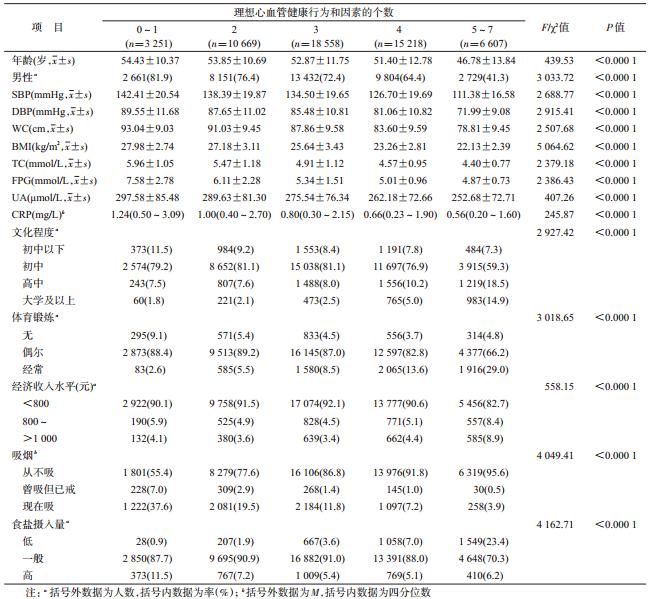
2. 不同理想心血管健康行为和因素组体检资 料:将研究对象按具有基线理想心血管健康行为和 因素的个数分为5组(由于具有0、6、7个理想心血管 健康行为和因素的人数较少,分别为241例、744例、 69例,故将0、1个合并,5~7个合并)。随着理想心 血管健康行为和因素个数的增加,年龄、男性比例、 SBP、DBP、WC、BMI、TC、FPG、尿酸(UA)、CRP水 平及吸烟比例也呈逐渐降低趋势(P<0.0001),但 文化程度、经济收入水平、体育锻炼水平呈上升趋势 (P<0.0001),见表 2。
3. 不同心血管健康行为和因素组NAFLD患病 情况:随着理想心血管健康行为和因素个数的增加, NAFLD的患病率逐渐降低,在全人群中,具有0~1、 2、3、4、5~7个理想心血管健康行为与因素组的 NAFLD的患病率分别 为62.6%、48.9%、33.3%、 16.1%和7.5%(χ2=6547.36,P<0.0001)。女 性 NAFLD患病率分别为74.9%、54.0%、36.2%、17.9% 和7.3%(χ2=2753.67,P<0.0001),男性NAFLD患 病率分别为59.9%、47.4%、32.3%、15.1%和7.7%(χ2= 3912.57,P<0.0001),见表 3。

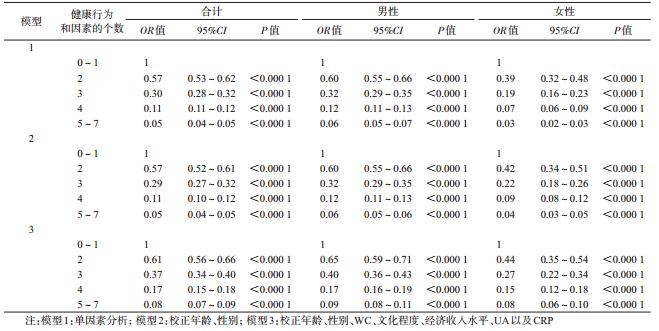
4. 理想心血管健康行为和因素与NAFLD的 logistic回归分析:以是否患NAFLD为因变量,以年 龄、性别、WC、文化程度、经济收入水平、UA、CRP以 及理想心血管健康行为和因素的个数为自变量进行 logistic回归分析。单因素分析显示,理想心血管健 康行为和因素与NAFLD有关,且随着健康行为和因 素个数的增多,OR值逐渐降低,分别为1、0.57、0.30、 0.11和0.05。校正年龄、性别因素后,理想心血管健 康行为和因素与NAFLD有关,且随着健康行为和因 素个数的增多(0~1、2、3、4、5~7),OR值逐渐降低, 分别为1、0.57、0.29、0.11和0.05。进一步校正WC、 文化程度、经济收入水平、UA以及CRP后,结果显 示,理想心血管健康行为和因素仍与NAFLD有关, 且随着健康行为和因素个数的增多(0~1、2、3、4、 5~7),OR值逐渐降低,分别为1、0.61、0.37、0.17和 0.08(表 4)。
近20年,随着肥胖和代谢综合征的广泛流行, NAFLD患病率迅速增长且呈低龄化发病趋势。本 研究显示,具有0~1、2、3、4、5~7个理想心血管健 康行为和因素组NAFLD患病率呈递减趋势,分别为 62.6%、48.9%、33.3%、16.1%和7.5%。在校正基线年 龄、性别、WC、文化程度等混杂因素后,理想心血管 健康行为和因素与NAFLD仍有关,且随着健康行为 和因素个数的增多,OR值(95%CI)逐渐降低,分别 为1、0.61(0.56~0.66)、0.37(0.34~0.40)、0.17 (0.15~0.18)和0.08(0.07~0.09)。张彩凤等[7]对开 滦研究人群随访4年的研究结果显示,具备2、3、4、 5~7个理想心血管健康行为和因素者发生高血压 的风险分别为0~1个理想心血管健康行为和因素 者的0.75、0.70、0.63和0.37倍。Wu等[8]对同一人群 的研究也发现,具备1、2、3、4、5、6~7个理想心血管 健康行为和因素者发生心脑血管事件的风险分别 为无理想心血管健康行为和因素者的0.88、0.63、 0.47、0.34、0.24和0.18倍。提示理想心血管健康行 为和因素不仅是心血管疾病的保护性因素,而且与 NAFLD密切相关。
本研究显示,随着理想心血管健康行为和因素 个数增加,SBP、DBP、WC、BMI、TC、FPG、UA、CRP 水平均呈下降趋势(P<0.0001),与已有研究结果 一致[9, 10, 11, 12]。
本研究也显示,随着理想心血管健康行为和因 素的增加,低盐饮食、不吸烟和体育锻炼者所占比例 增加,与已有研究结果一致[13, 14]。2012年Huffman 等[15]一 项 关 于 美 国 国 家 健 康 和 营 养 检 查 调 查 (National Health and Nutrition Examination Surveys, NHANES)的数据推测,到2020年全美人群心血管 健康只能改善6%,远低于AHA设定的20%的目 标。在众多NAFLD发病的危险因素中,7个理想心 血管健康行为和因素均为可干预因素,结合本研究 人群所体现的理想心血管健康行为和因素人数较少 的特点,故尚有很大的提升空间。
本研究存在局限性,第一,本研究为横断面研 究,仅能对理想心血管健康行为与因素和NAFLD的 相关性进行评估,仍需要大样本前瞻性研究进行补 充和验证。第二,研究对象仅限于开滦集团公司在 岗及离退休职工,且以男性为主,限制了结果外延。 第三,超声检查不能识别阈值(30%)以下的肝脏脂 肪浸润,可能导致本研究低估了NAFLD的发病 率。第四,由于引起NAFLD的原因很多(包括炎症 性疾病、胃肠道疾病、风湿免疫性疾病及药物等),不 能完全排除这些因素的干扰。
| [1] | Bhatia LS, Curzen NP, Calder PC, et al. Non-alcoholic fatty liver disease: a new and important cardiovascular risk factor?[J]. Eur Heart J, 2012, 33(10):1190-1200. |
| [2] | Vijay LM, Mouen K, Naga C. Non-alcoholic fatty liver disease and cardiovascular risk[J]. Curr Gastroenterol Rep, 2009, 11(1):50-55. |
| [3] | Lloyd-Jones DM, Hong YL, Labarthe D, et al. Defining and setting national goals for cardiovascular health promotion and disease reduction:the American Heart Association's strategic Impact Goal through 2020 and beyond [J]. Circulation, 2010, 121(4):586-613. |
| [4] | Jia Z, Zhou Y, Liu X, et al. Comparison of different anthropometric measures as predictors of diabetes incidence in a Chinese population[J]. Diabetes Res Clin Pract, 2011, 92(2):265-271. |
| [5] | Hu DY, Ma CS. Cardiology practice-standardized treatment(2010)[M]. Beijing:People's Health Publishing House, 2010:10-14. (in Chinese)胡大一, 马长生. 心脏病学实践2010——规范化治疗[M]. 北京:人民卫生出版社, 2010:10-14. |
| [6] | The Chinese National Workshop on Fatty Liver and Alcohol Liver Disease for the Chinese Liver Disease Association. Guidelines for management of nonalcoholic fatty liver disease: an updated and revised edition[J]. Chin J Hepatol, 2010, 18(3):163-166. (in Chinese)中华医学会肝病学分会脂肪肝和酒精性肝病学组. 非酒精性脂肪性肝病诊疗指南(2010年修订版)[J]. 中华肝脏病学杂志, 2010, 18(3):163-166. |
| [7] | Zhang CF, Shi JH, Huang Z, et al. Relationship between ideal cardiovascular behaviors and factors and the incidence of hypertension[J]. Chin J Epidemiol, 2014, 35(5):494-499. (in Chinese)张彩凤, 施继红, 黄喆, 等. 理想心血管健康行为和因素对新发高血压的影响[J]. 中华流行病学杂志, 2014, 35(5):494-499. |
| [8] | Wu S, Huang Z, Yang X, et al. Prevalence of ideal cardiovascular health and its relationship with the 4-year cardiovascular events in a northern Chinese industrial city[J]. Circ Cardiovasc Qual Outcomes, 2012, 5(4):487-493. |
| [9] | Fan JG, Saibara T, Chitturi S, et al. What are the risk factors and settings for non-alcoholic fatty liver disease in Asia-Pacific?[J]. J Gastroenterol Hepatol, 2007, 22(6):794-800. |
| [10] | Gaggini M, Morelli M, Buzzigoli E, et al. Non-alcoholic fatty liver disease (NAFLD) and its connection with insulin resistance, dyslipidemia, atherosclerosis and coronary heart disease[J]. Nutrients, 2013, 5(5):1544-1560. |
| [11] | Schwenger KJ, Allard JP. Clinical approaches to non-alcoholic fatty liver disease[J]. World J Gastroenterol, 2014, 20(7): 1712-1723. |
| [12] | Riley P, O'Donohue J, Crook M. A growing burden: the pathogenesis, investigation and management of non-alcoholic fatty liver disease[J]. J Clin Pathol, 2007, 60(12):1384-1391. |
| [13] | Keating SE, Hackett DA, George J, et al. Exercise and non- alcoholic fatty liver disease:a systematic review and meta-analysis[J]. J Hepatol, 2012, 57(1):157-166. |
| [14] | Del Ben M, Polimeni L, Baratta F, et al. Modern approach to the clinical management of non-alcoholic fatty liver disease[J]. World J Gastroenterol, 2014, 20(26):8341-8350. |
| [15] | Huffman MD, Capewell S, Ning H, et al. Cardiovascular health behavior and health factor changes(1988-2008) and projections to 2020: results from the National Health and Nutrition Examination Surveys[J]. Circulation, 2012, 125(21):2595- 2602. |