 2014, Vol. 35
2014, Vol. 35文章信息
- 寇宇, 潘劲草, 于新芬, 李钧, 杨旭辉, 文艳苹, 周银燕, 濮小英, 孙昼, 谢立. 2014.
- Kou Yu, Pan Jincao, Yu Xinfen, Li Jun, Yang Xuhui, Wen Yanping, Zhou Yinyan, Pu Xiaoying, Sun Zhou, Xie Li. 2014.
- 杭州地区2011-2013年儿童呼吸道感染人偏肺病毒分子流行病学研究
- Molecular epidemiology of human metapneumovirus in children with respiratory tract infection in Hangzhou
- 中华流行病学杂志, 2014, 35(12): 1384-1388
- Chinese Journal of Epidemiology, 2014, 35(12): 1384-1388
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2014.12.016
-
文章历史
- 投稿日期:2014-07-19




人偏肺病毒(hMPV)引起的儿童急性呼吸道感染可致毛细支气管炎和肺炎等[1]。研究显示,hMPV是杭州地区儿童急性呼吸道感染的重要病原,已有研究主要检出B1基因亚型[2],为进一步了解杭州地区儿童hMPV的流行状况及是否存在其他基因亚型,本研究对该地区儿童呼吸道门诊和住院患儿呼吸道样本进行检测。 对象与方法
1. 研究对象:哨点医院选择杭州地区就诊量大、具有代表性的医院,一家为省级儿童医院,另一家为设有儿科的综合性医院,均为国家流感哨点医院。选取2011年1月至2013年12月<14岁的呼吸道儿科门诊流感样病例(ILI)及住院的严重急性呼吸道感染病例(SARI)为研究对象[3, 4]。收集门诊ILI患儿的咽拭子样本,住院病例收集当日白天新入院诊断为SARI的痰液抽取物(或气管吸取物),并于24 h内送至实验室。样本采集过程均告知患儿家属并征得同意。
2. 研究方法:
(1)hMPV及其他病毒检测:样本病毒RNA提取使用德国Qiagen公司的RNeasy Mini试剂盒,按试剂盒说明书操作。用宝生物工程(大连)有限公司的TaKaRa反转录试剂盒,以随机六聚体引物反转录合成cDNA,-40 ℃保存。采用实时荧光 RT-PCR检测hMPV,检测方法、引物、探针参见文献[5],PCR反应20 μl体系中加入1 μl cDNA为模板,使用TaKaRa Ex Taq酶进行扩增。扩增条件:94 ℃ 3 min;94 ℃ 30 s,55 ℃ 30 s,72 ℃ 30 s,45个循环。传统RT-PCR检测hMPV,参考文献[6]合成hMPV F蛋白基因片段的引物,引物序列:hMPV F-F:5′-GAA AAT CCC AGA CAA TC-3′,hMPV F-R:5′-CCA TGT AAA TTA CGG AGC-3′,扩增条件: 94 ℃ 5 min;94 ℃ 30 s,55 ℃ 30 s,72 ℃ 1 min,36个循环;72 ℃ 7 min。目的片段526 bp(荧光定量RT-PCR检测荧光信号较强、Ct值较小的样本)。扩增产物测序结果与GenBank已知hMPV F蛋白进行比对。用实时荧光RT-PCR方法检测呼吸道合胞病毒(RSV)、流感病毒(INF,包括甲型和乙型),方法参见文献[7, 8]。
(2)hMPV基因分型及序列分析:测序由上海生工生物工程有限公司完成。所测序列用NCBI-BLAST和DNAStar软件进行同源性比较。基因分型采用基因测序分型方法,使用Mega 5.0软件,采用邻接法(NJ)构建进化树,参照各亚型标准株序列,毒株亚型以其F基因片段序列在进化树分支中的位置确认。序列比较和进化树分析所用4种不同亚型参考序列均来源NCBI的GenBank注册hMPV病毒株,参考序列号:A1亚型为NL00-1(AF371337);A2a亚型包括CAN97-83(AY297749)、NL00-17(AY298021);A2b亚型包括BJ1887(DQ843659)、JPS03-240(AY530095);B1亚型为NL99-1(AY525842);B2亚型包括CAN98-75 (AY297748)、BJ1887(DQ843659)。同时将杭州地区hMPV F蛋白核苷酸序列提交GenBank注册。
3. 统计学分析:用SPSS 16.0 软件进行数据整理分析、描述性统计和样本率的χ2检验,组间比较采用χ2分割检验。 结果
1. 一般情况:共纳入2 593例病例,其中儿科门诊1 676例、住院917例。hMPV检出率为6.51%(169/2 593),男性患儿检出率(7.01%,112/1 597)与女性患儿检出率(5.72%,57/996)差异无统计学意义(χ2=1.046,P=0.306)。
2. hMPV检出率:
(1)不同年龄组比较:hMPV检出患儿年龄为1月龄至10岁。以2岁组和3岁组检出率最高,分别为14.14%(28/196)、14.01%(22/157)。卡方分割分析显示,2岁组与3岁组检出率差异无统计学意义(χ2=0.001,P=0.972),与其他各组检出率差异有统计学意义(χ2=38.654,P=0.000)。
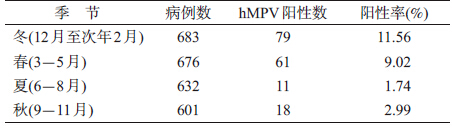
(2)不同时间比较:2011年hMPV检出率为6.50%(60/923)、2012年为6.11%(56/916)、2013年为7.02%(53/754),3年检出率差异无统计学意义(χ2=0.570,P=0.752)。hMPV检出有明显的季节性,检出率最高的是2013年3月(21.12%,15/71),各年7-9月检出率较低或未被检出,见图 1。按季节分布,冬季(11.56%)>春季(9.02%)>秋季(2.99%)>夏季(1.74%),见表 1。卡方分割分析显示,夏季与秋季检出率差异无统计学意义(χ2=2.111,P=0.146),冬季与春季检出率差异无统计学意义(χ2=2.378,P=0.123),冬春季与夏秋季差异有统计学意义(χ2=67.032,P=0.000)。
 |
| 图 1 2011-2013 年杭州地区门诊和住院儿童病例hMPV检出率 |
(3)门诊与住院病例比较:门诊ILI样本hMPV检出率为6.62%(111/1 676),住院SARI样本hMPV检出率为6.32%(58/917),差异无统计学意义(χ2=0.085,P=0.769)。连续监测显示,住院病例hMPV流行高峰滞后门诊病例1~2个月(图 1)。门诊样本hMPV冬季检出率最高,为13.56%(59/453),其次是春季,为8.08%(35/433);住院样本春季检出率最高,为9.34%(20/248),其次是冬季,为8.06%(26/243)。门诊与住院冬季两样本检出率差异有统计学意义(χ2=4.669,P=0.031);春季两样本检出率差异无统计学意义(χ2=1.298,P=0.255)。
3. hMPV基因进化树、序列分析:hMPV检测阳性样本核酸扩增产物测序率为52.07%(88/169)。利用杭州地区88株F基因526 bp基因核苷酸序列构建系统进化树,结果显示,杭州地区hMPV株的遗传谱系分为A、B 两个簇,各簇又分为A1、A2和B1、B2亚簇,其中A1亚簇仅包含1个分支(图 2)。进化树显示,2011-2012年杭州地区以B1基因为优势亚型,2012年底至2013年以A2为主要优势亚型,见图 3。
 |
| 图 2 2011-2013 年杭州地区hMPV 基因型系统进化树 |
 |
| 图 3 2011-2013年杭州地区hMPV基因型分布 |
同源性分析显示,测序的88株阳性基因序列与GenBank参考株序列同源性为81.60%~100.00%。各基因型与代表株核苷酸同源性较高,杭州地区A1基因型仅1例,与代表株NL00-1(AF371337)核苷酸同源性为 99.95%;A2基因型与代表株CAN97-83(AY297749)核苷酸同源性为96.00%~100.00%。B1基因型与代表株NL99-1(AY525843)核苷酸同源性为97.70%~100.00%;B2基因型与代表株CAN98-75(AY297748)核苷酸同源性为94.50%~100.00%。杭州地区的88株hMPV测序结果中12份F蛋白部分基因序列已收录GenBank,登录号为KF729939~KF729950。
4. hMPV不同基因型的年龄分布:A基因<1岁组占优势(53.19%,25/47),其次是1~2岁组(27.65%,13/47);B基因型1~2岁组最多(46.34%,19/41),其次<1岁组(31.70%,13/41),见表 2 。<1岁和≥1岁A、B基因型检出率差异有统计学意义(χ2=5.143,P=0.023)。

5. hMPV与RSV、INF混合感染情况:2 593份样本的3种病毒混合感染检出率为1.50%(39/2 593),hMPV与RSV或INF感染占23.07%(39/169)。39份混合感染样本中,hMPV与RSV阳性占48.71%(19/39),hMPV与INF阳性占30.76%(12/39),hMPV、RSV、INF同时阳性占5.12%(2/39),RSV与INF混合感染占15.38%(6/39)。 讨论
本研究显示,2011-2013年杭州地区患儿呼吸道感染hMPV检出率为6.51%,其中住院SARI样本检出率为6.32%(58/917),门诊ILI样本检出率为6.62%(111/1 676),门诊ILI与住院SARI样本hMPV检出率差异无统计学意义。与该地区之前的门诊检出率(6.27%)一致[9]。
本研究还显示,杭州地区患儿<1岁组hMPV检出率最低,1~3岁组较高,4~6岁组检出率逐渐降低,与Daniel等[10]研究一致。
本研究也显示,杭州地区hMPV每年流行高峰不一致,全年各季节均有hMPV检出,但统计学结果显示,冬春季与夏秋季hMPV检出率差异有统计学意义。杭州冬季检出率为11.56%,与本项目的前期研究(2009-2010、2010-2011冬季)检测结果(11.23%)一致[2]。杭州住院患儿hMPV高峰在冬末初春,与南京地区报道一致[11],可能与所处地域及环境气候有关。
有研究认为,A型hMPV的致病性高于B型[12],另报道则认为2种型别的致病性没有差别[13]。本研究显示,门诊、住院hMPV A基因型阳性样本差异无统计学意义。
hMPV基因型随年代发生不同变化:北京地区2008年7月至2009年3月以hMPV A2最流行,2009年4月至2010年3月以B1为主,其次是B2亚型[14]。杭州地区在2009-2010年冬季为B1亚型流行[2],与上述报道相同,2010-2011年冬季以B1为主。2011-2012年冬季以B1和A2为主,2012-1013年冬季以A2为主。基因进化分型分析,杭州地区hMPV毒株之间的亲缘关系较近,而与同型别内的参考株亲缘关系稍远,如A2b亚型杭州株与同亚型北京株(BJ1887)同属一个基因亚型,在不同的分支,提示杭州地区hMPV有地区特异性。
| [1] Chan PK,Tam JS,Lam CW,et al. Human metapneumovirus detection in patients with severe acute respiratory syndrome[J]. Emerg Infect Dis,2003,9(9):1058-1063. |
| [2] Kou Y,Yu XF, Pan JC, et al. Analysis of infection status and pathogenic features of human metapneumovirus among children in Hangzhou between year 2009 and 2011[J]. Chin J Prev Med,2013,47(1):31-34. (in Chinese)寇宇,于新芬,潘劲草,等. 2009-2011年杭州地区儿童人类偏肺病毒感染状况及病原特征分析[J]. 中华预防医学杂志,2013,47(1):31-34. |
| [3] The Ministry of Health of the People's Republic of China. National Programme of Influenza Surveilance (2010)[EB/OL]. [2010-09-03]. http://www.moh.gov.cn/jkj/s3577/201009/3fa356d0f4834d408f de6c12891a6482.shtml. (in Chinese)中华人民共和国卫生部. 全国流感监测方案(2010版) [EB/OL].[2010-09-03]. http://www.moh.gov.cn/jkj/s3577/201009/3fa356d0f4834d408fde6c12891a6482.shtml. |
| [4] The Ministry of Health of the People's Republic of China. Sentinel Surveilance Programme on Inpatients with Severe Acute Respiratory Tract Infection (2011)[EB/OL].[2011-01-28]. http://www.gov.cn/zwgk/2011-02/11/content_1801649.html.(in Chinese)中华人民共和国卫生部. 住院严重急性呼吸道感染病例哨点监测方案(2011年版)[EB/OL]. [2011-01-28]. http://www.gov.cn/zwgk/2011-02/ 11/content_1801649.html. |
| [5] Dare R, Sanghavi S, Bullotta A, et al. Diagnosis of human metapneumovirus infection in immunosupprssed lung transplant recipients and children evaluated for pertussis[J]. J Clin Microbiol,2007,45(2):548-552. |
| [6] Pabbaraju K,Wong S, McMillan T, et al. Diagnosis and epidemiological studies of human metapneumovirus using real-time PCR[J]. J Clin Virol,2007,40(3):186-192. |
| [7] Yu XF,Pan JC,Ye R, et al. Preparation of armored RNA as a control for multiplex real-time reverse transcription-PCR detection of influenza and severe acute respiratory syndrome coronavirus[J]. J Clin Microbiol,2008,46(3):837-841. |
| [8] van de Pol AC, van Loon AM, Wolfs TF, et al. Increased detection of respiratory syncytial virus,influenza viruses,parainfluenza viruses,and adenoviruses with real-time PCR in samples from patients with respiratory symptoms[J]. J Clin Microbiol,2007,45(7):2260-2262. |
| [9] Yang XH,Kou Y,Li J,et al. Human metapneumovirus infection in children with influenza-like illness Hangzhou[J]. Chin J Clin Infect Dis,2014,7(3):222-225. (in Chinese)杨旭辉,寇宇,李钧,等. 杭州地区儿童流感样病例人偏肺病毒流行情况分析[J]. 中华临床感染病杂志,2014,7(3):222-225. |
| [10] Daniel DE, Alpuche-Solís AG, Herrera-Díaz A,et al. Human meta-pneumovirus infections in Mexico:epidemiological and clinical characteristics[J]. J Med Microbiol,2005,54(10):969- 974. |
| [11] Jin Y, Zhang J, Zhao DY, et al. Molecular epideiological and clinical feature of human metapneumovirus in children with acute respiratory tract infection in Nanjing city[J]. Chin J Exp Clin Virol,2011,25(1):11-13. (in Chinese)金玉,张静,赵德育,等. 南京地区儿童人偏肺病毒感染的流行病学及临床特征分析[J]. 中华实验和临床病毒学杂志,2011,25(1):11-13. |
| [12] Vicente D,Mantes M,Cilia C,et al. Differencos in clinical verity between genotype A and genotype B human metapneumovirus infection in children[J]. Clin Infect Dis,2006,42(12):111-113. |
| [13] Wei HY,Tsao KC,Huang CG,et al. Clinical features of different genotypes/genogroups of human metapneumovirus in hospitalized children[J]. J Microbiol Immunol Infec,2013,46(5):352-357. |
| [14] Li J,Wang Z, Gonzalez R, et al. Prevalence of human metapneumovirus in adults with acute respiratory tract infection in Beijing,China[J]. J Infection,2012,64(1):96-103. |