 2014, Vol. 35
2014, Vol. 35文章信息
- 杨娟, 冯录召, 郑亚明, 余宏杰. 2014.
- Yang Juan, Feng Luzhao, Zheng Yaming, Yu Hongjie. 2014.
- 中国2012年疾病相关过早死亡的间接经济负担估计
- Estimation on the indirect economic burden of disease-related premature deaths in China, 2012
- 中华流行病学杂志, 2014, 35(11): 1256-1262
- Chinese Journal of Epidemiology, 2014, 35(11): 1256-1262
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2014.11.018
-
文章历史
- 投稿日期:2014-8-5




疾病经济负担指疾病、伤残和过早死亡(早亡) 对患者、家庭与整个社会带来的经济损失,主要包括 直接经济负担和间接经济负担。直接经济负担指患 者就医所支付的医疗费和交通费等[1];间接经济负 担包括疾病导致短期或长期失能带来的生产力损 失、早亡所导致的未来收入减少的现值、家属因陪护患者而误工所引起的经济损失等[2]。国外研究显 示,早亡所致生产力损失占疾病经济负担的21%~ 81%[3, 4, 5, 6, 7]。我国疾病经济负担研究主要关注直接经 济负担、疾病造成失能以及家属陪护所致间接经济 负担[8, 9, 10, 11, 12, 13]。尽管已有研究探索早亡所致间接经济负 担,但仅局限于个别危险因素和疾病(如吸烟和糖尿 病),且均采用人力资本法(human capital approach) 进行测算[14, 15, 16, 17]。估计间接经济负担通常采用人力资 本法。然而,该方法可能存在明显高估[18, 19, 20, 21]。目前 越来越多研究采用摩擦成本法(friction cost method)[18, 22]。为此本研究分别采用上述两种方法 测算我国不同疾病相关早亡所致间接经济负担,为 全面、宏观评估疾病负担提供重要信息。 资料与方法
1. 人力资本法:该法认为患者因早亡损失生命 年,s 岁个体早亡的间接经济负担等于活到s 岁的个 体在期望生存年限的总收入现值(present value of lifetime earnings,PVLE)[23]。计算公式

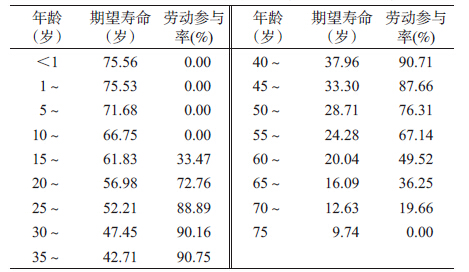
式(1)中各参数取值及其来源:①我国各年 龄段期望寿命(以5 年为间隔)来自WHO 寿命表 (表 1)[24],本文采用线性插入法得到各年龄(以1 年 为间隔)的期望寿命。②劳动参与率是指经济活动 人口占劳动年龄人口的比例[25],年龄别劳动参与率 数据来自我国2010 年人口普查结果[26]。我国经济 活动人口是指年龄≥16 岁在一定时期内为各种经 济生产和服务活动提供劳动力供给的人口。因此 本研究将<16 岁人群的劳动参与率设定为0,且≥ 75 岁老年人群不再参与经济活动(表 2)。③2012 年 我国城乡居民人均年收入分别为26 959 元和10 991 元[27],本文以城乡人口数为权重(城镇71 182 万 人;农村64 222 万人)计算得到我国人均年收入为 19 385 元。④基线分析时,本研究采用3%贴现率将 未来收入转换为2012 年现值[28]。
2. 摩擦成本法:该法认为雇员因病离职其工作 可由新雇员接替,故仅在前任雇员死亡至新雇员入 职期间(即摩擦期)存在经济损失,即a 岁个体早亡 的间接经济负担等于摩擦期内为恢复该岗位生产的 全部费用,包括生产力损失、招聘和培训新员工的成本[18, 22]。计算公式

式(2)中各参数取值及其来源:①劳动参与率和 年人均收入取值与式(1)相同。②摩擦期受整个社 会的失业率水平、劳动市场对劳动力需求和供应方 面的配置效率、雇员因病离开工作岗位至决定聘用 新雇员间的时间间隔等因素有关。由于本研究缺乏 相关数据,在基线分析时采用荷兰的研究结果(摩擦 期=3 个月)[18]。③本研究劳动力弹性设定为0.8,即 雇员误工1 个月将导致当月生产力损失80%,其余 20%将通过内部劳动力(如其他员工暂时顶替)等方 式得到弥补[21]。④前期研究显示,2009 年招聘和培 训新员工成本为2 441 元[29]。目前我国男女性法定 退休年龄分别为60 岁和55 岁,因而未考虑招聘和培 训>60 岁老年人的成本。⑤本研究所有成本均通 过居民消费价格指数调整至2012 年的价值[27]。
3. 疾病相关早亡的间接经济负担估计:采用人 力资本法计算疾病相关早亡的间接经济负担公式

4. 敏感性分析:本研究对不确定性参数进行敏 感性分析,以评估其对疾病相关早亡的间接经济负 担估计值的影响。不确定性参数包括①评估贴现率 为≤6%时,人力资本法估计值较基线值的变动情 况。②评估摩擦期为1~6 个月和劳动力弹性为 0.6~1.0 时,摩擦成本法估计值较基线值的变动情 况。③考虑到死因监测数据的漏报问题,本研究敏 感性分析采用8.59%~26.23%的漏报率评估死亡漏 报对结果的影响[31, 32, 33, 34, 35]。 结果
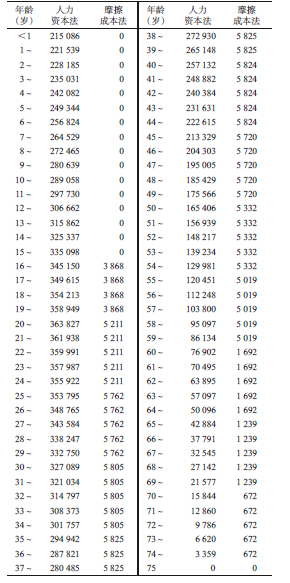
1. 早亡个体的生产力损失:人力资本法和摩擦 成本法测算得到的早亡个体生产力损失平均为 213 096 元/人和3 368 元/人。表 2 显示两种方法测 算得到的个体在不同年龄死亡所造成的生产力损失情况。后者估计值远远低于前者,几乎均不足前者 的5%。
2. 疾病相关早亡的间接经济负担:采用人力资 本法估计,2012 年我国早亡所致间接经济负担为 4 251 亿元,约占同期GDP(518 942 亿元)8‰[27]。其 中慢病相关早亡的间接经济负担所占比例最高 (67.1%,2 954 亿元),其次为伤害(25.6%,1 089 亿 元);传染病、母婴疾病和营养缺乏性疾病最低 (6.4 %,269亿元)。前五位早亡所致间接经济负担顺 位依次为恶性肿瘤(1 208 亿元)、心血管疾病(1 060 亿元)、意外伤害(916 亿元)、故意伤害(158 亿元)和 呼吸系统疾病(147 亿元),在全死因相关早亡所致 间接经济负担中所占比例均超过20%(表 3)。
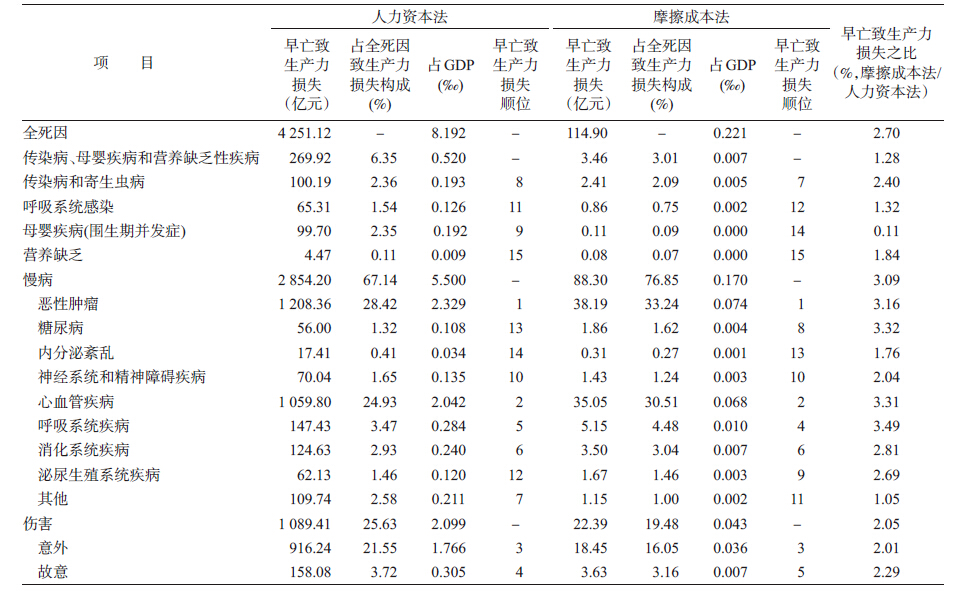
与人力资本法估计结果相比,采用摩擦成本法 估计的2012 年我国早亡所致间接经济负担仅为其 2.7%(115 亿元,占同期GDP 0.2‰);各类疾病相关 早亡所致间接经济负担约为其0.11%~3.49%;早亡 所致间接经济负担顺位基本一致(表 3)。
采用人力资本法估计的结果显示,与在低龄儿 童和老人年中较高死亡率情况不同,在40~59 岁人 群中全死因和慢病相关早亡所致间接经济负担均最 高;20~49 岁人群中以伤害最高;而<5 岁人群则传 染病、母婴疾病和营养缺乏性疾病最高。采用摩擦成 本法估计的结果与之略有差异,即不同疾病相关早亡 所致间接经济负担均为40~59岁人群最高(图 1)。
 |
| 图 1 我国居民疾病年龄别死亡率及早亡所致间接经济负担 |
3. 敏感性分析:与基线结果相比,当贴现率为0 和6%时,采用人力资本法估计的全死因相关早亡所 致间接经济负担分别上升33%(6 363 亿元)、下降 24%(3 224 亿元);不同类别疾病相关早亡所致间接 经济负担分别上升22%~58%、下降17%~60%。当 劳动弹性率在60%和100%间变动时,采用摩擦成本 法估计得到的早亡所致间接经济负担变化不大(分 别下降和上升13%~18%)。当摩擦期为1 个月和6 个月时,采用摩擦成本法估计得到的早亡所致间接 经济负担较基线值分别下降34% ~48% 、上升 52%~72%(图 2)。当分别采用8.59%~26.23%的漏 报率对死亡率进行校正时,两种方法的估计值相应 较基线值升高8.59%~26.23%。人力资本法估计全 死因相关早亡所致间接经济负担达到4 616 亿元至 5 366 亿元;摩擦成本法估计值为125亿元至145亿元。
 |
| 图 2 我国居民早亡相关死亡所致间接经济负担的敏感性分析 |
早亡所致间接经济负担是疾病经济负担的重要 组成部分。本研究发现,2012 年我国全死因相关早亡导致间接经济损失为4 251 亿元(人力资本法)和 115 亿元(摩擦成本法),占同期GDP 8‰和0.2‰。 2012 年我国疾病直接医疗费用约25 023 亿元(疾病 直接医疗费用=门诊人均医药费×门诊人次数+住 院人均医药费×出院人数[36])。早亡所致间接经济 负担约为疾病直接医疗费用的17%(人力资本法)和0.5%(摩擦成本法)。因未获得疾病相关直接非医疗 成本和伤残所致间接经济负担等数据,本研究尚不 能估计早亡所致间接经济负担在全部疾病经济负担 中所占比重。
本研究人力资本法估计得到的早亡个体生产力 损失平均为213 096 元/人,为Menzin 等[19]估计值的 2 倍。后者估计值较低主要与其采用的贴现率 (14.3%)很高有关。如敏感性分析结果显示,贴现率 对结果影响较大,贴现率越高,估计值越低。根据 WHO关于卫生经济学评价指南建议[28],本研究采用 3%(0~6%)贴现率将未来收入转换为2012 年现值。
本研究结果显示,摩擦成本法估计结果明显低 于人力资本法估计值,仅为后者的0.11%~3.49%。 Goeree 等[22]对精神分裂症所致早亡的间接经济负担评估也发现,人力资本法估计值是摩擦成本法的69 倍。人力资本法认为早亡所致间接经济负担等于患 者于当前年龄至75 岁间通过劳动创造的价值。而 摩擦成本法认为早亡所致间接经济负担只发生在摩 擦期(即前任雇员死亡至新雇员入职期间)。人力资 本法所采用的时间段远远大于摩擦成本法中的摩擦 期。这是导致两种方法估计值存在较大差异的主要 原因。目前关于间接经济负担估计方法的选择仍然 存在较大争议。反对人力资本法的学者认为,长期 误工可由重新雇佣员工得到解决,因而该方法可能 显著高估实际情况[18]。而反对摩擦成本法的学者指 出,该方法认为超过摩擦时间的劳动价值为零,这不 符合新古典经济学理论的基本假设[37]。由于使用何 种方法更优尚无定论,因而本研究同时使用两种方 法进行估计,相应结果可作为早亡所致间接经济负 担的最低和最高估计值,为评估疾病经济负担提供 参考信息。
两种估计方法结果均显示,慢病所致间接经济 负担所占比例最高,其次为伤害,传染病、母婴疾病 和营养缺乏性疾病所致间接经济负担相对较小。前 五位早亡所致间接经济负担顺位依次为恶性肿瘤、 心血管病、意外伤害、故意伤害和呼吸系统疾病。无 论从疾病对人群健康的影响方面[38],还是从疾病对 社会经济影响角度分析,慢病均是我国目前主要疾 病负担,伤害所致疾病负担也不容忽视。
制定防控策略主要从疾病对人群健康影响的角 度,着重针对发病和死亡风险高的人群(如儿童免疫 接种、中老年人肺癌筛查)。本研究发现,尽管死亡 率随年龄增加不断上升,但早亡所造成的间接经济 负担主要集中在20~59 岁人群。另外,尽管呼吸系 统感染死亡率高(死亡顺位居第五位),但因主要导 致<5 岁以下儿童和>60 岁老年人死亡,其对生产 力的影响很小(相关早亡所致间接经济负担顺位居 第11 或12 位)。因此,在制定疾病防控策略、分配卫 生资源时,不能忽略疾病经济负担影响,在关注高危 人群的同时,应兼顾发病和死亡风险相对较低但疾 病经济负担较重的劳动年龄人群。
敏感性分析显示,由于部分参数的不确定性,本 研究估计值存在一定程度的不稳定性。无论采用哪 种测算方法,死因监测数据的漏报对早亡所致间接 经济负担估计结果的影响不容忽视。漏报率越高, 基于现有报告数据的间接经济负担估计值越明显被 低估。监测数据质量是确保早亡所致间接经济负担 估计值准确性的基础。部分省市对死因监测数据质量进行了评估[31, 32, 33, 34, 35],然而却无公开发表的全国性漏 报评估结果,使得本研究无法对死亡率进行准确校 正。对人力资本法而言,间接经济负担估计值对贴 现率较敏感。本研究基线分析时采用WHO推荐的 3%贴现率[28],以便与其他研究结果具有可比性。对 摩擦成本法而言,摩擦期对摩擦成本法估计值影响 较大。摩擦期越长,早亡所致间接经济负担估计值 越大。由于我国尚无对摩擦期的相关研究,本文采 用荷兰数据(3 个月)进行基线分析。因我国劳动力 市场与荷兰存在差异,相应摩擦成本法估计值需后 续研究进一步验证。
除参数不确定性外,本研究还存在一些不足。 对人力资本法而言,未考虑家务劳动价值,如家庭主 妇看护孩子的经济价值。另外,本研究假设>75 岁 老人不再参与经济活动,而事实上还有部分老年人仍 从事一些经济活动(如务农),尤其在经济欠发达地 区,这些均可导致低估早亡所致间接经济负担。对摩 擦成本法测算结果而言,招聘和培训新员工成本在总 间接经济负担中所占比例很大(42%~63%)。然而, 因缺乏大规模研究,该数据来自一家三甲医院的调 查[29],很难代表全国所有行业的实际情况。
综上所述,本研究同时采用人力资本法和摩擦 成本法估计我国疾病相关早亡所致间接经济负担, 其结果为进一步全面、系统评估疾病总经济负担(包 括直接医疗成本、直接非医疗成本、伤残所致间接成 本和早亡所致间接成本)提供了重要数据。
| [1] World Health Organization. WHO guide to identifying the economic consequences of disease and injury [DB/OL]. [2014-07-17]. http://www.who. int/choice/publications/d_economic_impact_ guide.pdf. |
| [2] Hu JP,Rao KQ,Qian JC,et al. Macroscopic analysis on economic burden of diseases in China [J]. Chin Health Eco,2007,26(6):56-58. (in Chinese) 胡建平,饶克勤,钱军程,等. 中国疾病经济负担的宏观分析 [J]. 中国卫生经济杂志,2007,26(6):56-58. |
| [3] Ko SK,Yoon SJ, Oh IH, et al. The economic burden of inflammatory heart disease in Korea [J]. Korean Circ J,2011,41(12):712-717. |
| [4] Lightwood J,Bibbins-Domingo K,Coxson P, et al. Forecasting the future economic burden of current adolescent overweight:an estimate of the coronary heart disease policy model [J]. Am J Public Health,2009,99(12):2230-2237. |
| [5] Molinari NA,Ortega-Sanchez IR, Messonnier ML,et al. The annual impact of seasonal influenza in the US:measuring disease burden and costs [J]. Vaccine,2007,25(27):5086-5096. |
| [6] Luengo-Fernandez R, Leal J,Gray A,et al. Cost of cardiovascular diseases in the United Kingdom [J]. Heart,2006,92(10):1384-1389. |
| [7] Leal J,Luengo-Fernández R,Gray A,et al. Economic burden of cardiovascular diseases in the enlarged European Union [J]. Eur Heart J,2006,27(13):1610-1619. |
| [8] Wang D,Zhang T,Wu J,et al. Socio-economic burden of influenza among children younger than 5 years in the outpatient setting in Suzhou,China [J]. PLoS One,2013, 8(8):e69035. |
| [9] Zhou L,Situ S,Huang T,et al. Direct medical cost of influenza-related hospitalizations among severe acute respiratory infections cases in three provinces in China[J]. PLoS One,2013,8(5):e63788. |
| [10] Lu J,Xu A,Wang J,et al. Direct economic burden of hepatitis B virus related diseases:evidence from Shandong,China [J]. BMC Health Serv Res,2013,13(1):37. |
| [11] Chen J, Li YT, Gu BK, et al. Estimation of the direct cost of treating people aged more than 60 years infected by influenza virus in Shanghai[J]. Asia Pac J Public Health,2012.[Epub ahead of print] |
| [12] Ye F,Wang H,Huntington D,et al. The immediate economic impact of maternal deaths on rural Chinese households[J]. PLoS One,2012,7(6):e38467. |
| [13] Hu M,Chen W. Assessment of total economic burden of chronic Hepatitis B (CHB)-related diseases in Beijing and Guangzhou,China[J]. Value Health,2009,12 Suppl 3: S89-92. |
| [14] Sung HY,Wang L,Jin S,et al. Economic burden of smoking in China,2000 [J]. Tob Control,2006,15 Suppl 1:i5-11. |
| [15] Yang L,Sung HY,Mao Z,et al. Economic costs attributable to smoking in China:update and an 8-year comparison,2000-2008 [J]. Tob Control,2011,20(4):266-272. |
| [16] Le C,Lin L,Jun D,et al. The economic burden of type 2 diabetes mellitus in rural southwest China [J]. Int J Cardiol,2013,165(2):273-277. |
| [17] Lou P,Zhu Y,Chen P,et al. Vulnerability,beliefs,treatments and economic burden of chronic obstructive pulmonary disease in rural areas in China:a cross-sectional study [J]. BMC Public Health,2012,12:287. |
| [18] Koopmanschap MA,Rutten FF,van Ineveld BM,et al. The friction cost method for measuring indirect costs of disease[J]. J Health Econ,1995,14(2):171-189. |
| [19] Menzin J,Marton JP,Menzin JA, et al. Lost productivity due to premature mortality in developed and emerging countries:an application to smoking cessation[J]. BMC Med Res Methodol,2012,12:87. |
| [20] Drummond M. Cost-of-illness studies[J]. Pharmacoeconomics,1992,2(1):1-4. |
| [21] Hutubessy RC,van Tulder MW,Vondeling H,et al. Indirect costs of back pain in the Netherlands:a comparison of the human capital method with the friction cost method [ J]. Pain,1999,80(1):201-207. |
| [22] Goeree R, O'Brien BJ, Blackhouse G, et al. The valuation of productivity costs due to premature mortality:a comparison of the human-capital and friction-cost methods for schizophrenia [J]. Can J Psychiatry,1999,44(5):455-463. |
| [23] Xu DB,Ma AX,Li HC. Approaches of estimating disease burden [J]. Chin Lic Phar,2010,7(11):28-31. (in Chinese) 徐东波,马爱霞,李洪超. 疾病成本的测算方法研究[J]. 中国执业药师杂志,2010,7(11):28-31. |
| [24] World Health Organization. Life tables for 2011,2000 and 1990 [DB/OL]. [2013-08-28]. http://apps.who.int/gho/data/view.main.60340. |
| [25] International Labour Organization (ILO). Main statistics(annual) economically active population [EB/OL]. [2013-08-28]. http://laborsta.ilo.org/applv8/data/c1e.html. |
| [26] Population Census Office under the State Council & Department of Population and Employment Statistics National Bureau of Statistics of China.Tabulation on the 2010 population census of the People's Republic of China [R/OL]. [2014-05-03]. http://www.stats.gov.cn/tjsj/pcsj/rkpc/6rp/indexch.htm. (in Chinese) 国务院人口普查办公室国家统计局人口和就业统计司. 中国2010年人口普查资料[R/OL]. [2014-05-03]. http://www.stats.gov.cn/tjsj/pcsj/rkpc/6rp/indexch.htm. |
| [27] National Bureau of Statistics of China. China Statistical Yearbook 2013[R/OL]. [2014-07-03]. http://www.stats.gov.cn/tjsj/ndsj/2013/indexch.htm. (in Chinese) 中华人民共和国国家统计局. 中国统计年鉴2013 [R/OL]. [2014-07-03]. http://www.stats.gov.cn/tjsj/ndsj/2013/indexch.htm. |
| [28] World Health Organization. Making choices in health:WHO guide to cost-effectiveness analysis [EB/OL]. [2014-07-03]. http://www.who.int/choice/book/en/. |
| [29] Zhu JL,Mao XM. Research on calculation and analysis of recruitment cost in a tertiary hospital [J]. Chin Hosp,2012,16(12):63-65. (in Chinese) 朱俊利,毛晓旻. 某三甲医院人力资源招聘成本测算与分析 [J]. 中国医院,2012,16(12):63-65. |
| [30] Chinese Center for Disease Control and Prevention. Disease surveillance dataset 2012 of national disease surveillance system [M]. Beijing:Popular Science Press, 2013:248-252. (in Chinese) 中国疾病预防控制中心. 全国疾病监测系统死因监测数据集2012[M]. 北京:科学普及出版社,2013:248-252. |
| [31] Li XQ,Zhong WL, Lin SG. Investigation on the death under-reporting in disease monitoring system from 2006 to 2008 in Fujian [J]. Mod Prev Med,2011,38(18): 3778-3781.(in Chinese) 李晓庆,钟文玲,林曙光. 福建省疾病监测系统2006-2008年死因监测漏报调查 [J]. 现代预防医学,2011,38(18):3778-3781. |
| [32] Pan JJ,Zhang L,Zhang QJ,et al. Underreporting of death in disease surveillance system in Hubei,2009-2011 [J]. Dis Surveill,2013,28(6):478-480. (in Chinese) 潘敬菊,张岚,张庆军,等. 2009-2011年湖北省疾病监测点死因漏报调查分析[J]. 疾病监测,2013,28(6):478-480. |
| [33] Sha QY,Zhang S,Ma FC,et al. The causes of death in Qinghai province[J]. Chin Prev Med,2010,11(9):911-914. (in Chinese) 沙琼玥,张晟,马福昌,等. 2006-2009年青海省疾病监测点死因监测情况分析 [J]. 中国预防医学杂志,2010,11(9):911-914. |
| [34] Xu XJ,Xu YJ,Cai QM,et al. Death cause underreporting through disease surveillance system in Guangdong,2009-2011[J]. Dis Surveill,2013,28(7):570-574. (in Chinese) 许晓君,许燕君,蔡秋茂,等. 2009-2011年广东省疾病监测系统死因漏报调查分析[J]. 疾病监测,2013,28(7):570-574. |
| [35] Xuan SL,Di XJ,Li SF. Analysis of under-reporting of mortality surveillance from 2006-2008 in Henan [J]. Mod Prev Med,2014,41(7):1321-1325. (in Chinese) 轩水丽,底秀娟,李少芳. 河南省2006-2008年死因监测系统漏报调查分析 [J]. 现代预防医学,2014,41(7):1321-1325. |
| [36] National Health and Family Planning Commission of the People's Republic of China.Health Statistics Yearbook 2013[R/OL]. [2014-07-08]. http://www.nhfpc.gov.cn/htmlfiles/zwgkzt/ptjnj/year2013/index2013.html. (in Chinese) 中华人民共和国国家卫生和计划生育委员会. 2013中国卫生统计年鉴[R/OL]. [2014-07-08]. http://www.nhfpc.gov.cn/htmlfiles/zwgkzt/ptjnj/year2013/index2013.html. |
| [37] Johannesson M,Karlsson G. The friction cost method:a comment [J]. J Health Econ,1997,16(2):249-255. |
| [38] Press Office of Ministry of Heatlh in China. Major results of the third national survey of death causes[J]. Chin Cancer,2008(5):344-345. (in Chinese) 卫生部新闻办公室. 第三次全国死因调查主要情况 [J]. 中国肿瘤,2008(5):344-345. |