 2014, Vol. 35
2014, Vol. 35文章信息
- 周静雯, 吴佳慧, 梁柱, 佟斯琴, 佟伟军, 张永红, 张绍艳. 2014.
- Zhou Jingwen, Wu Jiahui, Liang Zhu, Tong Siqin, Tong Weijun, Zhang Yonghong, Zhang Shaoyan. 2014.
- 内蒙古部分地区蒙古族空腹血糖受损人群10年转归及影响因素分析
- Outcomes and correlated factors in patients with impaired fasting glucose: a ten-year follow-up analysis
- 中华流行病学杂志, 2014, 35(11): 1241-1243
- Chinese Journal of Epidemiology, 2014, 35(11): 1241-1243
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2014.11.014
-
文章历史
- 投稿日期:2014-5-19




2 内蒙古通辽市奈曼旗固日班花苏木卫生院
2 Health Center of Guribanhua Township, Naiman, Tongliao, Inner Mongolia
根据美国糖尿病协会(ADA)的标准,IFG 即 血糖为5.6 mmol/L(100 mg/dl)至6.9 mmol/L (125 mg/dl)[1]。血糖长期处于异常的状态,除了会 增加患2 型糖尿病的风险,还会增加患心血管疾病、 中风和MS 的风险[2]。已有研究显示,蒙古族人群 IFG 患病率高达18.5%[3],本研究进一步分析该人群 血糖转归情况及其影响因素。
对象与方法1. 研究对象:选取内蒙古科左后旗和奈曼旗2 个乡共32 个行政村为研究地点,研究方法参见文献 [3]。研究对象为蒙古族人群,保持着传统的蒙古族 生活方式和行为习惯。经知情同意后,基线时共有 2 589 名>20 岁常住蒙古族居民参与了问卷调查、体 格测量和实验室检测。选择IFG 且无糖尿病史的人 群为观察对象。本研究经苏州大学伦理委员会审查 批准。
2. 研究方法:
(1)基线调查:于2002 年7 月至2003 年9 月开展 基线调查。自行设计问卷,由经过统一培训的调查 员进行面对面调查,内容包括年龄、性别、吸烟、饮 酒、心脑血管疾病家族史等。体格测量包括身高、体 重、WC、臀围和血压等。测量时,要求被测者着少量 单衣,脱去鞋帽测量体重,取立位测量WC和臀围。 肥胖定义参照文献[4]。血压按国际标准方法测量, 取坐位,使用水银血压计,每隔30 s 测1 次,共测3 次,取平均值。采集晨起空腹静脉血5 ml,采用静脉 血葡萄糖氧化酶法检测FPG;现场分离血清,血清标 本用作血脂、胰岛素等检测,样本-80 ℃保存。
(2)随访调查:2013 年开展随访调查。问卷调 查内容包括年龄、性别、吸烟、饮酒、糖尿病史、高血 压史、脑卒中史、心脏病史以及肾病史等一般情况以 及服药情况,死亡者调查并核对死亡原因、死亡时 间。除进行问卷调查外,还进行了体格、血压测量和 血糖检测。FPG的测定要求被测者至少禁食8 h,现 场采集静脉血,采用静脉血葡萄糖氧化酶法检测。 根据2003 年ADA《糖尿病诊断标准》,将参与者的 FPG 分为3 类:正常血糖(FPG<5.6 mmol/L),IFG (5.6 mmol/L≤FPG<7.0 mmol/L),糖尿病(FPG≥ 7.0 mmol/L)。
3. 统计学分析:将EpiData 数据库转为SAS 数 据库,运用SAS 9.2 软件进行统计学分析。正态分布 的连续性变量,包括年龄,用x±s 表示,多组均 数的比较用方差分析,两两比较采用SNK 法; 非正态分布的连续性变量,包括WC、SBP、 DBP、TC、TG、LDL-C,用M(四分位间距)表示, 采用秩和检验进行分析;计数资料用率或构成 比表示,多组率的比较采用χ2检验,两两比较采 用χ2 分割法;以2013 年FPG 检测结果为因变 量,分为正常组、IFG 组和糖尿病(DM)组,进行 单因素和多因素无序多分类logistic 回归分析 不同因素对血糖转归的影响,分别计算OR值和 95%CI。所有P值基于双侧检验和0.05 的显著 性水平,P<0.05 为差异有统计学意义。
结果1. 一般情况:基线IFG 人群共474 人,10 年中死 亡64 人(均非糖尿病死亡),随访时拒绝采血检测血 糖26 人,最终384 人纳入分析。其中有150 人 (39.1%)FPG 恢复正常,174 人(45.3%)为IFG,60 人 (15.6%)进展为DM。将调查对象分为FPG 正常、 IFG 和DM 3 组,比较分析基线各因素在3 组之间的 水平。DM组的年龄、WC以及TG均高于IFG 组和 正常组,差异具有统计学意义(均P<0.05),这3 个 指标在IFG组和FPG正常组之间的差异无统计学意 义(均P>0.05)。性别、SBP、DBP、TC、LDL-C、 HDL-C、吸烟及饮酒在3 组间差异无统计学意义 (P>0.05),见表 1。

2. IFG转为正常及进展为DM的影响因素分析:
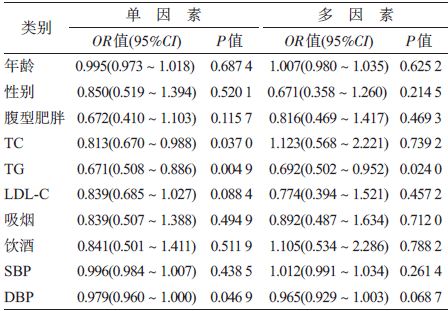
(1)IFG人群转归为正常:以2013 年FPG结果为 因变量(IFG=0,FPG 正常=1,DM=2),以年龄、性 别、腹型肥胖、TC、TG、LDL-C、吸烟、饮酒、SBP以及 DBP为自变量,做无序多分类logistic 回归分析。单 因素分析显示,TG 水平与IFG 人群恢复到正常的 OR 值(95%CI)为0.671(0.508~0.886),具有统计学 意义(P<0.05);经多因素调整后,TG水平与IFG 人 群恢复到正常的OR 值(95% CI)为0.692(0.502~ 0.952),仍然具有统计学意义(P<0.05)。年龄、性 别、腹型肥胖、TC、LDL-C、吸烟、饮酒、SBP 以及 DBP 与IFG 人群恢复到正常的关联无统计学意义 (P>0.05),见表 2。
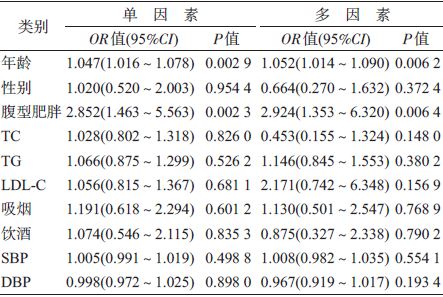
(2)IFG人群进展为DM:单因素分析显示,年龄 和腹型肥胖与IFG人群进展为DM的OR值(95%CI) 分别为1.047(1.016~1.078)和2.852(1.463~5.563), 具有统计学意义(均P<0.05)。经多因素调整后, 年龄和腹型肥胖与IFG 人群进展为DM的OR 值(95%CI)分别为1.052(1.014~1.090)和2.924(1.353~6.320)。性别、TC、TG、LDL-C、吸烟、饮酒、SBP 以 及DBP 与IFG 人群进展为DM 无关(P>0.05),见 表 3。
本研究显示,蒙古族IFG 人群经过10 年有 39.1%FPG 恢复正常,45.3%仍为IFG,15.6%进展为 DM。多因素分析显示,TG与IFG 人群恢复到正常 的OR 值为0.692;年龄与IFG 人群进展为DM的OR 值为1.052,IFG 人群中腹型肥胖者进展为DM的危 险性是非腹型肥胖者的2.924 倍,提示TG升高在蒙 古族IFG 人群恢复正常的过程中起到抑制作用,年 龄和腹型肥胖是IFG进展为DM的危险因素。
本研究中IFG 人群中15.6%的DM转化率与已 有研究结果相似[5, 6, 7, 8, 9, 10]。TG升高是IFG 人群转为正常 的抑制因素,与已有研究结果一致[7, 8, 9, 11, 12, 13, 14]。提示降 低TG水平可以降低患IFG 和DM的风险,也有利于 IFG 人群血糖转为正常水平。腹型肥胖是IFG 人群 进展为DM的危险因素,与已有研究结果一致[15, 16, 17], 提示IFG 者中有腹型肥胖的患者发展成DM的可能 性将会增大。
本研究存在局限性。首先,样本量偏少,由于研 究人群来自农村一般社区而非医院,因而其中的 IFG 人群相对较少,但可以代表一般蒙古族人群;其 次,基线时只检测了FPG,而未做餐后血糖的检测, 因而随访人群中未包括同样属于DM前期的糖耐量 受损人群。此外,本研究未评估由于运动和饮食习 惯的改变对转归结果的影响。
| [1] Genuth S, Alberti KG, Bennett P,et al. Follow-up report on the diagnosis of diabetes mellitus[J]. Diabetes Care,2003,26(11):3160-3167. |
| [2] Wen CP,Cheng TY,Tsai SP,et al. Increased mortality risks of pre-diabetes (impaired fasting glucose) in Taiwan[J]. Diabetes Care,2005,28(11):2756-2761. |
| [3] Zhang S,Tong W,Xu T,et al. Diabetes and impaired fasting glucose in Mongolian population,Inner Mongolia,China[J]. Diabetes Res Clin Pract,2009,86(2): 124-129. |
| [4] Alberti KG,Zimmet P,Shaw J,et al. IDF Epidemiology Task Force Consensus Group. The metabolic syndrome—a new worldwide definition[J]. Lancet,2005,366(9491 ):1059-1062. |
| [5] Neumann A,Norberg M,Schoffer O,et al. Risk equations for the development of worsened glucose status and type 2 diabetes mellitus in a Swedish intervention program [ J]. BMC Public Health,2013,13:1014. |
| [6] Lecomte P,Vol S,Cacès E,et al. Five-year predictive factors of type 2 diabetes in men with impaired fasting glucose[J]. Diabetes Metab,2007,33(2):140-147. |
| [7] Chen KT,Chen CJ,Gregg EW,et al. Impaired fasting glucose and risk of diabetes in Taiwan: follow-up over 3 years[J].Diabetes Res Clin Pract,2003,60(3): 177-182. |
| [8] Shaw JE,Zimmet PZ,de Courten M,et al. Impaired fasting glucose or impaired glucose tolerance. What best predicts future diabetes in Mauritius?[J]. Diabetes Care, 1999,22(3):399-402. |
| [9] Söderberg S, Zimmet P, Tuomilehto J,et al. High incidence of type 2 diabetes and increasing conversion rates from impaired fasting glucose and impaired glucose tolerance to diabetes in Mauritius[J]. Intern Med,2004,256(1):37-47. |
| [10] Wu YT,Xing AJ,Wu SL,et al. Natural outcome and its correlated factors in patients with impaired fasting glucose[J]. Chin J Diabetes,2013,21(8):728-730. (in Chinese) 吴云涛,邢爱君,吴寿岭,等. 空腹血糖受损人群自然转归及其影响因素的观察[J]. 中国糖尿病杂志,2013,21(8):728-730. |
| [11] Lin SX,Berlin I,Younge R,et al. Does elevated plasma triglyceride level independently predict impaired fasting glucose?: the Multi-Ethnic Study of Atherosclerosis (MESA) [J]. Diabetes Care,2013,36(2):342-347. |
| [12] Schmidt MI,Duncan BB,Bang H,et al. Identifying individuals at high risk for diabetes: the atherosclerosis risk in communities study[J]. Diabetes Care,2005,28(8) :2013-2018. |
| [13] Svedberg J,Björntorp P,Lönnroth P,et al. Prevention of inhibitory effect of free fatty acids on insulin binding and action in isolated rat hepatocytes by etomoxir[J] . Diabetes,1991,40(6):783-786. |
| [14] Golay A,Swislocki AL,Chen YD,et al. Relationships between plasma-free fatty acid concentration,endogenous glucose production,and fasting hyperglycemia in normal and non-insulin-dependent diabetic individuals[J]. Metabolism,1987,36(7):692-696. |
| [15] Baena-Díez JM, Elosua R, Cano JF,et al. Waist circumference and impaired fasting glucose screening in a Mediterranean population[J]. Diabetes Res Clin Pract,2009 ,86(2):e12-14. |
| [16] Carba DB,Bas IN,Gultiano SA,et al. Waist circumference and the risk of hypertension and prediabetes among Filipino women[J]. Eur J Nutr,2013,52(2):825-832. |
| [17] Wahrenberg H,Hertel K,Leijonhufvud BM,et al. Use of waist circumference to predict insulin resistance: retrospective study[J]. BMJ,2005,330(7504):1363-1364. |