 2014, Vol. 35
2014, Vol. 35文章信息
- 黄宇玲, 王志军, 刘雪梅, 李雯, 王迈, 陈朔华, 吴寿岭. 2014.
- Huang Yuling, Wang Zhijun, Liu Xuemei, Li Wen, Wang Mai, Chen Shuohua, Wu Shouling. 2014.
- 中老年人群高静息心率对颈动脉斑块检出率的影响
- Effect of high resting heart rate on the detection rate of carotid artery plaque in elderly population
- 中华流行病学杂志, 2014, 35(9): 1053-1057
- Chinese Journal of Epidemiology, 2014, 35(9): 1053-1057
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2014.09.019
-
文章历史
- 投稿日期:2014-5-12




2 河北联合大学附属医院心内科;
3 开滦总医院超声科;
4 开滦总医院重症医学科;
5 开滦总医院心内科
2 Department of Cardiology, Affiliated Hospital of Hebei United University;
3 Department of Ultrasonography, Kailuan General Hospital of Heibei United University;
4 Department of Internal Medicine, Kailuan General Hospital of Heibei United University;
5 Department of Cardiology, Kailuan General Hospital of Heibei United University
高静息心率是指静息状态时每分钟心率80~85次。近年研究报道高静息心率人群易发生高血压等疾病[1, 2, 3, 4, 5],而后者又是动脉粥样硬化的危险因素,提示高静息心率与动脉粥样硬化有一定关联。动物试验也发现心率直接影响动脉粥样硬化,而药物或窦房结消融术减低心率能延缓和阻止动脉粥样硬化的进展[6]。但高静息心率是否为动脉粥样硬化的危险因素,尚无定论。目前高静息心率与动脉粥样硬化关系的大样本流行病学研究甚少。颈动脉斑块是反映全身动脉粥样硬化病变的一个“窗口”[7],可作为动脉粥样硬化早期评价的指标。为此,本研究依据开滦研究(注册号:CHiCTR-TNC-11001489)资料,探讨中老年人群高静息心率对颈动脉斑块检出率的影响。
对象与方法1. 研究对象:本研究为开滦研究的一部分。开滦研究为在2006-2007年度101 510名开滦集团公司健康体检职工中,按照2005年全国1%抽样调查所得≥40岁全国人口性别和年龄的比例,根据每2岁一个年龄段按比例分层随机抽取5 852人组成研究人群,于2010年6月至2011年6月对该人群进行第3次体检,详细情况见相关文献[8, 9]。入选标准为种族、性别不限,年龄≥40岁,认知能力无缺陷可完成问卷并同意参加本研究者;排除标准为身体严重残疾不能接受检查,既往有缺血性脑卒中、短暂性脑缺血发作(不包括腔隙性梗死)、心肌梗死且不同意参加本研究者。共入组符合标准者5 440人。
2. 研究方法:
(1)资料收集:设计流行病学调查表,制定统一的填写指南,收集入选人群的资料,包括人口学特征、职业状况、行为习惯(睡眠、吸烟、饮酒、体育锻炼及膳食)、疾病史与家族史等。调查员及体检医生均为固定人员且经过统一培训,采取面对面逐一询问调查方式。
(2)人体测量:按常规方法采用经校正的RGZ-120型体质量秤测量身高(精确到1 mm)和体质量(精确到0.1 kg),并计算BMI(kg/m2)。采用经校正的台式水银血压计测量右侧肱动脉血压,SBP读数取柯氏音第1时相,DBP读数取柯氏音第5时相,连续测量3次,每次测量间隔1~2 min,取均值。
(3)静息心率检测:受试者在安静状态下平卧休息10 min后,用12导联心电图记录标准12导联心电图,选择Ⅱ导联,连续描记10个心动周期,用平均R-R间期计算心率。
(4)颈部血管超声检查:由经过统一培训且从事超声工作5年以上的医生进行检查。采用PHILIPS公司HD-15彩色超声诊断仪(高频探头,频率7.5 MHz)。患者取平卧位,头部偏向检查对侧,充分暴露颈部,探头轻轻置于颈前部气管外侧,扫查双侧颈总动脉、颈内动脉及颈外动脉,记录血管内膜中层厚度(IMT),观察有无斑块及其大小。斑块定义:局部隆起突出于动脉管腔>0.5 mm,或超过环绕IMT值的50%或IMT>1.5 mm[10]。由2名具有5年以上工作经验的超声医师依据上述标准共同判断确认,并由不同的超声专科医师随机重查颈动脉超声并重新判断IMT及斑块结果,重测信度为97%。
(5)实验室检测:晨空腹抽取肘静脉血5 ml,分离并提取血清用于生物化学指标检测。包括TC、TG、FPG、HDL-C、LDL-C、高敏C反应蛋白(hs-CRP)、UA等。生物化学指标检测统一用日立7600自动生物化学分析仪,由同一组专业检验师操作。
3. 诊断标准及定义:高血压诊断采用《中国高血压防治指南2010》标准[11],即SBP≥140 mmHg(1 mmHg=0.133 kPa)和/或DBP≥90 mmHg,或正在服用抗高血压药物者;糖尿病诊断标准为FPG≥7.0或<7.0 mmol/L既往已确诊为糖尿病并使用降糖药物者[12];吸烟定义为近1年平均每天至少吸1支烟;饮酒定义为每日酒精摄入量>25 g(即白酒80 ml,葡萄酒200 ml,啤酒600 ml),既往饮酒现已戒酒为不饮酒。
4. 统计学分析:所有数据由双人录入,建立EpiData数据库,应用SPSS 13.0软件进行统计学处理。正态性计量资料以x±s表示,组间比较用独立样本t检验;计数资料用百分数(%)表示,两两比较采用χ2检验,采用单因素、多因素非条件logistic回归模型分析高静息心率对颈动脉斑块的影响,以P<0.05为差异有统计学意义。
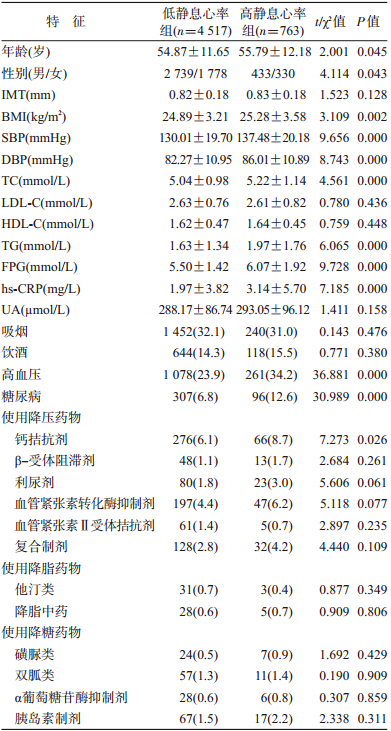
结 果1. 一般特征:5 440名入组对象中有56例心电图确诊心律失常、74例心率资料不完整、30例未行颈动脉斑块检测,最终纳入统计分析的有效数据为5 280例(男3 172例,女2 108例),年龄(55.0±11.7)岁。根据静息心率水平分为≤80次/分(低静息心率组)和>80次/分(高静息心率组),两组人群的年龄、性别、BMI、SBP、DBP、TC、TG、FPG、hs-CRP及患高血压、糖尿病所占百分比和钙拮抗剂使用情况的差异有统计学意义(P<0.05或P<0.001);两组间IMT、LDL-C、HDL-C、UA、吸烟、饮酒及服降压、降脂、降糖药物情况的差异无统计学意义(P>0.05),见表 1。
2. 不同性别人群颈动脉斑块检出率:两组人群颈动脉斑块检出率为42.6%,其中高、低静息心率组颈动脉斑块检出率分别为48.9%、41.5%,差异有统计学意义。男性人群颈动脉斑块检出率为53.0%,高、低静息心率组颈动脉斑块检出率分别为58.7%、52.1%,差异有统计学意义;女性人群颈动脉斑块检出率为26.9%,高、低静息心率组颈动脉斑块检出率分别为36.1%、25.1%,差异有统计学意义(表 2)。

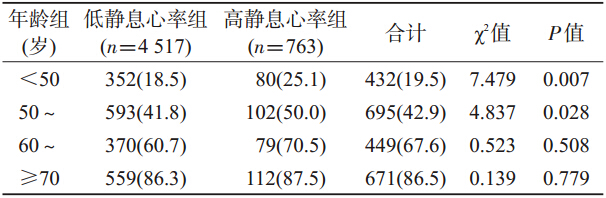
3. 不同年龄分层人群颈动脉斑块检出率:年龄<50、50~、60~、≥70岁人群颈动脉斑块检出率分别为19.5%、42.9%、67.6%、86.5%,显示随年龄增长,颈动脉斑块检出率增加。在年龄<50和50~岁人群,高静息心率组颈动脉斑块检出率高于低静息心率组,差异有统计学意义(P<0.05);而年龄60~和≥70岁人群,高、低静息心率组颈动脉斑块检出率比较差异无统计学意义(表 3)。
4. 颈动脉斑块logistic回归分析:以颈动脉有无斑块为因变量,将静息心率、年龄、性别、血脂各项指标、高血压、糖尿病、吸烟等一起进入方程进行logistic回归分析。单因素分析高静息心率组发生颈动脉斑块的风险是低静息心率组的1.35倍。校正年龄、性别后高静息心率组发生颈动脉斑块的风险是低静息心率组的1.44倍。校正年龄、性别和其他危险因素后高静息心率组发生颈动脉斑块的风险是低静息心率组的1.23倍(表 4)。
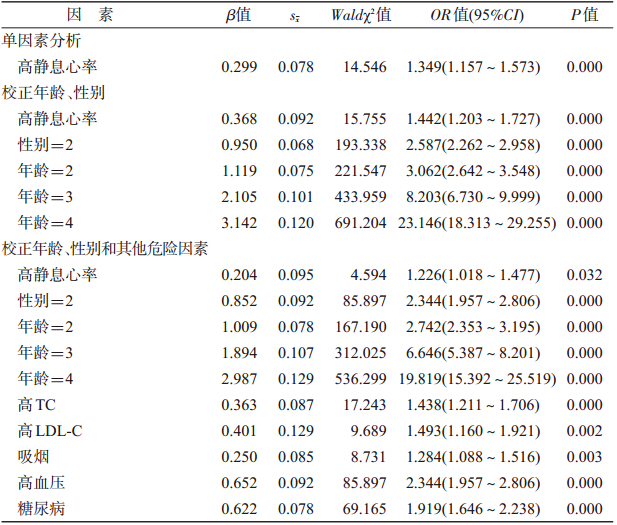 | |||||
| 注: 性别:女性=1,男性=2; 年龄:40~49岁=1,50~59岁=2,60~69岁=3,≥70岁=4; TC≤5.72 mmol/L=1,TC>5.72 mmol/L=2;LDL-C≤3.64 mmol/L=1,LDL-C>3.64 mmol/L=2;HDL-C≥0.91 mmol/L=1,HDL-C<0.91 mmol/L=2; TG≤1.70 mmol/L=1,TG >1.70 mmol/L=2; 吸烟:否=1,是=2; 饮酒:否=1,是=2; 高血压:否=1,是=2;糖尿病:否=1,是=2 | |||||
动脉粥样硬化是心血管疾病发生最重要的病理基础,而高血压、糖尿病、血脂异常、肥胖等是其传统的可控危险因素。高静息心率是交感神经系统激活的一个可靠指标,近年研究报道交感神经系统异常激活可导致血压、血糖水平升高和胰岛素抵抗,进而发现高静息心率与高血压、糖尿病等关系密切[13, 14, 15],但高静息心率能否增加动脉粥样硬化的发生风险,尚无定论。
颈动脉斑块是动脉粥样硬化的临床标志。本研究发现无论是总体人群,还是男性或女性人群,高静息心率组颈动脉斑块检出率均高于低静息心率组(P<0.05),与国内报道类似[16, 17]。高血压及糖、脂代谢异常可引起高静息心率,而高静息心率又可加重高血压及糖、脂代谢紊乱的发生发展[2]。本研究中高静息心率组BMI、SBP、DBP、TC、TG、FPG水平明显高于低静息心率组(P<0.05)。提示高静息心率可能与动脉粥样硬化的其他危险因素相互作用并协同促进了颈动脉斑块的发生。
年龄是动脉粥样硬化形成的主要危险因素[18],随着年龄增加,动脉硬化或动脉斑块的发生概率增加。本研究也发现颈动脉斑块的检出率随年龄增长而增加,如60~69岁年龄组人群斑块检出率为67.6%,≥70岁组人群斑块检出率为87.5%,均高于西方发达国家报道[19]。在年龄<50岁和50~59岁人群中高静息心率组颈动脉斑块检出率高于低静息心率组,而60~69岁和≥70岁人群中,颈动脉斑块检出率的差异无统计学意义。分析原因可能随着年龄的增长,年龄与其他危险因素的合并作用削弱了高静息心率对颈动脉斑块的影响。提示对于年龄<60岁即老年前期人群,更应关注其心率。
传统危险因素可影响颈动脉斑块的检出率[20, 21],为此本研究校正了这些危险因素,结果高静息心率组与低静息心率组比较颈动脉斑块发生风险仍有增加(OR=1.226,95%CI:1.018~1.477,P<0.05)。Shigetoh等[3]报道高静息心率患者发生胰岛素抵抗、肥胖、糖尿病的概率分别是静息心率(<60次/分)的1.20、1.34和4.39倍。Inoue等[1]对4 331名正常血压人群进行3年的随访,校正其他因素后结果显示静息心率>70次/分者发生高血压风险是静息心率≤58次/分者的1.6倍。进一步支持高静息心率能增加颈动脉斑块的发生风险。
高静息心率对颈动脉斑块的发生有一定的促进作用。其可能机制[22, 23]:高静息心率能增加血流在颈动脉内的搏动性,并产生沿切应力方向的震荡,致使血流速度和方向发生改变,使血管内皮释放一氧化氮和其他的血管活性物质,导致血管内皮受损和通透性增加;也可增加血管外周阻力,严重时易发生内皮破裂,脂质渗透入血管壁,从而诱发和加重颈部血管动脉粥样硬化;并能明显延长血管处于高张力状态的时间,进一步导致血管张力增高,动脉弹性降低或硬化;还能增加血管壁氧化应激水平,促进颈部动脉粥样硬化形成。
在多因素logistic回归分析中,在高静息心率组传统的危险因素(高龄、高血压、糖尿病、高TC、吸烟等)明显影响颈动脉斑块的发生,尤其是年龄,≥70岁年龄组颈动脉斑块的发生风险约是<50岁年龄组的20倍。提示防治动脉粥样硬化的重点仍是加强传统危险因素的综合控制。针对高静息心率的干预措施,目前主要提倡改善生活方式、适度有氧运动、减缓工作压力和心理调整。
本文为横断面研究,存在一定局限性。首先研究中未能考虑到影响静息心率的情绪、精神心理等因素,故判断其临床意义方面可能受到一定影响;其次,未能排除人群中服用药物等情况对颈动脉斑块的影响。但由于研究样本量大,仍可反映高静息心率能增加颈动脉斑块的发生风险,对<60岁年龄人群早期干预高静息心率对其动脉粥样硬化的防治有一定意义。
| [1] Inoue T,Iseki K,Iseki C,et al. Higher heart rate predicts the risk of developing hypertension in a normotensive screened cohort[J]. Circ J,2007,71(11):1755-1760. |
| [2] Palatini P,Dorigatti F,Zaetta V,et al. Heart rate as a predictor of development of sustained hypertension in subjects screened for stage 1 hypertension:the HARVEST study[J]. J Hypertens,2006,24(9):1873-1880. |
| [3] Shigetoh Y,Adachi H,Yamagishi S,et al. Higher heart rate may predispose to obesity and diabetes mellitus:20-year prospective study in a general population[J]. Am J Hypertens,2009,22(2):151-155. |
| [4] Fernandes RA,Ronque ERV,Venturini D, et al. Resting heart rate:its correlations and potential for screening metabolic dysfuctions in adolescents[J]. BMC Pediatr ,2013,13(1):48-54. |
| [5] Palatini P, Mos L,Santonastaso M,et al. Resting heart rate as a predictor of body weight gain in the early stage of hypertension[J]. Obesity(Sliver Spring),2011 ,19(3):618-623. |
| [6] Custodis F, Schirmer SH, Baumhäkel M, et al. Vascular pathophysiology in response to increased heart rate[J]. J Am Coll Cardiol,2010,56(24):1973-1983. |
| [7] Shah PK. Screening asymptomatic subjects for subclinical atherosclerosis:can we,does it matter,and should we?[J]. J Am Coll Cardiol,2010,56(2):98-105. |
| [8] Yao T, Wang ZF, Li L, et al. Relations between serum homocysteinemia and carotid artery plaques[J]. Chin J Epidemiol,2012,33(8):846-849. (in Chinese) 姚涛,王张锋,李丽,等. 血同型半胱氨酸水平与颈动脉斑块的相关性研究[J]. 中华流行病学杂志,2012,33(8):846-849. |
| [9] Li W,Zhou Y,Liu XM,et al. The detection rate and influential factors of carotid artery plaque in the elderly population[J]. Chin J Hypertens,2012,20(3):232-236. (in Chinese) 李雯,周勇,刘雪梅,等. 中老年人群颈动脉斑块的检出率及其影响因素[J]. 中华高血压杂志,2012,20(3):232-236. |
| [10] Sztajzel R. Ultrasonographic assessment of the morphological characteristics of the carotid plaque[J]. Swiss Med Wkly,2005,135(43/44):635-643. |
| [11] Writing Group of 2010 Chinese Guidelines for the Management of Hypertension. 2010 Chinese guidelines for the management of hypertension[J]. Chin J Hypertens,2011, 19(8):701-743. (in Chinese) 中国高血压防治指南修订委员会. 中国高血压防治指南2010[J]. 中华高血压杂志,2011,19(8):701-743. |
| [12] Genuth S,Alberti KG,Bennett P,et al. Expert committee on the diagnosis and classification of diabetes mellitus:follow-up report on the diagnosis of diabetes mellitus[J]. Diabetes Care,2003,26(11):3160-3167. |
| [13] Aleksandra P, Walerian P, Grazyna B,et al. The relationship between resting heart rate and atherosclerosis is risk factors[J]. Kardilo Pol,2008,66(10):1069-1075. |
| [14] Mancia G, Bousquet P, Elghozi JL,et al. The sympathetic nervous system and the metabolic syndrome[J]. J Hypertens,2007,25(5):909-920. |
| [15] Shibao C,Gamboa A,Diedrich A, et al. Autonomic contribution to blood pressure and metabolism in obesity[J]. Hypertension,2007,49(1):27-33. |
| [16] Liu P,Wang SJ,Zhang Y. The relationship between resting heart rate and target organs damage in senile essential hypertension[J]. Chin J Cardiol,2005,33(1):49-53. (in Chinese) 刘平,王苏加,张运. 老年高血压患者的静息心率增加与靶器官损害的相关性研究[J]. 中华心血管病杂志,2005,33(1):49-53. |
| [17] Tang WH,Zhang Q,Chen XJ. Analysis of correlation between resting heart rate and carotid artery disease in patients with cerebral infarction[J]. J Guangdong Med, 2011,32(19):2531-2533. (in Chinese) 唐文红,张琴,陈晓婕. 脑梗死患者静息心率与颈动脉病变相关性分析[J]. 广东医学,2011,32(19):2531-2533. |
| [18] den Ouden ME, Schuurmans MJ,Arts IE,et al. Atherosclerosis and physical fuctioning in older men,a longitudinal study[J]. J Nutr Health Aging,2013,17(1):97-104. |
| [19] Johnsen SH, Mathiesen EB, Joakimsen O, et al. Carotid atherosclerosis is a stronger predictor of myocardial infarction in women than in men:a 6-year follow-up study of 6 226 persons:the tromse study[J]. Sroke,2007,38(11):2873-2880. |
| [20] Chow CK,Mcquillan B,Raju PK, et al. Greater adverse effects of cholesterol and diabetes on carotid intima-media thickness in South Asian Indians:comparison of risk factor-IMT associations in two population-based surveys[J]. Atherosclerosis,2008,199(1):116-122. |
| [21] Yu RH,Ho SC,Ho SS,et al. Carotid atherosclerosis and the risk factors in early postmenopausal Chinese women[J]. Maturitas,2009,63(3):233-239. |
| [22] Giannoglou GD,Chatzizisis YS,Zamboulis C,et al. Elevated heart rate and atherosclerosis is an overview of the pathogenetic mechanisms[J]. Int J Cardiol,2008,126 (3):302-312. |
| [23] Bolduc V, Drouin A,Gillis MA, et al. Heart rate-associated mechanical stress impairs carotid but not cerebral artery compliance in dyslipidemic atherosclerotic mice[J]. Am J Physiol Heart Circ Physiol,2011,301(5):H2081-2092. |