 2014, Vol. 35
2014, Vol. 35文章信息
- 王胜锋, 刘清, 刘庆敏, 任艳军, 吕筠, 李立明. 2014.
- Wang Shengfeng, Liu Qing, Liu Qingmin, Ren Yanjun, Lyu Jun, Li Liming. 2014.
- 综合干预对杭州市社区医务人员提供戒烟咨询的效果及影响因素分析
- Assessment on the impact of smoking cessation counseling service and related influencing factors under comprehensive community-based intervention programs about the community medical staff in Hangzhou city
- 中华流行病学杂志, 2014, 35(9): 1002-1006
- Chinese Journal of Epidemiology, 2014, 35(9): 1002-1006
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2014.09.007
-
文章历史
- 投稿日期:2014-4-24




2 杭州市疾病预防控制中心
2 Hangzhou Center for Disease Control and Prevention
2009年,美国将戒烟咨询和干预纳入以社区医务人员为核心的临床预防服务工作重点的范畴[1],其中最重要的两点为询问(ask)和建议(advice)[2]。然而,大多数国家的社区卫生中心实际开展戒烟咨询的水平仍较低,国外已开展对应的干预研究,效果并不如意[3, 4, 5, 6],而国内仍为空白。本研究基于社区健康干预(CIH)[7],评价综合干预对社区医务人员提供戒烟咨询的短期效果及影响因素,以期更有效激励社区医务人员发挥带动患者戒烟的作用。
对象与方法1. 调查对象:选择社区卫生服务中心有较多机会接触患者并与其交流的医务人员,涉及科室包括内科、外科、五官科、预防保健科、针灸科、口腔科、中医推拿科等。全部接受调查,未进行抽样。基线、随访分为2次独立的横断面调查,分别于2008年11-12月完成940人(应答率92.2%)、2011年7-10月完成870人(应答率94.1%)。因人员变动频繁,前后仅440人一致,为更好的评价干预本身的效果,本研究仅分析这部分人群。
2. 调查内容:采用国际项目组统一设计的问卷包括①一般情况(性别、年龄、平均每周接诊量、自身吸烟状况等);②接受的戒烟知识技能培训、咨询建议的准备情况;③可获取及实际利用的资源;④戒烟咨询行为(交流吸烟情况、吸烟危害和指导如何戒烟)。
3. 干预活动:干预为期2年,包括:①定期开展技能讲座培训;②分发宣传资料和手册;③制作指导戒烟的提醒台历;④鼓励医务人员对接诊患者进行生活方式危险因素的筛查和指导;⑤鼓励医务人员向社区居民发放宣传资料。2009年中旬至2011年中旬在干预区(下城区、拱墅区各4个社区卫生服务中心)开展。同期,对照区6个社区卫生服务中心不采取项目相关的干预活动,但允许开展常规实践。结局评价:①接受戒烟培训的比例和种类;②戒烟资源的可获取比例和种类;③戒烟资源的利用比例和种类:④戒烟咨询的准备情况;⑤对≥90%的患者提供戒烟咨询(包括询问吸烟状况、告知吸烟危害、给予戒烟建议)的比例。
4. 统计学分析:数据录入采用EpiData 3.1软件,分析使用SPSS 20.0软件。连续变量使用x±s(偏态分布采用四分位数),分类变量使用频数(构成比)。组间连续变量的均值比较使用独立样本t检验,无序及有序分类变量分别采用χ2检验、非参数秩和检验(Mann-Whitney)。分析影响因素采用logistic回归,参考平行线检验选择Ordinal或Multinomial。变化量构建采用结局-基线,并以此分为变差(差值<0)、不变(差值=0)和变好(差值>0)3组。
结 果1. 基本情况:2次调查均参与者440人(46.8%),相比失访者,这一人群更为年轻(34.1岁vs. 37.3岁,P<0.001),医生比例较高(65.5% vs. 59.0%,P=0.042),其余差异均无统计学意义。干预区299人,男性占22.3%,吸烟率(包括既往吸烟)约5%,平均每周接诊量>100人的比例高于65%。对照区141人,各特征与干预区差异均无统计学意义(表 1)。
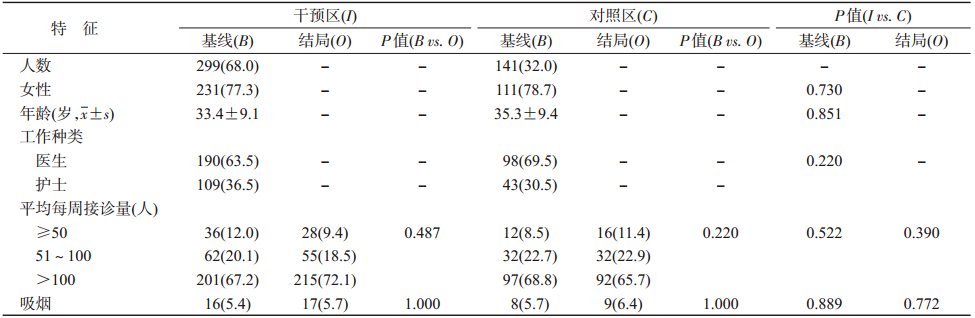 | ||||||||
| 注:括号外数据为人数,括号内数据为构成比(%);“基线”、“结局”分别代表 2008年、2011年调查情况;因个体自身前后配对,对不随时间改变的变量,仅比较“基线”一列,“-”代表不适用 | ||||||||
2. 干预效果评价:
(1)戒烟培训:干预前后,干预区至少接受过1种戒烟培训的比例从65.6%提高至75.9%、接受种类从平均1种增加至2种(P=0.004),对照区至少接受过1种戒烟培训的比例从52.5%提高至59.6%(P=0.220)、接受种类只有1种。增幅最明显的均为参加会议和研讨会(表 2)。
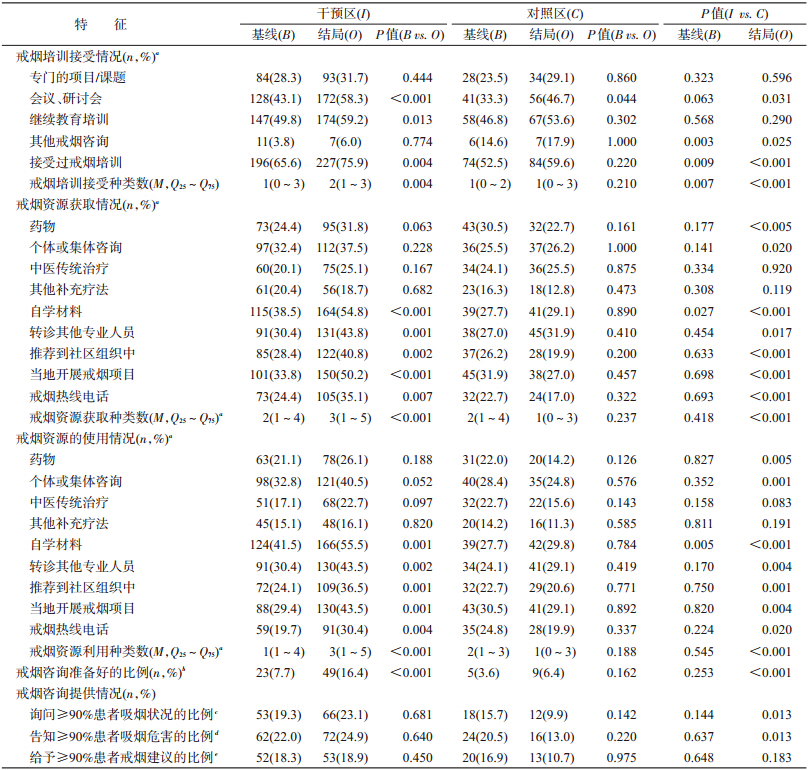 | ||||||||
| 注:a、b、c、d、e对应基线分别存在0、2、50、41、38个缺失,结局分别存在0、2、33、28、37个缺失 | ||||||||
(2)戒烟资源可获取比例:干预区干预后有5种资源明显提高,对照区9种资源均未提高,甚至4种呈下降趋势。戒烟资源使用比例的变化趋势与其完全一致。自学材料的可获取及实际使用比例均最高,分别仅为54.8%、55.5%。干预前后,干预区戒烟资源获取数量从平均2种上升至3种(P<0.001),对照区从平均2种减少为1种(P=0.237)。干预前后,干预区戒烟资源使用数量从平均1种上升至3种(P<0.001),对照区从平均2种减少为1种(P=0.188)。
(3)准备情况:干预区准备好戒烟咨询的比例前后分别为35.5%、52.0%(P<0.001),对照区前后分别为28.1%、39.3%(P=0.162)。就实际行动,干预区能对≥90%的患者提供戒烟咨询的医务人员比例呈小幅上升趋势,而对照区呈下降趋势。 调整基线性别、年龄、戒烟培训种类后,干预区获取、利用戒烟资源、戒烟咨询准备水平变好的概率分别是对照组的3.02、2.62、1.47倍(P分别为<0.001、<0.001、0.049),见表 3。
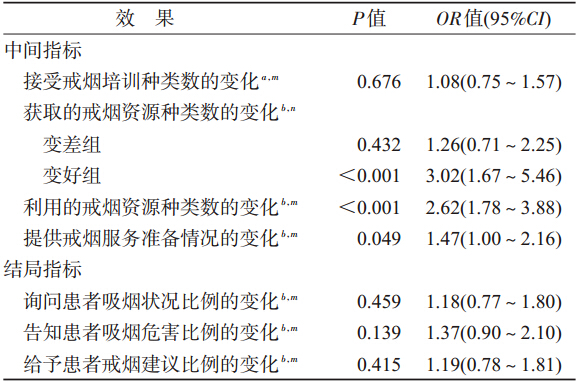 | ||
| 注:a 调整年龄、性别;b 调整年龄、性别、可利用戒烟资源数; m Ordinal logistic regression;n Multinominal logistic regression | ||
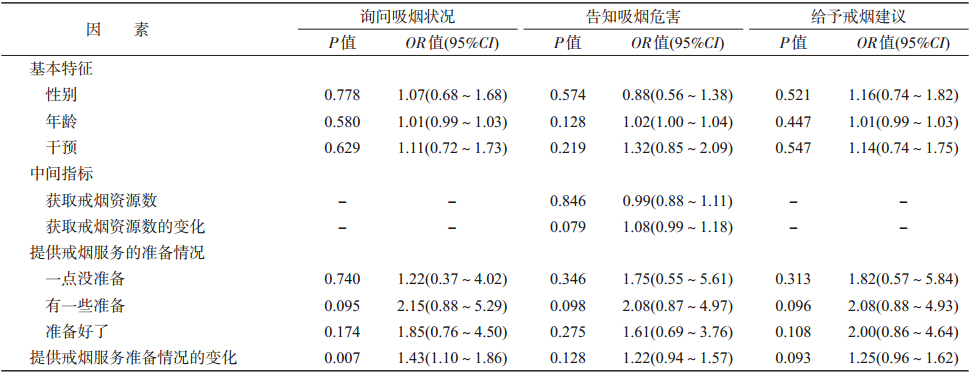
3. 统计学分析:单因素分析,未发现年龄、性别、自身吸烟状况、干预措施、戒烟资源与戒烟咨询变化之间的关联,仅戒烟咨询准备情况改善,有助于提供3种戒烟咨询(均P<0.05);经多变量调整后,戒烟咨询准备情况改善仅有助于提高医务人员询问患者吸烟状况的比例(调整OR=1.43,P=0.007),见表 4。
CIH项目干预旨在提高社区医务人员所提供戒烟咨询的水平,近两年干预后,干预区医务人员获取戒烟资源及咨询准备情况有明显提升,但戒烟咨询的询问和建议行为却未见改善。本研究未发现年龄、性别、自身吸烟状况、干预措施、戒烟资源与戒烟咨询之间的关联,提示自身准备情况的改善会促进医务人员询问患者吸烟状况。
干预后,干预区在戒烟培训、资源、咨询准备方面均有明显改善。参考国外同类研究,准备情况较好的医生能够更多的利用戒烟资源,也倾向于提供更多的戒烟咨询[3, 4, 5, 8],但本研究中向≥90%的患者提供3种戒烟咨询的医务人员比例始终维持在20%,并无显著改善。这与Ockene等[3]针对1283名社区医务人员的干预结果一致,显著低于Herie等[9, 10, 11]研究结果。究其原因,可能包括:第一,国内医疗体系支持的不足。Lam等[12]指出医院的支持对医务人员提供戒烟咨询非常关键。目前美国17%的医院规定医生必行戒烟咨询,另有15%的医院将其纳入医生绩效考核[13],而国内尚无类似要求,导致服务价值难以体现,损害积极性[9, 12, 14]。第二,干预强度可能有所欠缺。本研究干预基本与其常规工作相融合,所有培训均自愿参加,非强制要求,导致实际参与比例较低(培训参与率最高项仍不足60%),这与Ockene等[3]研究较为相似。
本研究未发现社区医务人员的性别、年龄与戒烟咨询变化之间存在关联,与Gunes等[15]和Mcavoy等[16]研究结果一致。既往研究发现,医务人员自身吸烟会导致其对患者吸烟的默认或劝阻力度的降低[8, 12, 14, 17, 18, 19],但此次未证实,考虑与调查中吸烟率(约5%)明显低于其他研究(约50%)有关。Polyzos等[20]发现,53%~70%的社区医务人员因日常工作量较大而无暇提供戒烟咨询,但本研究及Lam等[12]在我国进行的研究均未发现每周接诊量与提供戒烟咨询的关联。原因考虑与每周接诊量的划分有关,前者为医务人员对其工作量的主观赋值[20],而本研究分为3个具体等级,相对更为客观。
本次干预研究,未发现社区医务人员接受干预与其戒烟咨询变化之间的关联,与Zhou等[8]在南宁的研究结果一致,但不同于Lam等[12]与López-De-Munain等[19]的结果。考虑主要由于干预前后的戒烟咨询水平变化幅度及变异度均较小,不易发现其影响因素。此外,本研究所得干预OR<1.10,把握度分析提示,样本量有所欠缺。准备情况的改善会促进医务人员提供戒烟咨询,这与已有研究一致[8],一定程度提示干预价值。但应注意,基线准备较好的医务人员存在戒烟咨询水平下降的情况,反映出即便准备情况较好的医务人员也难以持续戒烟咨询,某种程度上再次提示现行体制下相关激励或绩效可能存在问题[9, 12, 14]。其实,制度的弊漏不仅影响到行为的持续,同时影响到行为的启动,正如本研究所反映的尽管干预后戒烟培训、戒烟资源、戒烟咨询准备情况均有改善,但真正开始戒烟咨询的人员比例却并无改观。
本研究存在局限性。第一,440名分析对象仅占基线人数的47%,且医生比例较高,一定程度影响其代表性。但不可否认,该数据反映了社区医务人员的真实流动情况,尤其护士流动性大于医生。因离开者继续戒烟咨询的可能性很低,纳入者其实是对社区卫生服务中心内工作稳定性相对较高群体的一个体现,更贴近真实期望的干预效果。当然,人员流动性较大本身也反映出持续干预的必要性;第二,干预仅两年,较国外研究短[3],而服务的改善可能需要更长时间观察;第三,干预与对照仅按行政区人为划分而未随机分组,可能导致干预区和对照区的实际工作情况存在差异,尤其对照区可能常规慢性病防治工作表现较好,这种情况使得本研究所发现的干预效果更趋于保守。
| [1] U. S. Preventive Services Task Force. USPSTF A and B Recommendations[R/OL]. (2014-06-26). http://www.uspreventiveservicestaskforce.org/uspstf/uspsabrecs.html. |
| [2] Clinical Practice Guideline Treating Tobacco Use and Dependence 2008 Update Panel,Liaisons,and Staff. A clinical practice guideline for treating tobacco use and dependence:2008 update. A U.S. Public Health Service report[J]. Am J Prev Med,2008,35(2):158-176. |
| [3] Ockene JK, Lindsay EA, Hymowitz N,et al. Tobacco control activities of primary-care physicians in the Community Intervention Trial for Smoking Cessation. COMMIT Research Group[J]. Tob Control,1997,6 Suppl 2:S49-56. |
| [4] Young JM, D'Este C, Ward JE. Improving family physicians' use of evidence-based smoking cessation strategies:a cluster randomization trial[J]. Prev Med,2002,35 (6):572-583. |
| [5] Duncan C, Stein MJ, Cummings SR. Staff involvement and special follow-up time increase physicians' counseling about smoking cessation:a controlled trial[J]. Am J Public Health,1991,81(7):899-901. |
| [6] Crooks CE,Kenney E,Elder JP, et al. Tobacco control activities of primary care physicians in California results of the statewide independent evaluation of primary health care providers[J]. Eval Health Prof,1993,16(3):311-321. |
| [7] Duffany KOC,Finegood DT, Matthews D, et al. Community Interventions for Health (CIH):a novel approach to tackling the worldwide epidemic of chronic diseases[J]. CVD Prev Control,2011,6(2):47-56. |
| [8] Zhou J, Abdullah AS, Pun VC, et al. Smoking status and cessation counseling practices among physicians,Guangxi,China,2007[J]. Prev Chronic Dis,2010,7(1): 1-10. |
| [9] Herie M, Connolly H, Voci S,et al. Changing practitioner behavior and building capacity in tobacco cessation treatment:the TEACH project[J]. Patient Educ Couns ,2012,86(1):49-56. |
| [10] Rindal DB, Rush WA, Schleyer TK,et al. Computer-assisted guidance for dental office tobacco-cessation counseling:a randomized controlled trial[J]. Am J Prev Med ,2013,44(3):260-264. |
| [11] Strayer SM, Heim SW, Rollins LK, et al. Improving smoking cessation counseling using a point-of-care health intervention tool (IT):From the Virginia Practice Support and Research Network(VaPSRN)[J]. J Am Board Fam Med,2013,26(2):116-125. |
| [12] Lam TH,Jiang C,Chan YF,et al. Smoking cessation intervention practices in Chinese physicians:do gender and smoking status matter?[J]. Health Soc Care Community, 2011,19(2):126-137. |
| [13] Mcmenamin SB,Schauffler HH,Shortell SM,et al. Support for smoking cessation interventions in physician organizations:results from a national study[J]. Med Care,2003 ,41(12):1396-1406. |
| [14] Brotons C,Björkelund C,Bulc M,et al. Prevention and health promotion in clinical practice:the views of general practitioners in Europe[J]. Prev Med,2005,40(5): 595-601. |
| [15] Gunes G,Karaoglu L, Genc MF, et al. University hospital physicians' attitudes and practices for smoking cessation counseling in Malatya,Turkey[J]. Patient Educ Couns,2005,56(2):147-153. |
| [16] Mcavoy BR,Kaner EF,Lock CA,et al. Our Healthier Nation:are general practitioners willing and able to deliver?A survey of attitudes to and involvement in health promotion and lifestyle counselling[J]. Br J Gen Pract,1999,49(440):187-190. |
| [17] Li HZ,Sun WX,Cheng FM,et al. Cigarette smoking status and smoking cessation counseling of Chinese physicians in Wuhan,Hubei province[J]. Asia Pac J Public Health, 2008,20(3):183-192. |
| [18] Jiang Y,Ong MK,Tong EK,et al. Chinese physicians and their smoking knowledge,attitudes,and practices[J]. Am J Prev Med,2007,33(1):15-22. |
| [19] López-De-Munain J, Torcal J, López V,et al. Prevention in routine general practice:activity patterns and potential promoting factors[J]. Prev Med,2001,32(1) :13-22. |
| [20] Polyzos A, Gennatas C,Veslemes M, et al. The smoking-cessation promotion practices of physician smokers in Greece[J]. J Cancer Educ,1995,10(2):78-81. |