 2014, Vol. 35
2014, Vol. 35文章信息
- 李亚绒, 刘小乖, 雷玲霞, 贺方智, 李瑞娜, 彭晓康, 张晓芳, 刘莹, 习艳丽, 黄河清, 王增国. 2014.
- Li Yarong, Liu Xiaoguai, Lei Lingxia, He Fangzhi, Li Ruina, Peng Xiaokang, Zhang Xiaofang, Liu Ying, Xi Yanli, Huang Heqing, Wang Zengguo. 2014.
- 百日咳感染的家庭聚集性特征分析
- Recognizing the vaccination strategy of pertussis according to the family aggregation feature of transmission
- 中华流行病学杂志, 2014, 35(8): 953-955
- Chinese Journal of Epidemiology, 2014, 35(8): 953-955
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2014.08.017
-
文章历史
- 投稿日期:2013-12-27


2. 西安市疾病预防控制中心

 , Liu Xiaoguai1, Lei Lingxia1, He Fangzhi1, Li Ruina1, Peng Xiaokang1, Zhang Xiaofang1, Liu Ying2, Xi Yanli2, Huang Heqing2, Wang Zengguo2
, Liu Xiaoguai1, Lei Lingxia1, He Fangzhi1, Li Ruina1, Peng Xiaokang1, Zhang Xiaofang1, Liu Ying2, Xi Yanli2, Huang Heqing2, Wang Zengguo2
2 Xi'an Center for Disease Control and Prevention
百日咳是一种疫苗可预防的传染病,我国用于 预防百日咳的疫苗包括全细胞百白破疫苗(DTwP) 和/或无细胞百白破疫苗(DTaP),接种程序为基础免 疫(3,4,5月龄各一剂次)和强化免疫(18~24月龄 一剂次)。我国自20世纪80年代将百日咳疫苗纳入 常规免疫以来,其疫苗覆盖率已逐渐达到较高水平, 同时百日咳报告发病率迅速下降并长期保持在1/10 万以下。但我国个别地区也偶有高发病的报道[1]。自一些疫苗高覆盖率国家所报道的“百日咳重现”现 象发生以来[2, 3],近年来我国学者也对该病进行了大 量研究,并认为我国的百日咳发病被严重低估[4, 5, 6, 7]。 为此本研究在对西安市儿童医院就诊的可疑百日咳 患者进行实验室确证的基础上,描述病例的年龄分 布并追踪传染源,以了解当前百日咳发病及传播特 征,为制定有针对性的预防策略提供科学依据。 对象与方法
1. 病例及其来源:儿童及婴幼儿病例来自2012 年1月至2013年8月于西安市儿童医院就诊的百日 咳可疑病例[其定义参考我国现行百日咳诊断标准 (WS274-2007)];流行病学相关病例(密切接触者 病例)为入组百日咳儿童及婴幼儿实验室确诊病例 的密切接触者中20d内具有咳嗽症状者。百日咳实 验室诊断病例定义为百日咳鲍特菌分离培养阳性 和/或核酸检测阳性和/或PT-IgG≥100IU/ml的临床 可疑病例或流行病学相关病例。
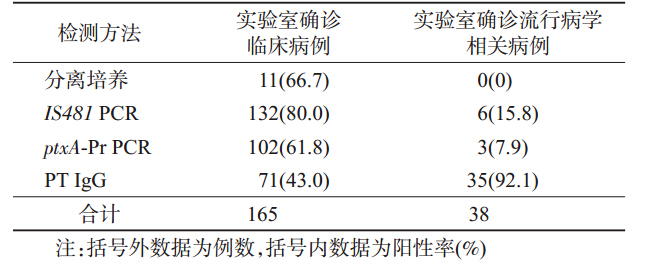
2. 实验室诊断:根据知情自愿原则,采集本研究 纳入的就诊病例及其流行病学相关病例双份鼻咽拭 子标本(NPS)和血清标本,参照文献方法[7],分别用 于百日咳鲍特菌分离培养,IS481和ptxA-Pr基因特 异性PCR检测以及单份血清的PT-IgG检测。
3. 统计学分析:使用Excel2007软件建立数据 库,并完成图表制作。 结 果
1. 一般情况:研究期间在西安市儿童医院共纳 入百日咳临床可疑病例254例(2012年178例、2013 年76例),所有病例均采集标本进行实验室检测, 实验室确诊病例165例(2012年121例、2013年44 例)。其中28例曾接种1~3剂次DTaP,3例曾接种 4剂次DTaP,11例接种史不详,其余未接种百日咳 疫苗(表 1)。对165例实验室确诊病例的密切接触 者调查发现,61例的密切接触者供述无咳嗽症状或 者不详,在其余105例的密切接触者中,均发现流 行病学相关病例。采集流行病学相关病例标本54 人份进行实验室检测,其中实验室确诊病例38例 (表 2)。

2. 实验室确诊病例的年龄分布:临床诊断病例 经实验室确诊的165例和流行病学相关病例经实验 室确诊的38例均按照<1、1~、4~、7~、13~及≥ 20岁分组,其实验室确诊病例的年龄分布见表 3。

3. 流行病学相关病例分析:54例流行病学相关病例经实验室确诊38例,均为患儿家庭成员。其中 33例在患儿发病前有咳嗽症状,5例为患儿发病后 有咳嗽症状。每代流行病学相关病例其发病间隔时 间为4~13(M=8)d,因此结合各病例每起聚集性发 病的间隔日期(潜伏期),判定实验室确诊的临床病 例中来自传染源共计33例,后续病例共计5例。 其中33例的直接传染源均为患者家属(母亲占 59.4%,父亲占18.8%,其他亲属占21.8%)。38例实 验室确诊的流行病学相关病例中,多数无百日咳典 型症状(痉挛性咳嗽6例,间歇性咳嗽及咽炎喘息32 例),且无一例被诊断为百日咳(未就诊27例,诊断 感冒11例)。
4. 百日咳传播模式:根据每起家庭聚集性发病 病例间潜伏期计算,推测其传播模式为成年人-婴幼 儿(≤3岁)30起,儿童(4~12岁)-婴幼儿2起以及 儿童-成年人、婴幼儿-成年人和成年人-成年人。 讨 论
目前“百日咳重现”发生于全球多个疫苗高覆盖 率国家和一些发展中国家[3, 8],是唯一发病呈上升趋 势的疫苗可预防疾病[9]。在百日咳新的高发病率情况下,其流行特征较疫苗大规模接种前发生了诸多 变化,如<1岁婴儿、青少年及成年人发病较多,不 同于过去在儿童间传播的特征,而呈现家庭聚集性 传播[10]。
当前我国关于百日咳发病特征尤其是传播特征 的报道较少。2010年天津市曾发生百日咳暴发并开 展了社区监测,在我国首次报道了百日咳家庭聚集性 发病的现象[1]。血清流行病学调查认为我国百日咳 发病被严重低估,由于临床忽视和较少开展实验室辅 助诊断,报告的病例数依然较少。2012年全国报告 百日咳发病仅2183例[11],而90%的病例为具有典型 临床症状的婴幼儿[12]。本研究中<1岁的婴儿病例 占实验室确诊病例的构成比最高,而其传染源则主要 来自成年人,尤其是其保育者(父母及其他亲属)。国 外报道百日咳死亡病例主要发生在<1岁婴儿[9]。
本研究<1岁病例均未接种或未完成百白破疫 苗接种。而作为传染源的成年人却可能因为感染后 发病较轻,临床症状不典型被误诊或未引起注意[4], 如本研究83.3%的成年病例仅表现为持续性咳嗽, 并无典型的百日咳症状,而回顾性调查发现,无一诊 断为百日咳。成年人作为百日咳的传染源,虽然其 临床症状较轻,但流行病学意义重大。因此疫苗预 防接种可能是相对有效的预防措施。虽然当前一些 研究认为,接种无细胞百白破疫苗可能效果不佳,但 依然是预防控制百日咳最有效途径[9]。
国外报道一致认为,母亲是婴儿患百日咳最主 要的传染源,由此提出针对妊娠晚期孕妇应产前接 种疫苗,但该方案尚存有争议[13]。在我国奶奶或外 婆常作为婴儿保育者,因此在传染源中其角色不可 忽视。目前国外推荐一种百日咳预防接种“蚕茧策 略”,即对围产期母亲及其家庭成员和新生儿密切接 触者接种疫苗[14],或如美国推荐的给予孕妇产前或 产后以及新生儿密切接触者包括其他家庭成员、卫 生保健人员等加强免疫[15],可能对我国百日咳预防 具有一定的借鉴意义。
此外,相关研究发现,百白破疫苗免疫或百日咳 自然感染后形成的免疫具有自然消退的特点[2, 16],青 少年在发病年龄分布中依然占有一定的比例[17],而 本研究则未见青少年病例,可能由于病例就医时对 医院选择和病例症状不典型所致,而应采取主动监 测可以准确了解当前百日咳发病人群的特点,并提 供科学的预防控制措施。
| [1] Zhang Y, Huang HT, Liu Y,et al. Incidence surveillance of pertussis based on community and analysis of its transmitted features in Tianjin[J]. Chin J Vacc Immun,2011,17(3):209-211.(in Chinese)张颖,黄海涛,刘勇,等. 天津市社区人群百日咳发病监测及传播特征研究[J]. 中国疫苗和免疫,2011,17(3):209-211. |
| [2] Mooi FR,Na VDM,de Melker HE. Pertussis resurgence:waning immunity and pathogen adaptation - two sides of the same coin[J]. Epidemiol Infect,2013,142(4):685-694. |
| [3] Mattoo S,Cherry JD. Molecular pathogenesis,epidemiology,and clinical manifestations of respiratory infections due to Bordetella pertussis and other Bordetella subspecies[J]. Clin Microbiol Rev,2005,18(2):326-382. |
| [4] Wang CQ, Zhu QR. Seroprevalence of Bordetella pertussis antibody in children and adolescents in China[J]. Pediatr Infect Dis J,2011,30(7):593-596. |
| [5] Wang CQ,Zhu QR. Clinical characteristics of pertussis and no-pertussis in children and adolescents with chronic cough[J]. J Clin Pediatr,2010,28(6):542-544.(in Chinese)王传清,朱启镕. 百日咳与非百日咳迁延性慢性咳嗽儿童及青少年临床特征分析[J]. 临床儿科杂志,2010,28(6):542-544. |
| [6] Wang ZG, Li YR, Hou TJ, et al. Appearance of macrolide- resistant Bordetella pertussis strains in China[J]. Antimicrob Agents Chemother,2013,57(10):5193-5194. |
| [7] Wang ZG,Yang Y,Liu Y,et al. Comparative studies on different methods for laboratory diagnosis of pertussis[J]. Chin J Epidemiol,2013,34(10):1010-1012.(in Chinese)王增国,杨杨,刘莹,等. 百日咳实验室诊断方法的应用分析与比较[J]. 中华流行病学杂志,2013,34(10):1010-1012. |
| [8] Sadoh AE,Oladokun RE. Re-emergence of diphtheria and pertussis:implications for Nigeria[J]. Vaccine,2012,30(50):7221-7228. |
| [9] Tiwari T,Murphy TV,Moran J. Recommended antimicrobial agents for the treatment and postexposure prophylaxis of pertussis:2005 CDC Guidelines[J]. MMWR Recomm Rep,2005,54(RR-14):1-16. |
| [10] Huang HT,Li YC,Liu Y,et al. Transmitted features of family aggregation on pertussis in Tianjin[J]. Chin J Epidemiol,2011,32(8):843-844.(in Chinese)黄海涛,李永成,刘勇,等. 天津市百日咳家庭聚集性发病的传播特征研究[J]. 中华流行病学杂志,2011,32(8):843-844. |
| [11] WHO. Vaccine preventable diseases:monitoring system[DB/OL]. 2013 Global Summary [cited 2013 Oct. 1]. http://apps.who.int/immunization_monitoring/globalsummary/countries?countrycriteria% 5Bcountry%5D%5B%5D=CHN&commit=OK. |
| [12] Zhang Q, Zheng H, Liu M,et al. The seroepidemiology of immunoglobulin G antibodies against pertussis toxin in China:a cross sectional study[J]. BMC Infect Dis,2012,12:138. |
| [13] Halperin BA,Halperin SA. The reemergence of pertussis and infant deaths:is it time to immunize pregnant women?[J]. Future Microbiol,2011,6(4):367-369. |
| [14] Forsyth KD,Wirsing von Konig CH,Tan T,et al. Prevention of pertussis:recommendations derived from the second Global Pertussis Initiative roundtable meeting[J]. Vaccine,2007,25(14):2634-2642. |
| [15] Murphy TV,Slade BA,Broder KR,et al. Prevention of pertussis,tetanus,and diphtheria among pregnant and postpartum women and their infants recommendations of the Advisory Committee on Immunization Practices (ACIP)[J]. MMWR Recomm Rep,2008,57(RR-4):1-51. |
| [16] Klein NP,Bartlett J,Rowhani-Rahbar A,et al. Waning protection after fifth dose of acellular pertussis vaccine in children[J]. N Engl J Med,2012,367(11):1012-1019. |
| [17] Chiappini E,Stival A,Galli L,et al. Pertussis re-emergence in the post-vaccination era[J]. BMC Infect Dis,2013,13:151. |