 2018, Vol. 29
2018, Vol. 29 


 ,
Zhaochao Xub
,
Zhaochao Xub
b Key Laboratory of Separation Science for Analytical Chemistry, Dalian Institute of Chemical Physics, Chinese Academy of Sciences, Dalian 116023, China;
c University of Chinese Academy of Sciences, Beijing 100039, China
Breast cancer (BC) is the most common diagnosed cancer and the leading cause of death in females worldwide, representing about 25% of all cancer cases and 15% of all cancer deaths [1]. Thanks to early detection and improved treatment, the BC death rates have been stable or decreasing [2]. Over the past decades, great progress has been achieved in medical imageology, which benefit the early diagnosis of BC. Based on the diagnostic information (including the stage of diagnosis, the size and location of the tumor, and tumor characteristics), individual therapeutic regimen has been chosen. Although the traditional anatomical imaging such as computed X-ray tomography (CT), magnetic resonance imaging (MRI), and ultrasound (US) still account for the main part of medical imageology, the rapidly developing field of molecular imaging (MI) promises more precise molecular and physiological information [3]. These advantages greatly improve our ability to fight BC.
MI is defined as the visualization, characterization, and measurement of biological processes at the molecular and cellular levels in humans and other living systems. Currently, only several MI techniques are applied in BC clinic, including positron emission tomography (PET), single photon emission CT (SPECT), MRI, and magnetic resonance spectroscopy (MRS) [4]. Besides, developments of optical molecular imaging also show potential in clinical applications. Compared to the former techniques, the optical molecular imaging have the superiorities in resolution, selectivity, sensitivity, specificity, higher near infrared fluorescent penetration ability, brighter imaging signal and the lower price [5]. Therefore, the optical imaging technology has opened a new era for the further development of early diagnosis and surgical treatment of BC in clinical. In this review, we attempt to summarize various fluorescent probes associated with BC in recent years and analyzed their advantages and limitations.
2. Overview of BCBC develops from the abnormal breast cells which multiply to be the malignancy. The prevalence, incidence and the mortality rates of BC are still raising, predominantly from the unclear malignancy pathogenesis. It accounts for 16% of all female cancers, and 18.2% of cancer deaths worldwide died of BC. There are some risk factors which can develop BC including: age, obesity, lack of exercise, alcohol consumption, the history of the reproduction and menstruation, benign breast lumps, a history of BC, radiation exposure, hormonal and genetics [6]. Otherwise, Brophy found that certain jobs can increase the high risk of developing BC such as plastics manufacturing jobs, food canning, farming, bars-gambling and metal working [7]. Breast cancer is a heterogeneous disease. BC has multiple different subtypes on the histological, molecular level. On account of the gene expression profiling, the molecular level has been classified into six distinct subtypes include Luminal A, Luminal B, HER-2-enriched, basal-like, claudin-low BC and normal breast-like group [8, 9]. The 12th St Gallen International Breast Cancer Conference (2011) Expert Panel has proposed that using immunohistochemical staining results of ER, PR/overexpression and/or amplification, HER-2/neu oncogene, and Ki- 67-labelling index and/or histological grade as a differentiation of the clinical subtypes [10]. In addition to the classical and accepted by clinical subtypes at the genomic and transcriptomic levels, the proteomic has been the novel research domain. Proteomic maps of BC subtypes demonstrated that the high quantification accuracy for the BC was possible [11]. Based on the above clinical subtypes, the treatment method of BC is more likely to be targeted to the individual: preoperative or neoadjuvant chemotherapy (NACT), neoadjuvant endocrine therapy, and targeted drug therapy. However, the accurate early diagnosis and treatment of BC are still very challenging.
3. Fluorescent probes for imaging BCFluorescence imaging offers an innovative way to recognize BC cells, image in vivo animal models, monitor the effects of antitumor drugs, and guide the surgery in the breast tumor model with high sensitivity and specificity. The key of fluorescence imaging is the construction of fluorescent probe which is composed of two parts, recognition groups to recognize cancer cells and fluorophores to signal the recognition events.
So far, some fluorescent dyes, such as indocyanine green (ICG), methylene blue and 5-aminolevulinic acid (5-ALA), have been approved to be applied in clinical by FDA. Although ICG has been widely used in sentinel lymph node mapping [12], the light stability is still unsatisfied. Besides, some other novel fluorescent dyes are under the clinical trial phase.
In comparison to fluorophores, recognition groups for cancer are much more important to ensure accuracy. Recognition groups specifically bind the over-expressed biomarkers in cancer cells. Compared with the normal breast tissue, αvβ3 integrin, matrix metalloproteinase, cathepsins, fibrin-fibronectin complexes, folate receptor, estrogen receptor, progesterone receptor, human epidermal growth factor receptor 2, epidermal growth factor receptor, vascular endothelial growth factor, insulin-like growth factor receptor, tissue polypeptide specific antigen etc., are uniquely overexpressed in BC tissue. Then, fluorescent probes for BC were designed on the base of recognizing these biomarkers.
3.1. The αvβ3 integrin targeted probesIntegrins are a family of cell surface proteins involved in cell adhesion. Since tumor cells are characterized by migration, invasion and metastasis, the integrins of tumor growth and metastasis are obvious [13, 14]. Among them, αvβ3 is the most important factor involved in the angiogenesis and metastasis in many tumors (such as M21 melanoma, U87MG brain glioblastoma, and BC). Compared to normal tissues, αvβ3 is over-expressed in tumor tissues. In BC, the over-expressed αvβ3 integrin are confirmed to participate in the angiogenesis and promotes the dissolution of extracellular matrix, which lead to tumor invasion and metastasis [15].
RGD are well-known motif to specific bind the αvβ3 integrin which mediates the interactions among cells (Fig. 1) [16]. The affinity of RGD peptides to αvβ3 integrin are affected by the physical and chemical properties, surface charge distribution and the steric conformation of the peptide. Through cyclization, multimerization, glycosylation, polyethylene glycol-modified, bifunctional chelating agent and double target modification, the targeting performance of the RGD peptide are improved. Compared to the linear RGD, those with the highly susceptible to chemical degradation, cyclic RGD (cRGD) peptides showed better properties in conformational stability and tumor-targeting [17].

|
Download:
|
| Fig. 1. Chemical structure of RGD peptides targeted probes. (a) Diagram of the combination of RGD and αvβ3. Reproduced with permission [16]. Copyright 2002, Science. (b) Pattern diagram of the RGD fluorescent probe. Reproduced with permission [24]. Copyright 2002, Cancer Research. | |
{kind=link}
Besides, radiolabelling also is introduced in RGD modification. Jacobson [18] labeled four cyclic RGD peptides with 89Zr all or none PEG functional groups, using the Micro-PET imaging. As a consequence, the 89Zr radiolabeled peptides provided high-quality and high resolution micro-PET images in BC. Chen et al. [19] labeled cyclic RGD peptide c (RGDyK) with 125I, 18F and 64Cu in murine orthotopic MDAMB-435 human BC model. 18F-FB-RGD and 64Cu-DOTA-RGD were demonstrated to be suitable for PET imaging of αvβ3 integrin expression in BC. Zhou [20] synthesized 99mTc-labeled cyclic RGD dimmer to image the Integrin αvβ3-positive tumors.
Although the radionuclide has made great achievements in molecular imaging, its bad biological security and expensive price restrict their application. Therefore, the researchers pay attention to the development of the optical fluorescent dyes. Liu [21] designed mPEG-PLGA-PLL nanoparticles functionalized with cRGD and mitoxantrone (DHAQ) or rhodamine B (Rb). Quantum dots (QD) coated with the specific amphiphiles RGD-C18 and 2-(p-isothiocyanatobenzyl)-1, 4, 7-triazacyclononane-1, 4, 7-triacetic acid [NOTA]-C18 successfully imaged the integrin αvβ3 in subcutaneous U87MG glioblastoma and MCF-7 cells [22]. In another study, cRGD peptide and a near infrared (NIR) fluorescent dye (MPA) were used to bind gold nanoclusters (AuNCs). The specific fluorescent probe Au–cRGD–MPA was successfully demonstrated to image over-expressed integrin-αvβ3 in the MDA-MB-231(BC cell lines) [23].
Near infrared fluorescent dyes labeled with RGD peptide have good applications in BC imaging for their low background signals and deep tissue penetration. Chen et al. [24] (Fig. 1) labeled RGD peptide with the dye Cy5.5 to construct near infrared fluorescent probe RGD-Cy5.5 for a highly sensitive and semiquantitative imaging of tumors in subcutaneous U87MG glioblastoma xenograft. Moreover, Lee [25] developed a RGD-mediated near-infrared pH-activatable fluorescent probe. When pH was over 6, the probe keptin darkstate, butonce the pH was lessthan 5 inlysosomes, the probe was activated to fluoresce. Fluorescent probes based on the RGD-αvβ3 integrin provide a reliable way for tumor imaging and therapy.
3.2. Matrix metalloproteinase and cathepsins targeted probesProteases also named proteolytic enzyme which catalyze hydrolysis of the peptide bond in proteins. A great variety of proteases include serine proteinase, cysteine proteinase, aspartic proteinase, threonine protease and metalloproteinase. Among them, matrix metalloproteinase (MMPs) and cathepsin are highly expressed in various cancers, such as colon and BC [26-28]. The human Matrix metalloproteinase family belongs to zinc-dependent endopeptidases which complexes zinc ion as the active-sites. Among them, the main MMPs associated with BC include MMP-1, MMP-2, MMP-9, MMP-11 and MMP-13 [29]. Numerous studies show that the over-expressed MMPs are involved in the invasion and metastasis in BC through the degradation of the tumor extracelluar matrix, promoting the secretion of growth factor and angiogenesis. The activation of other proteases inducing the immune tolerance of the tumor cell, regulating the adhesion between the tumor cells [30]. Among Cathepsins families, cathepsin B from the cysteine proteases and cathepsin D from the aspartic proteases are highly expressed in BC [31]. High expression of cathepsin B and cathepsin D are linked to the degradation of the tumor extracelluar matrix compents, such as colleagen, laminin, elastin and fibronectin [32], which are demonstrated to be associated with the tumor growth, invasion, metastasis and poor differentiation in BC [33].
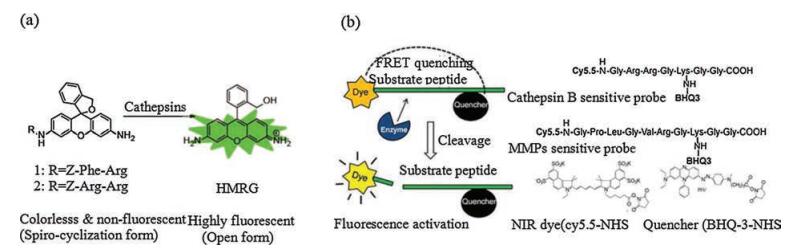
Then, fluorescent probes to identify BC cells specifically were developed on the basis of recognizing these two biomarkers. Nonluminous enzyme-sensing imaging probes including the sequence which can be identified and cleavged by the MMPs and cathepsins. Once the sequence was cleavged, the fluorescent and quenching groups was separated and the fluorescence was recovered. Yasuteru Urano [34] designed an "OFF-ON" fluorescent probe for the γ-glutamy-ltransferase (GGT) which has highly expression in some tumor tissue (Fig. 2). In addition, they used the probe for the local spray imaging. The results showed that the fluorescent probe displayed the specific recognition on tumor tissue. Shortly afterwards, the team also reported an activatable HMRG-based fluorescent probe targeting cathepsins. It could detect the tiny tumors of intraperitoneally disseminated tumors in model mice [32]. Cathepsin B-sensitive (Gly-Arg-Arg-Gly-Lys-GlyGly) and MMPs-sensitive (Gly-Pro-Leu-Gly-Met-Arg-Gly-Leu-GlyLys) substrate peptide conjugated with NIR fluorochrome (Cy5.5) and dark quencher (BHQ-3) were developed lately. When the fluorescent probes located into the tumor region, the fluorescence would be displayed to map the tumor accurately (Fig. 2) [33].

|
Download:
|
| Fig. 2. Pattern diagram of the mechanism of the target Cathepsin B and MMP fluorescent probe. (a) Chemical structures of novel cathepsin probes. Reproduced with permission [32]. Copyright 2014, Bioconjugate Chemistry. (b) NIRF recovery of the cathepsin B and MMP probes by target enzyme and structural designs of cathepsin B probe and MMP sensitive probe. Reproduced with permission [33]. Copyright 2011, Theranostics. | |
{kind=link}
In addition to accurately recognizing the BC cells, fluorescent probes can also be used to identify the tumor margin in the BC surgery. Chi [35] developed a MMPS-activatable near-infrared fluorescent probe MMPSense 750 FAST; Pan [27] constructed a fluorescentnanoprobe, DNA molecular beacons(MBs) labeled with Alexa Fluor 405 and Cy5; MMP-sensitive peptides tagged with FITC and rhodamine B (RhB) were linked to the surface of gold nanoparticles (AuNPs) to act as porbes. Two real-time protease-activatable NIR fluorescent probes ProSense680 and ProSense750 were synthesized [36]. A cathepsin-targeted substrate probe 6QCNIR has also been reported [37]. All of these fluorescent probes were used to precisely distinguish BC margins and guide the tumor resection in the syngeneic rat model of primary BC. Ferber et al. [38] designed two polymeric systems consisting self-quenched-Cy5 (SQ-Cy5) as a near-infrared fluorescent (NIRF) probe. Anticancer agent paclitaxel (PTX) binding to N-(2-hydroxypropyl) methacrylamide (HPMA) copolymer through a Gly-pheleu-Gly (GFLG) was developed, which was cleaved by cathepsin B (HPMA copolymer-SQ-Cy5 and HPMA copolymer-PTX) for the theranostics (therapy and diagnostics) by the real time non-invasive intravital orthotopic monitoring of drug release in BC.
3.3. Fibrin-fibronectin complexes targeted probesFibronectin is one of the extracellular matrix (ECM) components of solid tumors. Tumor cells secrete vascular permeability factor such as vascular endothelial growth factor (VEGF).Therefore, it displays the ability of hyperpermeable to fibronectin and plasma proteins [39] By combination of the extravasated fibronectin and plasma proteins, the meshwork of clotted plasma proteins was formed which played an essential role in tumor invasion, progression and metastasis [40]. Normal breast tissues lack CGLIIQKNEC (CLT1) and CNAGESSKNC (CLT2), CREKA (Cys-Arg-Glu-Lys-Ala) peptide [39, 41, 42]. Pilch et al. [39] labeled CLT1 and CLT2 with fluorescein; Simberg [41] decorated CREKA peptide with superparamagnetic, amino dextran-coated iron oxide (SPIO) and cyanine 7; Tan et al. [43] synthesized the CLT1 peptide-targeted nanoglobular Gd-DOTA monoamide. Likewise, all of above probes were injected in the MDA-MB-435 human BC xenograft model, and all displayed the highly specificity to recognize BC.
The tumor homing peptide targeting fibrin-fibronectin complexes were designed as fluorescent probes and used for cancer therapeutics as well as drug delivery. The conjugation of tumor homing PEGylated CREKA peptide to DIM-P loaded nano-particles (NCs-D) can be used in theranostic tumor homing drug delivery [44]. CREKA peptide conjugated to paclitaxel-albumin nanoparticle accumulated in breast tumor blood vessels as a promising method for the target therapy [42].
3.4. Folate receptor targeted probesFolic acid (FA) is an essential vitamin B group in the body, mainly participating in DNA synthesis, DNA configuration, integrity maintenance, gene expression, DNA methylation and cell proliferation of human body. The FA pinch may lead to tumorigenesis [45].
In vivo, the transporting pathway of FA mainly relies on the folate receptor (FR). FR is a glycosylphosphatidylinositol (GPI) – anchoring membrane glycoprotein which can mediate extracellular folic acid into the cell [46]. Currently, four isoforms of FR have been identified including FRα, FRβ, FRγ and FRδ. Among them, FRα and FRβ have higher affinity to FA [47]. FR is over-expressed in various types of human carcinomas, such as breast, ovarian, cervical, colorectal, lung cancer, compared to normal tissue [48]. Then, FA labeled with organic fluorescent dyes, dye doped nanoparticles, quantum dots, magnetic nanoparticles, were designed to target FR to achieve tumor imaging, anticancer drugs delivering and surgical resection assistance.
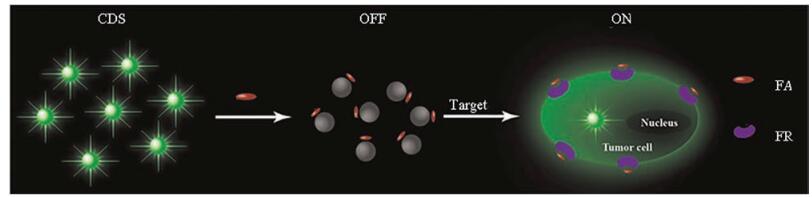
Liu et al. [49] synthesized a novel turn-on fluorescence probe (FA-CDs) via poly aclylate sodium (PAAS, a passivation agent)- prepared CDS binding to the folate for imaging cancer cells (Fig. 3). Feng et al. [50] used folate to modify quantum dots (QDs) loaded with two copolymers of poly (lactide)-vitamin E TPGS (PLA-TPGS) and vitamin E TPGS-carboxyl (TPGS-COOH). The probe displayed a brighter fluorescence in MCF-7 BC cells.

|
Download:
|
| Fig. 3. Scheme illustration of the designed fluorescence turn-on probe for imaging cancer cells overexpressed FR. Reproduced with permission [49]. Copyright 2015, Biosensors and Bioelectronics. | |
{kind=link}
Besides recognize BC cells, fluorescent probes labeled with folic acid can also be used to deliver breast anticancer drugs. For example, Wang et al. [51] conjugated folate with micellar PTX and labeled complex with FITC fluorescent dye. The probe was used to study the transfer of anticancer drugs and multidrug resistance. A pH-sensitive fluorescent probe functionalized with folic acid and encapsulated ZnO hollow-nanocarriers with paclitaxel (PAC) was synthesized. When the probe was accumulated in BC cells, the fluorescence would switch from blue to green and get 10 times increase in fluorescent intensity. The fluorescent probes improved the targeting recognition of BC, and enhanced the effectiveness of anticancer drug delivery [52]. In this study, Silica was encapsulated on the Fe3O4 nanoparticle surfaces. Thereafter, Notch-1 shRNA and co-polymer of PEI-FA conjugated the nanoparticles to synthesize magnetic and fluorescent core/shell nanoparticles. This fluorescent probe decreased the expression of Notch-1 effectively and led the death of MDA-MB-231 cancer cells. The researchers also found that the probe was expected to become a new strategy for the imaging diagnosis and targeted gene therapy for BC [53].
3.5. Hormone receptors targeted probesNumerous studies have shown that 70% patients of BC have the positive hormone receptors, the estrogen receptor (ER) and the progesterone receptor (PR) [54]. For cancerization, ER-positive with or without PR-positive BC are sensitive to the endocrine therapy such as tamoxifen or aromatase inhibitors. Hence, for patients of different types, cancer cell differentiation degree is higher while the degree of malignancy is lower. ER is a member of the nuclear hormone family and a ligand-dependent transcription factor [55], including ER α and ER β, playing a critical role in the breast oncogenesis [56]. PR is the final product of estrogen. Its synthesis and concentration were regulated by estrogen.
Currently, the status of ER and PR are measured by in vitro immunohistochemistry assays of biopsy samples. At present, although there are very few literature reports on the fluorescent probes targeting hormone receptors, these probes have showed a good BC imaging ability. Sukerkar et al. [57] used a proGlo probe to target PR (+) BC cells. Organic fluorescent material tetramethylr-hodamine (TMR) assembled nanoparticles to diagnose ER expression quantitatively. Moreover, in comparison with IHC-DAB and general organic fluorescent QDs, the probe displayed higher signal intensity and broad dynamic detection range of ER expression levels [55]. Besides, a novel NIR fluorescent probe has been reported to measure the ER levels in vivo. Through an ester formation, 17-β estradiol was tagged with a cyanine dye. It showed that the NIRD1 conjugate (NIRDC1) displayed a highly quantum yield and hydrophilicity in comparison with ICG. Notably, the fluorescent probe had the ability of early diagnosis of BC [58].
3.6. Human epidermal growth factor receptor 2 (HER-2) targeted probesThe HER family consists of HER-1/EGFR (epidermal growth factor receptor)/c-erbB1, HER-2/c-erbB2, HER-3/c-erbB3 and HER- 4/c-erbB4. Among them, HER-2 is the most important member, which is also known as HER-2neu/ErbB2 or c-erbB2 [59]. HER-2 locates on the long arm of seventeenth chromosome which is a transmembrane protein with tyro-sine kinase activity composed by three domains: extracellular, transmembrane, and intracellular tyrosine kinase. Over-expressed HER-2 has been found in numerous cancers include ovarian, stomach, kidney, colon, prostate, urinary, breast and so on [60]. Over-expressed HER-2 exist in twenty to twenty-five percent of BC which not only promote the mitosis of cancer cells, inhibit the apoptosis, accelerate the tumor angiogenesis, but also be associated with the aggressiveness and poor prognosis [61]. Currently, HER-2 has been a hot target in the molecular imaging. The fluorescent probes detect the over-expressed HER-2 in BC cells, and further act as a drug delivery system for molecular therapies in BC.
As an example, three different types of HER2-specific affibody molecules (monomer ZHER2:342, dimer (ZHER2:477)2, and albumin-binding domain (ABD)-fused (ZHER2:342)2) were labeled with (AlexaFluor750) dye. By contrast, the ABD-(ZHER2:342)2 conjugate showed more clear tumor accumulation and clearance. Then the results suggest that the specific near-infrared probe can be usedasauniquenon-invasive means in molecular imaging of HER-2- positive BC [62]. Soon after, by NIR optical imaging, the same team used the probe ABD-(ZHER2:342)2-AlexaFluor750 to noninvasively monitor HER2 expression levels in vivo [63].
In addition to the affibody molecules, trastuzumab (Herceptin), humanized monoclonal antibody directed against the HER-2 receptor, modified chitosan-doxorubin conjugate (CS-DOX-mAb) in targeted drug delivery. Through the contrast, there is a higher rate of cell uptake [64]. Gee et al. [65] also reported a fluorescent probe derived from trastuzumab with NIR fluorescent dyes (cyanine 5.5 or AF750). The fluorescent probe displayed a strong binding capacity and high recognition ability. Even during the therapy, the probe also can evaluate the therapeutic susceptibility and drug dosing. In another study, two activatable fluorescent probes, including panitumumab (Pan) labeled with AlexaFluor680 (Alexa680) and trastuzumab (Tra) labeled with indocyanine green (ICG), respectively, was used to monitor the expression of EGFR, HER-2 in BC cells [66].
The level of HER-2 indicates the treatment effect and the risk of recurrence. At present, the clinical methods of testing HER-2 in BC include immunohisto-chemistry and fluorescence in situ hybridization (FISH) through the BC tissue by biopsy and surgical excision. But the problem is that these methods are unable to achieve the real-time and accurate assessment to the patients' HER-2 status. In 2000 years, FDA approved serum HER-2 ECD in BC as the application of monitoring the efficacy and long-term followup. However, in the clinic, only the method of ELISA can detect serum HER-2 ECD, because of many confounding factors in serum. The detection result may cause the existence of false positive or false negative. So it is urgently needed to develop a real-time, accurate and non-invasive technique for the monitoring of serum HER-2 status.
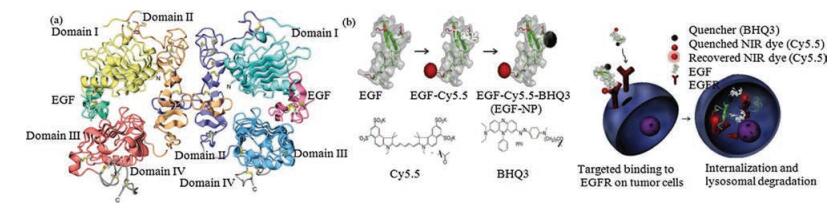
3.7. Epidermal growth factor receptor (EGFR) targeted probesEpidermal growth factor receptor (EGFR, HER1, erb1) (Fig. 4) [67] is a transmembrane glyco-protein belonging to the tyrosine kinase receptor family. When EGFR binds to the corresponding ligands in vivo, the tyrosine kinase would be activated, causing excessive cell division, proliferation and malignant transformation. Hence, the over-expressed EGFR was involved in the cancer cell proliferation, differentiation, angiogenesis, invasion, metastasis, as well as with the poor prognosis and increased metastatic potential. Studies have shown that over-expressed EGFR is associated with numerous types of cancers including the brain, breast, colon, head and neck, ovarian, pancreas, prostate, and skin cancer [68]. So as the same as HER-2, EGFR is widely used in the construction of fluorescent probes to reach the target recognition of BC cells.

|
Download:
|
| Fig. 4. (a) Pattern map of EGF and EGF receptors. Reproduced with permission [67]. Copyright 2002, Cell press. (b) Illustration of chemical reactions used to conjugate Cy5.5 and BHQ3 onto EGF and chemical structures of Cy5.5 and BHQ3. Schematic presentation for activation of EGF-NP. EGF labeled with a NIR fluorophore and a quencher (EGF-NP) binds to EGFR, which leads to cellular internalization and intracellular degradation of EGF-NP in the lysosome. Then, lysosomal degradation of EGF-NP causes separation of the fluorophore from the quencher, allowing recovered fluorescence only within the EGFR-positive cells. Reproduced with permission [71]. Copyright 2013, Biomaterials. | |
{kind=link}
For example, the first FDA-approved anti-EGFR monoclonal antibody Erbitux labeled with Cy5.5 worked as a fluorescent probe. When the probe was injected in MDA-MB-231 (EGFR-overexpressing) and MCF-7 cells (EGFR-low-expressing), it exhibited a 9.32-fold higher affinity, higher uptake rate and maximum intake dose for MDA-MB-231 cells than MCF-7 cells. In the BC xenografts, it also can image EGFR expression status successfully. Additionally, through changing the different fluorescent groups and target element, same model but different fluorescent probes were constructed which can improve the fluorescent signal, achieving a better recognition effect. For example, panitumumab labeled with the NIR fluorescent dye IRDye800 imaged the expression levels of the EGFR in three different BC xenografts [69]. On the surface of the fluorescent naoparticles (FNs) was coupled with the anti-EGFR antibody successfully recognized the MCF-7 BC with good sensitivity [70].
The large size of EGFR antibodies restricted its cell permeability. Hence, in search of a small molecule, EGF (6.2 kDa) labeled with cy5.5 (fluorophore) and BHQ3 (quencher), and EGF-based nanoprobe (EGF-NP) showed a brighter fluorescent intracellular signal in MDA-MB-468 cells (high EGFR-expressing) than in the MDA-MB- 436 cells (low EGFR-expressing) (Fig. 4) [71]. Ac-Cys-ZEGFR: 1907 conjugated with four fluorescent dyes (Cy5.5, Alex-Fluor-680, SRfluor680, IRDye-800CW) to image EGFR in EGFR positive A431 cells and low EGFR expressing MCF7 cells. Among them, Alex680- ZEGFR: 1907 and Cy5.5-ZEGFR: 1907 showed higher tumor-tonormal tissue ratios [72].
3.8. Vascular endothelial growth factor (VEGF) targeted probesOncocytes growth and metastasis depends on the angiogenesis. Among the factors which associated with angiogenesis, vascular endothelial growth factor (VEGF) plays the most important role. VEGF family consists of VEGF A, B, C, D, E and placental growth factor (PIGF) six subtypes. VEGF and VEGFR also involved in the cancer cell proliferation, metastasis due to the mechanism of promoting the endothelial cell mitosis, accelerating the angiogenesis and enhancing the vascular permeability [73]. Currently, using the VEGF and VEGFR as the target for BC imaging has been reported.
In an early study, anti-VEGF antibody bevacizumab and antiHER-2 antibody trastuzumab conjugated with the NIR fluorescent dye IRDye800. Meanwhile, bevacizumab and trastuzumab labeled with 89Zr as the control in the experiments in ovarian cancer cell line A2780 (HER-2-negative, high VEGF expression), SK-BR-3 BC cell (HER-2-overexpressing), KATO-Ⅲ gastric cancer cell lines (HER-2-overexpressing) and ovarian cancer cell line SKOV-3luc1 (HER-2-overexpressing). In a conclusion, all exhibited higher specific, sensitive detection to tumor lesions in vivo and a well guidance in the intraoperative imaging [74].
Additionally, CdTe/ZnS core/shell QDs coupled with antiVEGF165 mAbs and incubated in MCF-7 cells and HEK293 cells. The probe not only detected the human VEGF, but also displayed the antitumor effect through the MTT assays [75]. In another study, through using the optical-only imaging reconstruction method, the probe by VEGF labeling with cyanine 7 was used in BC xenografts and got the noninvasive and deeply seated tumors imaging successfully [76]. Although VEGF is also the specific target for BC, compared to HER-2 and EGFR, its application was still limited.
3.9. Other receptors targeted probesKi67 is a monoclonal antibody against Hodgkin's lymphoma cells which can react with the proliferating cell nuclear antigen in the cell cycle. Some researchers have showed that Ki67 was highexpressed in BC than in the normal breast tissue. Furthermore, over-expressed Ki67 in BC is associated with the pathological grading, tumor cell proliferation, invasive growth, metastasis, and poor prognosis. QD-based double fluorescent dyes simultaneously image the co-expressions of ki67 and HER-2 in BC cells, and to detect the role of Ki67 and HER-2 in BC. As a consequence, Ki67 exhibited the bright red fluorescence in nucleus while HER-2 displayed the green luminance on the cell membrane. Next, the clinical prognosis trials of the both markers in the BC showed that a much more side effect on the prognosis of Ki67 than HER-2 in BC [77].
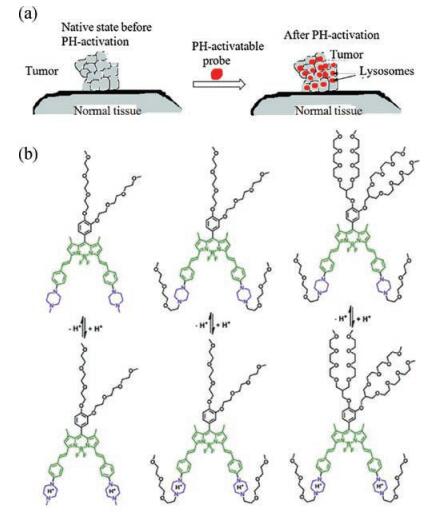
Dysregulated pH includes intracellular pH (pHi) and extracelluar pH (pHe) plays the important roles in tumor cell proliferation and metastasis, so it has become a hot research topic to study the physiological and pathological processes of the cells by the accurate detection of pH. Recently, a new pH sensitive fluorescent probe has been used (Fig. 5). It's in the state of quenching in normal tissues, while in acidic pH, it's in activated state, fluorescent signal got increased. So it can be spatial and temporal monitoring of tumor acidic region [78].

|
Download:
|
| Fig. 5. (a) Selective pH activation of tumor in acidic lysosomal compartments. Reproduced with permission [25]. Copyright 2011, Bioconjugate Chemistry. (b) Chemical structures of near-infrared fluorescent probes and their responses to pH. Reproduced with permission [79]. Copyright 2015, Journal of Materials Chemistry B. | |
{kind=link}
Three acidotropic BODIPY-based near-infrared fluorescent probes A, B, C were synthesized to detect the lysosomal pH. Meanwhile, two cell types include MDA-MB-231 BC cell line and normal endothelial cell line HUVEC-C were incubated with these three NIR probes. At the neutral pH environment, they showed extremely low fluorescence, while at the acidic pH, the low fluorescence would convert to the strong fluorescence due to the intramolecular charge transfer (ICT) and potential photo-induced electron transfer effect (Fig. 5) [79]. In another study, Herceptinbased CypHer5E labeled pH-sensitive near-infrared fluorescent probe (pH-Her) and an always-on fluorescent probe Alexa Fluor 647-Herceptin (Alexa-Her) as the control were used in the HER2- positive (KPL-4) and HER-2-negative (MDA-MB-231) BC cells and carcinoma xenografts. In contrast, the pH-Her probe displayed a higher, faster sensitivity and discovery rate or even the brighter fluorescent signal [80].
Furthermore, three novel analogues of peptide 18 (18-4, 18-9, 18-10) were labeled with FITC, which exhibited the higher affinity and uptake to human BC cell lines: MDA-MB-435, MDA-MB-231, and MCF-7with minimal cellular toxicity and efficient targeting moieties [81]. Moreover, PAR1 is a novel biomarker in HER-2- negative BC patients, which promoted the tumor metastasis as a G protein-coupled receptor. In the study, anti-PAR1 antibody was conjugated with the QDs (anti-PAR1-QDs) for imaging the expression of the PAR1 in BC cells. As the consequence demonstrated that it would be potential as an anticancer drug delivery or even the prognostic biomarker to the BC [61].
3.10. Aptamers as new recognition groups for BCAptamer is one of the most active new targeted molecules in currently research, also known as "chemical antibody". It is a single strain oligonucleotide achieved through a method called systematic evolution of ligands by exponential enrichment (SELEX).Aptamer has the three-dimensional structure and can bind the target molecule with high affinity and specificity. Compared to the antibody, aptamer has many advantages including the strong stability, high affinity, non-immunogenicity, non-toxic, good tissue penetration, modification and extensive target molecules [82]. Therefore aptamer has a considerable prospect in BC molecular diagnosis and biological targeted therapy and so on.
The aptamer (S2.2)-guided Ag-Au nanostructures (aptamer-Ag-Au) have been synthesized. Through the surface-enhanced Raman scattering (SERS) spectra indicated that the nanostructures can target the human BC cells (MCF-7) with high affinity and specificity compared to the HepG2 (human liver cancer cells) and MCF-10A cells (human normal breast epithelial cells). This study also discriminated the MCF-7 cells from MCF-10A cells and HepG2 cells. Except for that, the nanostructures performed near-infrared (NIR) photothermal therapy for MCF-7 BC cells. Hence, the aptamer-Ag-A nanostructures offered a method to recognize, detect and treat the BC cells specifically and sensitively [83].
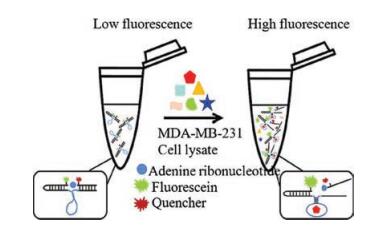
Another study also displayed an RNA-Cleaving Fluorogenic DNAzyme (RFDs) Probe AAI2-5. The probe was synthesized with a fluorescein and a quencher coupled with a RNA unit flanked by adenine ribonucleotide which produced through the Systematic Evolution of Ligands by Exponential enrichment (SELEX) process. AAI2-5 can detect the BC cell line MDA-MB-231 from normal cells as well as other types of tumor cells sensitively and specifically. Furthermore, AAI2-5 responded positively to more than 90% of BC. As the consequence, it showed that the probe AAI2-5 was most likely applied for the diagnosis and treatment of BC in the future (Fig. 6) [84].

|
Download:
|
| Fig. 6. Mechanism of the action of the adapter fluorescent probe. Reproduced with permission [84]. Copyright 2014, Analytical Chemistry. | |
{kind=link}
Moreover, a dual aptamer-modified silica nanoparticle was synthesized to target two types of BC cells: the MUC1 (+) and HER- 2 (+) cell lines simultaneously. Compared with the single aptamer system, the probe displayed a stronger fluorescence. In addition, based on Dual-SiNPs, a more accurate, sensitive detection of BC cells was performed. Therefore, it is expected that the probe will be a noteworthy tool for the diagnosis and prognosis of BC [85].
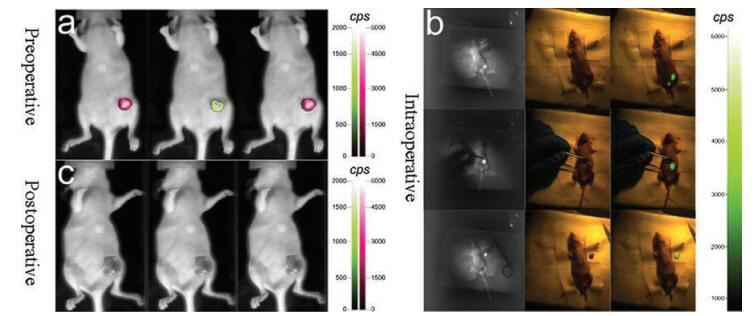
4. Preclinical application of fluorescent probesIn recent years, fluorescence-guided surgery (FGS) is a kind of new medical imaging technique in clinic surgery [86], helping the operators distinguish the accurate margins between the cancer and the adjacent normal tissues to execute the cancer resection in real time intra-operatively [87]. The signal of fluorescent probes is usually measured as a change in fluorescent intensity, fluorescent lifetime, or a shift of fluorescent wavelength [88]. In 2000, Stummer [89] was the first one to report a new technique using 5- ALA fluorescent probe to guide glioblastoma surgical resection of 52 cases in clinic. The fluorescence of 5-ALA has the highest accuracy in judging the boundary of glioblastoma, the sensitivity was 0.89 and the specificity was 0.96. After the operation, 33 cases achieved complete resection of enhancing tumor (CRET) by reviewing the MRI, CRET ratio was 63.5%. Subsequently, in the European countries, FGS has been widely used in the surgical treatment of adult glioblastoma. In 2011, van Dam et al. [90] used fluorescence guided technology for the surgical removal of human ovarian cancer for the first time. Due to the fact that folate receptor is over-expressed in human ovarian cancer, the researchers connected the folic acid with a common green fluorescent dye FITC. The fluorescent probe achieved the selective labeling to the ovarian cancer tissue. Surgeon can identify the cancer tissue and the adjacent healthy tissue in contrast to the bright field and the fluorescent field to achieve the precise resection of ovarian cancer. These achievements could result in a great improvement on patient outcome and reduction of entire healthcare costs. However, some fluorescent probes such as, a MMPS-activatable near-infrared fluorescent probe MMPSense 750 FAST [35]; two real-time protease-activatable NIR fluorescent probes ProSense680 and ProSense750 were synthesized [36], they were used into the intra-operative precisely distinguishing BC margins and guiding the tumor resection in the syngeneic rat model of primary BC. But there is no report on the clinic surgery application of fluorescent probes in BC. Hence, we deem that the FGS will be a major breakthrough in the combination of fluorescent probes and clinic (Fig. 7).

|
Download:
|
| Fig. 7. Detection and resection of breast cancer using FMI-guided surgery. (a) Before surgery, used fluorescence and the bioluminescence images to confirm the probes was specifically targeted the breast cancer. The fluorescence of the MMP-750 probe was labeled in red. The bioluminescence was labeled in green. (b) The FMI-guided BCS system was used to detect the breast tumour margins and remove the whole tumour intra-operatively. In vivo fluorescent images are shown in the first column. Because near-infrared light is not visible, there was no tumourspecific information in colour images in vivo in the second column. The merged in vivo images based on the calculation of the software in our system are shown in the right column. The lower fluorescent spot is urine, and the light was eliminated by wiping. According to the guidance of the fluorescent image, the surgeons could quickly find the location of the orthotropic breast tumour margin, and the orthotropic tumour could be carefully removed during surgery. (c) Fluorescence and bioluminescence images were collected postoperatively to confirm the completeness of the resection. Reproduced with permission [35]. Copyright 2015, Nature. | |
{kind=link}
5. Conclusion and outlook
In this review, we conclude that the fluorescent probes have been used to image BC cell lines and related animal models. Compared with other diagnostic techniques, due to its high selectivity, sensitivity, specificity and signal intensity [91], fluorescent probes can be a diagnostic aid for the early diagnosis of BC. However, the emission wavelength of most fluorescent probes locating in the visible region limits their further application in vivo [92] and breast cancer lacks of pertinent biomarker, there are still many problems to be solved. For instance, in terms of fluorescence-guided surgery (FGS), fluorescent probes in clinical need to have better selectivity, nontoxic or low toxicity, sufficient luminous intensity and light stability. Secondly the fluorescent wavelength must be in the near infrared region, so that it can reduce the background interference, the tissue absorption and increase the penetration depth. However, currently reported fluorescent probes cannot meet the above requirements. The fluorescent probes were only been tested in the BC cell lines and animal models, while in human BC cells and transplantation animal models of BC have not yet been applied. That is to say it lacks of universality. Perhaps, the reported probes only can target on BC cell lines, but lack of specificity for the identification in human BC cells. Therefore, we need the preclinical experiments. At present, there are very few kinds of fluorescent dyes get the FDA certification in the clinic, and because of the poor light stability limit their widely application.
AcknowledgmentsWe thank financial supports from the National Natural Science Foundation of China (Nos. 31370391, 81772812, 21422606, 21402191), Dalian Cultivation Fund for Distinguished Young Scholars (Nos. 2014J11JH130 and 2015J12JH205), and The Foundation of Dalian Science Department (No. 2015E12SF149).
| [1] |
L.A. Torre, F. Bray, R.L. Siegel, et al., Ca Cancer J. Clin. 65 (2015) 87-108. DOI:10.3322/caac.21262 |
| [2] |
M.D. Althuis, J.M. Dozier, W.F. Anderson, S.S. Devesa, L.A. Brinton, Int. J. Epidemiol. 34 (2005) 405-412. DOI:10.1093/ije/dyh414 |
| [3] |
H. Liu, Y. Chen, S. Wu, et al., Nucl. Med. Commun. 37 (2016) 1116-1124. DOI:10.1097/MNM.0000000000000576 |
| [4] |
M.A. Pysz, S.S. Gambhir, J.K. Willmann, Clin. Radiol. 65 (2010) 500-516. DOI:10.1016/j.crad.2010.03.011 |
| [5] |
S. Lee, J. Xie, X.Y. Chen, Chem. Rev. 110 (2010) 3087-3111. DOI:10.1021/cr900361p |
| [6] |
X.R. Yang, J. Chang-Claude, E.L. Goode, F.J. Couch, J. Natl. Cancer I 103 (2011) 250-263. DOI:10.1093/jnci/djq526 |
| [7] |
J.T. Brophy, M.M. Keith, A. Watterson, et al., Environ. Health-Glob. 11 (2012) 87. DOI:10.1186/1476-069X-11-87 |
| [8] |
A. Skibinski, C. Kuperwasser, Oncogene 34 (2015) 5309-5316. DOI:10.1038/onc.2014.475 |
| [9] |
D.C. Koboldt, R.S. Fulton, M.D. McLellan, H. Schmidt, J. Kalicki-Veizer, Nature 490 (2012) 61-70. DOI:10.1038/nature11412 |
| [10] |
A. Goldhirsch, W.C. Wood, A.S. Coates, R.D. Gelber, B. Thurlimann, Ann. Oncol. 22 (2011) 1736-1747. DOI:10.1093/annonc/mdr304 |
| [11] |
S. Tyanova, R. Albrechtsen, P. Kronqvist, et al., Nat. Commun. 7 (2016) 1-11. |
| [12] |
A. Taruttis, V. Ntziachristos, Nat. Photonics 9 (2015) 219-227. DOI:10.1038/nphoton.2015.29 |
| [13] |
J.S. Desgrosellier, D.A. Cheresh, Nat. Rev. Cancer 10 (2010) 890-890. |
| [14] |
R. Rathinam, S.K. Alahari, Cancer Metast. Rev. 29 (2010) 223-237. DOI:10.1007/s10555-010-9211-x |
| [15] |
Y. Zheng, S. Ji, A. Czerwinski, et al., Bioconjugate Chem. 25 (2014) 1925-1941. DOI:10.1021/bc500452y |
| [16] |
J.P. Xiong, T. Stehle, R.G. Zhang, et al., Science 296 (2002) 151-155. DOI:10.1126/science.1069040 |
| [17] |
M. Fani, D. Psimadas, C. Zikos, et al., Anticancer Res. 26 (2006) 431-434. |
| [18] |
O. Jacobson, L. Zhu, G. Niu, et al., Mol. Imaging Biol. 13 (2011) 1224-1233. DOI:10.1007/s11307-010-0458-y |
| [19] |
X.Y. Chen, R. Park, M. Tohme, et al., Bioconjugate Chem. 15 (2004) 41-49. DOI:10.1021/bc0300403 |
| [20] |
Y. Zhou, Y.S. Kim, X. Lu, S. Liu, Bioconjugate Chem. 23 (2012) 586-595. DOI:10.1021/bc200631g |
| [21] |
P.F. Liu, L.B. Qin, Q. Wang, et al., Biomaterials 33 (2012) 6739-6747. DOI:10.1016/j.biomaterials.2012.06.008 |
| [22] |
Y.K. Lee, J.M. Jeong, L. Hoigebazar, et al., J. Nucl. Med. 53 (2012) 1462-1470. DOI:10.2967/jnumed.111.092759 |
| [23] |
H.Y. Chen, M. Zhang, H.B. Yang, et al., Rsc Adv. 4 (2014) 8191-8199. DOI:10.1039/C3RA47453D |
| [24] |
X.Y. Chen, P.S. Conti, R.A. Moats, Cancer Res. 64 (2004) 8009-8014. DOI:10.1158/0008-5472.CAN-04-1956 |
| [25] |
H. Lee, W. Akers, K. Bhushan, et al., Bioconjugate Chem. 22 (2011) 777-784. DOI:10.1021/bc100584d |
| [26] |
T. Yamada, T. Oshima, K. Yoshihara, et al., Anticancer Res. 30 (2010) 2693-2699. |
| [27] |
W. Pan, H.J. Yang, N. Li, L.M. Yang, B. Tang, Chem. Eur. J. 21 (2015) 6070-6073. DOI:10.1002/chem.v21.16 |
| [28] |
B.S. Parker, D.R. Ciocca, B.N. Bidwell, et al., J. Pathol. 214 (2008) 337-346. DOI:10.1002/path.2265 |
| [29] |
A. Merdad, S. Karim, H.J. Schulten, et al., Anticancer Res. 34 (2014) 1355-1366. |
| [30] |
D. Bourboulia, W.G. Stetler-Stevenson, Semin. Cancer Biol. 20 (2010) 161-168. DOI:10.1016/j.semcancer.2010.05.002 |
| [31] |
H.R. Lee, K.C. Choi, Toxicology 304 (2013) 13-20. DOI:10.1016/j.tox.2012.10.012 |
| [32] |
T. Fujii, M. Kamiya, Y. Urano, Bioconjugate Chem. 25 (2014) 1838-1846. DOI:10.1021/bc5003289 |
| [33] |
J.Y. Yhee, S.A. Kim, H. Koo, et al., Theranostics 2 (2012) 179-189. DOI:10.7150/thno.3716 |
| [34] |
Y. Urano, M. Sakabe, N. Kosaka, et al., Sci. Transl. Med. 3 (2011) 110-119. |
| [35] |
C.W. Chi, Q. Zhang, Y.M. Mao, et al., Sci. Rep. 5 (2015) 14197. DOI:10.1038/srep14197 |
| [36] |
J.S.D. Mieog, M. Hutteman, J.R. van der Vorst, P.J.K. Kuppen, Breast Cancer Res. Treat. 128 (2011) 679-689. DOI:10.1007/s10549-010-1130-6 |
| [37] |
L.O. Ofori, N.P. Withana, T.R. Prestwood, M. Verdoes, J.J. Brady, ACS Chem. Biol. 10 (2015) 1977-1988. DOI:10.1021/acschembio.5b00205 |
| [38] |
S. Ferber, H. Baabur-Cohen, R. Blau, et al., Cancer Lett. 352 (2014) 81-89. DOI:10.1016/j.canlet.2014.02.022 |
| [39] |
J. Pilch, D.M. Brown, M. Komatsu, et al., Proc. Natl. Acad. Sci. U. S. A. 103 (2006) 2800-2804. DOI:10.1073/pnas.0511219103 |
| [40] |
N.E. Reticker-Flynn, D.F.B. Malta, M.M. Winslow, J.M. Lamar, M.J. Xu, Nat. Commun. 3 (2013) 1122. |
| [41] |
D. Simberg, T. Duza, J.H. Park, et al., Proc. Natl. Acad. Sci. U. S. A. 104 (2007) 932-936. DOI:10.1073/pnas.0610298104 |
| [42] |
P.P. Karmali, V.R. Kotamraju, M. Kastantin, M. Black, D. Missirlis, Nanomed.-Nanotechnol. 5 (2009) 73-82. DOI:10.1016/j.nano.2008.07.007 |
| [43] |
M.Q. Tan, X.M. Wu, E.K. Jeong, Q.J. Chen, Z.R. Lu, Biomacromolecules 11 (2010) 754-761. DOI:10.1021/bm901352v |
| [44] |
A.R. Patel, M.B. Chougule, E. Lim, et al., Nanomed.-Nanotechnol. 10 (2014) 1053-1063. DOI:10.1016/j.nano.2013.12.002 |
| [45] |
P. Chen, C. Li, X. Li, et al., Br. J. Cancer 110 (2014) 2327-2338. DOI:10.1038/bjc.2014.155 |
| [46] |
M. Bai, D.J. Bornhop, Curr. Med. Chem. 19 (2012) 4742-4758. DOI:10.2174/092986712803341467 |
| [47] |
T. Yang, F.F. Xu, D.J. Fang, Y. Chen, Sci. Rep. UK 5 (2015) 16733. DOI:10.1038/srep16733 |
| [48] |
H. Li, Y. Cheng, Y. Liu, B. Chen, Talanta 158 (2016) 118-124. DOI:10.1016/j.talanta.2016.05.038 |
| [49] |
Q.L. Liu, S.H. Xu, C.X. Niu, et al., Biosens. Bioelectron. 64 (2015) 119-125. DOI:10.1016/j.bios.2014.08.052 |
| [50] |
J. Pan, S.S. Feng, Biomaterials 30 (2009) 1176-1183. DOI:10.1016/j.biomaterials.2008.10.039 |
| [51] |
Y.Z. Wang, L. Yu, L.M. Han, X.Y. Sha, Int. J. Pharm. 337 (2007) 63-73. DOI:10.1016/j.ijpharm.2006.12.033 |
| [52] |
N. Puvvada, S. Rajput, B.N.P. Kumar, et al., Sci. Rep. UK 5 (2015) 11760. DOI:10.1038/srep11760 |
| [53] |
H. Yang, Y. Li, T.T. Li, et al., Sci. Rep. UK 4 (2014) 7072. |
| [54] |
C. Park, K. Park, J. Kim, et al., World J. Surg. Oncol. 14 (2016) 244. DOI:10.1186/s12957-016-0999-x |
| [55] |
K. Gonda, M. Miyashita, M. Watanabe, et al., Biochem. Biophys. Res. Commun. 426 (2012) 409-414. DOI:10.1016/j.bbrc.2012.08.105 |
| [56] |
M. Widschwendter, H. Lichtenberg-Frate, G. Hasenbrink, Br. J. Cancer 101 (2009) 160-165. DOI:10.1038/sj.bjc.6605106 |
| [57] |
P.A. Sukerkar, K.W. MacRenaris, T.J. Meade, J.E. Burdettes, Mol. Pharmaceutics 8 (2011) 1390-1400. DOI:10.1021/mp200219e |
| [58] |
I. Jose, K.D. Deodhar, U.B. Desai, S. Bhattacharjee, J. Fluoresc. 21 (2011) 1171-1177. DOI:10.1007/s10895-010-0795-x |
| [59] |
H. Nitta, B.D. Kelly, C. Allred, et al., Pathol. Int. 66 (2016) 313-324. DOI:10.1111/pin.2016.66.issue-6 |
| [60] |
J. Capala, K. Bouchelouche, Curr. Opin. Oncol. 22 (2010) 559-566. DOI:10.1097/CCO.0b013e32833f8c3a |
| [61] |
K. Gonda, M. Miyashita, H. Higuchi, et al., Sci. Rep. UK 5 (2015) 14322. DOI:10.1038/srep14322 |
| [62] |
S.B. Lee, M. Hassan, R. Fisher, O. Chertov, Clin. Cancer Res. 14 (2008) 3840-3849. DOI:10.1158/1078-0432.CCR-07-4076 |
| [63] |
V. Chernomordik, M. Hassan, S.B. Lee, R. Zielinski, Mol. Imaging 9 (2010) 192-200. |
| [64] |
P. Yousefpour, F. Atyabi, E. Vasheghani-Farahani, A.A.M. Movahedi, Int. J. Nanomed. 6 (2011) 1977-1990. |
| [65] |
M.S. Gee, R. Upadhyay, H. Bergquist, et al., Radiology 248 (2008) 925-935. DOI:10.1148/radiol.2482071496 |
| [66] |
K. Sano, M. Mitsunaga, T. Nakajima, P.L. Choyke, H. Kobayashi, Breast Cancer Res. 14 (2012) R61. |
| [67] |
H. Ogiso, R. Ishitani, O. Nureki, et al., Cell 110 (2002) 775-787. DOI:10.1016/S0092-8674(02)00963-7 |
| [68] |
M.J. Crow, G. Grant, J.M. Provenzale, A. Wax, Am. J. Roentgenol. 192 (2009) 1021-1028. DOI:10.2214/AJR.07.3535 |
| [69] |
S. Bhattacharyya, N.L. Patel, L. Wei, L.A. Riffle, J.D. Kalen, MedChemComm 5 (2014) 1337-1346. DOI:10.1039/C4MD00116H |
| [70] |
X. Hun, Z.J. Zhang, Spectrochim. Acta A 74 (2009) 410-414. DOI:10.1016/j.saa.2009.06.033 |
| [71] |
J.H. Ryu, M. Shin, S.A. Kim, S. Lee, H. Kim, Biomaterials 34 (2013) 9149-9159. DOI:10.1016/j.biomaterials.2013.08.026 |
| [72] |
S.B. Qi, Z. Miao, H.G. Liu, et al., Bioconjugate Chem. 23 (2012) 1149-1156. DOI:10.1021/bc200596a |
| [73] |
F. Su, B. Liu, M. Chen, et al., Int. J. Biol. Marker. 31 (2016) e235-e244. DOI:10.5301/jbm.5000198 |
| [74] |
A.G.T.T. van Scheltinga, G.M. van Dam, W.B. Nagengast, V. Ntziachristos, J. Nucl. Med. 52 (2011) 1778-1785. DOI:10.2967/jnumed.111.092833 |
| [75] |
L.L. Pang, J. Xu, C. Shu, et al., Luminescence 29 (2014) 1177-1182. DOI:10.1002/bio.v29.8 |
| [76] |
N.C. Biswal, J.K. Gamelin, B.H. Yuan, M.V. Backer, J.M. Backer, J. Biomed. Opt. 5 (2010) 016012. |
| [77] |
Q.M. Xiang, L.W. Wang, J.P. Yuan, J.M. Chen, Exp. Mol. Pathol. 99 (2015) 133-138. DOI:10.1016/j.yexmp.2015.06.013 |
| [78] |
L. Wang, Z.C. Fan, J.Y. Zhang, Y.Z. Changyi, C.Y. Huang, Int. J. Cancer 136 (2015) E107-E116. DOI:10.1002/ijc.29153 |
| [79] |
J.T. Zhang, M. Yang, C. Li, et al., J. Mater. Chem. B 3 (2015) 2173-2184. DOI:10.1039/C4TB01878H |
| [80] |
J.E. Mathejczyk, J. Pauli, C. Dullin, et al., J. Biomed. Opt. 17 (2012) 076028. DOI:10.1117/1.JBO.17.7.076028 |
| [81] |
R. Soudy, A. Gill, T. Sprules, A. Lavasanifar, J. Med. Chem. 54 (2011) 7523-7534. DOI:10.1021/jm200750x |
| [82] |
X.L. Li, W.Y. Zhang, L. Liu, Z. Zhu, G.L. Ouyang, Anal. Chem. 86 (2014) 6596-6603. DOI:10.1021/ac501205q |
| [83] |
P. Wu, Y. Gao, H. Zhang, C.X. Cai, Anal. Chem. 84 (2012) 7692-7699. DOI:10.1021/ac3015164 |
| [84] |
S.N. He, L. Qu, Z.F. Shen, et al., Anal. Chem. 87 (2015) 569-577. DOI:10.1021/ac5031557 |
| [85] |
H. Jo, J. Her, C. Ban, Biosens. Bioelectron. 71 (2015) 129-136. DOI:10.1016/j.bios.2015.04.030 |
| [86] |
S.B. Mondal, S.K. Gao, N. Zhu, et al., Adv. Cancer Res. 124 (2014) 171-211. DOI:10.1016/B978-0-12-411638-2.00005-7 |
| [87] |
J.C. DeLong, R.M. Hoffman, M. Bouvet, Expert Rev. Anticancer 16 (2016) 71-81. DOI:10.1586/14737140.2016.1121109 |
| [88] |
S. Leng, Q. Qiao, L. Miao, et al., Chin. Chem. Lett. 28 (2017) 1911-1915. DOI:10.1016/j.cclet.2017.08.054 |
| [89] |
W. Stummer, A. Novotny, H. Stepp, et al., J. Neurosurg. 93 (2000) 1003-1013. DOI:10.3171/jns.2000.93.6.1003 |
| [90] |
G.M. van Dam, G. Themelis, L.M.A. Crane, et al., Nat. Med. 17 (2011) 1315. DOI:10.1038/nm.2472 |
| [91] |
Y. Yang, H. Wang, Y. Wei, et al., Chin. Chem. Lett. 28 (2017) 2023-2026. DOI:10.1016/j.cclet.2017.08.051 |
| [92] |
Z. Xu, J. Chen, L. Hu, et al., Chin. Chem. Lett. 28 (2017) 1935-1942. DOI:10.1016/j.cclet.2017.07.018 |