 2022, Vol. 49
2022, Vol. 49文章信息
- 腹膜癌新发病例的流行病学研究
- Epidemiological Study of New Cases of Peritoneal Metastases
- 肿瘤防治研究, 2022, 49(11): 1190-1194
- Cancer Research on Prevention and Treatment, 2022, 49(11): 1190-1194
- http://www.zlfzyj.com/CN/10.3971/j.issn.1000-8578.2022.22.0270
- 收稿日期: 2022-03-18
- 修回日期: 2022-05-29
引用本文 |



腹膜癌(peritoneal metastases, PM)是指在腹膜上发生和发展的一类恶性肿瘤,包括原发性PM和继发性PM两种。前者的典型代表是原发性腹膜癌和恶性腹膜间皮瘤(malignant peritoneal mesothelioma, MPM)。后者是各种肿瘤所形成的腹膜转移癌,常见的是胃肠道肿瘤及妇科肿瘤的腹膜转移癌。根据临床确诊PM的时间不同,继发性PM可分为同时性PM和异时性PM。同时性PM是指初诊恶性肿瘤时即发现腹膜转移,包括腹水中检测到癌细胞和(或)术中发现腹膜转移。异时性PM是指恶性肿瘤患者接受以根治性手术为主的综合性治疗后,随访期间发现的腹膜转移[1]。
既往PM被认为是一种终末期疾病,但近40年来,随着对PM认识的转变,肿瘤学界将其视为一种可治性区域癌转移,以此开创了以肿瘤细胞减灭术(cytoreductive surgery, CRS)加腹腔热灌注化疗(hyperthermic intraperitoneal chemotherapy, HIPEC)为核心的综合治疗体系,显著改善了患者生存[2]。虽然HIPEC在腹膜癌中已有应用[3],但CRS+HIPEC技术复杂、操作难度大,对肿瘤学医师以及专科护理团队要求极高,一般只能在规范化腹膜癌诊疗中心开展此类手术。然而目前国内规范化PM诊疗中心少,患者群体大,急需建立足够数量的专业化腹膜癌中心,但国内尚缺乏PM相关流行病学数据。因此本文旨在根据我国国家癌症中心发布的癌症新发病例统计数据,结合PM的临床预后资料,按照临床流行病学的研究方法,估算我国所需PM诊疗中心数,为CRS+HIPEC的技术推广及PM诊疗中心的建设提供数据支撑,促进腹膜肿瘤学科发展。
1 胃癌腹膜转移胃癌(gastric cancer, GC)是全世界最常见的恶性肿瘤之一,约占恶性肿瘤总例数的5.7%,其导致的死亡例数在恶性肿瘤中居第3位[4]。GC常见的转移方式包括直接浸润、淋巴转移、血行转移、腹膜种植转移等。腹膜种植转移是指GC细胞脱落种植于腹腔壁腹膜或脏腹膜表面,并在局部定植增生形成转移灶。因GC PM多为腹腔弥漫性病变,多数分期系统均将其归为晚期病变,指南推荐行姑息化疗或支持治疗[5]。据文献报道,GC PM患者仅接受支持治疗,中位生存期仅为3~4个月[6-7]。接受姑息性化疗的患者,由于血浆-腹膜屏障的存在,系统化疗难以在腹腔局部病灶达到有效的药物浓度,效果较差,中位生存期仅为8~10个月[8]。然而如果经选择的GC PM患者,接受了规范化的CRS+HIPEC治疗后,中位生存期能达到11~21个月,极少数甚至可达到临床治愈[8-10]。
2014年荷兰的一项GC流行病学研究统计分析了1995—2011年间在埃因霍温癌症登记处(The Eindhoven Cancer Registry)登记的5 220例GC患者,数据显示,约14%的患者在初诊时即发现存在PM[6]。另一项来自荷兰国家癌症中心的GC流行病学数据显示,2008—2017年虽然GC发病率下降,但同时性GC PM率持续上升,最高为2017年的27%[11]。GC患者在行GC根治术后有一部分患者仍然会出现肿瘤复发,其中一部分为PM。国外有研究统计,GC根治术后43%的患者会出现PM复发,即异时性PM,12%的患者出现淋巴结转移复发,22%的患者局部复发,25%的患者多部位转移复发[12]。
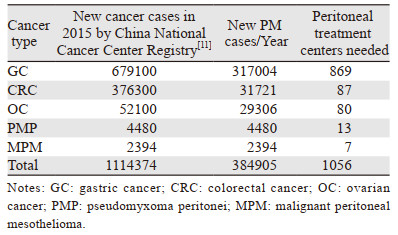
据中国国家癌症中心统计,2015年中国新发GC患者例数约为679 100例[13],90%患者(n=611 190)初诊时即为进展期GC;14%患者(n=95 074)确诊时已发现了PM,其余76%患者(n=516 116)在接受GC根治术后,又有43%患者(n=221 930)会出现以PM为主要形式的复发[14],这样算来每年新发GC患者中出现同时性PM和异时性PM的总例数为317 004例。根据估计,一个规范的PM诊疗中心年手术量大约为365台,要满足中国每年新发GC PM患者的就诊需求需要大约869个PM诊疗中心。
2 结直肠癌腹膜转移结直肠癌(colorectal cancer, CRC)发病率在全世界位居所有肿瘤中的第3位,死亡率位居第2位[3]。腹膜是结直肠癌常见的转移部位,预后较肝、肺等转移差。荷兰埃因霍温癌症登记处的一项流行病学调查显示,CRC PM患者的中位生存期仅为6个月,远低于其他器官远处转移的15个月[15]。既往研究发现,与系统化疗或姑息手术相比,CRS+HIPEC可显著提高CRC PM患者的无病生存率,降低复发风险,延长生存期达到14~54个月,且不会增加与治疗相关的死亡率[16]。然而PRODIGE7的结果表明,结直肠癌腹膜转移患者接受CRS或CRS+HIPEC治疗后的生存无显著差异[17],这在肿瘤学界引起了巨大争议。因此在第11届国际腹膜癌大会上,全球的腹膜肿瘤学家针对该研究,进行了深刻的分析和探讨,最终认为,该研究在入组患者、HIPEC方案等方面存在明显不足,其结果不足以否定HIPEC的治疗作用,该方案采用的是大剂量奥沙利铂方案,时间仅为30 min,但腹膜癌领域都知道大剂量奥沙利铂方案不良反应较大,以丝裂霉素为主的方案应用更加广泛。其次,更广泛的HIPEC方案时长为60~90 min,30 min难以充分发挥HIPEC的疗效。van de Vlasakker等[18]进一步指出“以手术为主的整合治疗”的根本原则:以CRS为核心,HIPEC为必要辅助,且必须符合肿瘤药物治疗“机制互补、疗效协同”的基本原理。
国外的多项流行病学调查数据显示,CRC患者初诊时出现PM,即CRC同时性PM的发病率约为5.5%[19-22]。非PM患者在接受根治性手术为主的治疗后,出现异时性PM的发病率约为3.1%[15, 21-23]。根据中国国家癌症中心统计的数据,2015年中国新发CRC患者例数约为376 300例[12]。参考国外流行病学统计的CRC同时性/异时性PM的发病率,可估算出中国每年新发的CRC PM患者的例数约为31 721例,由此推算大约需要90个PM诊疗中心,才能满足中国每年新发CRC PM患者的治疗需求。
3 卵巢癌腹膜转移卵巢癌(ovarian cancer, OC)是第二常见的妇科肿瘤,是引起女性肿瘤患者死亡的最主要原因。全球范围内,每年有超过20万女性新诊断为OC[4]。其中大多数患者就诊时已处于临床晚期(FIGO Ⅲ~Ⅳ期),肿瘤已经累及腹膜或已发生远处转移[24-25]。
根据美国SEER(The Surveillance, Epidemiology, and End Results)数据库统计(https://seer.cancer.gov/statfacts/html/ovary.html .),美国OC年发病率为10.9/10万,死亡率为6.5/10万。OC患者初诊时,病变局限于原发部位者仅占16%,剩余84%的患者已经出现区域性淋巴受累或是远处转移。OC患者的平均5年生存率大约为49.1%,且出现远处转移后5年生存率显著下降,仅为30.3%。du Bois等综合分析了3项前瞻性随机Ⅲ期多中心试验,其中FIGO ⅢC期或FIGO Ⅳ期的OC患者接受完全性CRS治疗后,中位总生存期分别能达到81和55个月[26]。
根据中国国家癌症中心统计,2015年中国新发OC患者例数约为52 100例[12]。这部分新诊断的OC患者中,有75%的患者在确诊时已是晚期OC,而在这些晚期OC患者中75%的患者已经出现或将会出现PM[27]。这样估算,每年新发OC患者中约有29 306例会存在PM。根据1个PM诊疗中心年手术量365台来计算,中国需要80个PM诊疗中心来满足OC PM患者的诊疗需求。
4 腹膜假黏液瘤腹膜假黏液瘤(pseudomyxoma peritonei, PMP)是一种恶性肿瘤临床综合征,可由多种脏器原发性黏液性肿瘤腹腔播散导致。据文献报道,约90%以上的PMP都是来源于阑尾黏液性肿瘤,少部分源于卵巢、结肠、脐尿管等脏器的原发性黏液性肿瘤[28]。
2000年前,国内外PMP的流行病学调查很少。2008年荷兰的一项全国性调查显示,PMP患者中,男性的中位诊断年龄为63岁,女性为62岁,而据NKI(Netherlands cancer institute)数据库统计,PMP的中位诊断年龄为57岁(30~77岁)[29]。一项挪威和英格兰的PMP流行病学调查,统计了2009—2018年10年间PMP的发病率,结果显示,10年间两个国家的平均发病率皆为3.2/100万[30]。
2008年,国际腹膜表面肿瘤协作组(peritoneal surface oncology group international, PSOGI)就CRS+HIPEC治疗PMP达成首个专家共识[31]。2012年Chua等[32]的一项多中心回顾性研究统计分析了2 298例接受CRS+HIPEC治疗的PMP患者,结果显示,中位生存期为196个月,中位无进展生存期达到98个月,10年和15年生存率分别为63%和59%。
目前国内尚缺乏PMP的临床流行病学研究,国外大量相关研究显示PMP发病率为2/100万~4/100万[28]。以3.2/100万作为我国PMP发病率预估值,我国现总人口数大约为14亿人,按照3.2/100万的发病率来算,我国每年新发的PMP患者约为4 480例,要满足4 480例PMP患者的就诊需求大约需要12个PM诊疗中心。
5 恶性腹膜间皮瘤MPM目前的病因和发病机制相关研究较少,目前已知的致癌因素包括化学致癌因素,如石棉及其他矿物质纤维等,物理致癌因素如慢性腹膜炎等以及某些生物致癌因素。其中石棉是其主要的物理致癌因素,平均潜伏期为30~40.9年。据报道,我国很多地方仍存在石棉厂,主要存在于吉林省集安市、辽宁省锦州市、青海省茫崖市、四川省彭州市以及河北省涞源市。考虑到国内仍然存在相当数量的石棉厂,所以预估未来我国恶性间皮瘤患者的数量仍会上升[33-35]。
目前MPM在全球范围内的流行病学数据差异较大,且我国研究很少,2000年前几乎没有相关数据。Zhao等[36]国内学者对我国2000—2013年间的MPM患者进行了流行病学调查研究,发现2013年MPM的年龄标化发病率为1.71/100万,且发病率呈逐年递增的趋势。2008年Yan等[37]的一项多中心研究显示,405例接受CRS+HIPEC的MPM患者,中位生存期为53个月,3年和5年生存率分别为60%和47%。
以Zhao等[36]对我国2013年MPM进行流行病学研究的结果作为我国MPM发病率的预估值。目前,我国现总人口数大约为14亿人,按照1.71/100万的发病率来算,我国每年新发的MPM患者约为2 394人,要满足这部分患者的诊疗需求,大约需要7个PM诊疗中心。
6 总结根据以上统计,我国每年新发腹膜癌患者总数约为384 905例,其中占比最大的是GC PM(82.4%),其次分别为CRC PM(8.2%)、OC PM(7.6%)、PMP(1.2%)、MPM(0.6%),见表 1。目前腹膜癌的治疗是以CRS为核心、HIPEC为必要补充的整合治疗体系,但作为一个发展中的技术体系,从理论认识到技术方法、从临床选择到结果评价,都存在很大的探索和讨论空间。对于HIPEC治疗CRC PM、OC PM,国际肿瘤学界尚存在争议[17, 38],仍需要大样本前瞻性临床研究的验证。但HIPEC对于接受CRS后的GC PM、PMP、MPM患者[39-41]的疗效是受到广泛认可的。据本文统计,GC PM、PMP、MPM患者约占总体PM患者的84.2%,因此以CRS+HIPEC作为专业化腹膜癌中心的关键技术是合理且必需的。
|
根据表 1统计,要满足我国每年新增的原发性和继发性PM患者的诊疗需求,大约需要1 056个规范化PM诊疗中心。根据2021年中国卫生健康统计年鉴[42],目前我国有三级医院2 996个,其中三甲医院约1 580个,考虑到CRS+HIPEC手术专业性极强、难度极大,一般只能在三级甲等医院开展此类手术,所以大约每1.5个三甲医院就需要建立1个PM诊疗中心。然而,目前国内现有的规范化PM诊疗中心少,需求与现有的差距大,预示着建设全国范围的规范化PM诊疗中心之路任重而道远。
本文不足之处在于,文中流行病学数据大多参考国际流行病学研究,相关估算值可能存在偏差。此外年新发病例数根据年发病率所估算,但目前经CRS+HIPEC治疗后,PM患者中位生存期超过3年[43],年患病例数应远高于年新发病例数,因此所需规范化腹膜癌诊疗中心远多于本文估算值。未来尚需进一步加强国内PM相关流行病学调查,并采用年患病人数来估算所需腹膜癌诊疗中心数。
作者贡献:
杨锐:文献检索、文章撰写
苏延冬、马茹:文章修改
安松林、林育林:文献检索
李雁:文章构思、文章修改
| [1] |
李雁. 腹膜癌研究之我见[J]. 中国肿瘤临床, 2012, 39(22): 1685-1686. [Li Y. My opinion on peritoneal cancer research[J]. Zhongguo Zhong Liu Lin Chuang, 2012, 39(22): 1685-1686. DOI:10.3969/j.issn.1000-8179.2012.22.001] |
| [2] |
李雁, 周云峰, 梁寒, 等. 细胞减灭术加腹腔热灌注化疗治疗腹膜表面肿瘤的专家共识[J]. 中国肿瘤临床, 2015, 42(4): 198-206. [Li Y, Zhou YF, Liang H, et al. Expert consensus on cytoreductive surgery plus intraperitoneal hyperthermic chemotherapy in the treatment of peritoneal surface oncology[J]. Zhongguo Zhong Liu Lin Chuang, 2015, 42(4): 198-206. DOI:10.3969/j.issn.1000-8179.20150013] |
| [3] |
詹宏杰, 梁寒. 腹腔热灌注化疗在腹膜癌中的应用现状[J]. 肿瘤防治研究, 2021, 48(4): 327-332. [Zhan HJ, Liang H. Current Situation of Hyperthermic Intraperitoneal Chemotherapy in Peritoneal Carcinoma[J]. Zhong Liu Fang Zhi Yan Jiu, 2021, 48(4): 327-332. DOI:10.3971/j.issn.1000-8578.2021.20.1280] |
| [4] |
Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71(3): 209-249. DOI:10.3322/caac.21660 |
| [5] |
Ajani JA, D'Amico TA, Bentrem DJ, et al. Gastric cancer, version 2. 2022, NCCN clinical practice guidelines in oncology[J]. J Natl Compr Canc Netw, 2022, 20(2): 167-192. DOI:10.6004/jnccn.2022.0008 |
| [6] |
Thomassen I, van Gestel YR, van Ramshorst B, et al. Peritoneal carcinomatosis of gastric origin: A population-based study on incidence, survival and risk factors[J]. Int J Cancer, 2014, 134(3): 622-628. DOI:10.1002/ijc.28373 |
| [7] |
Kang JH, Lee SI, Lim DH, et al. Salvage chemotherapy for pretreated gastric cancer: A randomized phase iii trial comparing chemotherapy plus best supportive care with best supportive care alone[J]. J Clin Oncol, 2012, 30(13): 1513-1518. DOI:10.1200/JCO.2011.39.4585 |
| [8] |
Brandl A, Yonemura Y, Glehen O, et al. Long term survival in patients with peritoneal metastasised gastric cancer treated with cytoreductive surgery and HIPEC: A multi-institutional cohort from PSOGI[J]. Eur J Surg Oncol, 2021, 47(1): 172-180. DOI:10.1016/j.ejso.2020.10.006 |
| [9] |
Yu P, Ye Z, Dai G, et al. Neoadjuvant systemic and hyperthermic intraperitoneal chemotherapy combined with cytoreductive surgery for gastric cancer patients with limited peritoneal metastasis: A prospective cohort study[J]. BMC Cancer, 2020, 20(1): 1108. DOI:10.1186/s12885-020-07601-x |
| [10] |
Ji ZH, Yu Y, Liu G, et al. Peritoneal cancer index (PCI) based patient selecting strategy for complete cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy in gastric cancer with peritoneal metastasis: A single-center retrospective analysis of 125 patients[J]. Eur J Surg Oncol, 2021, 47(6): 1411-1419. DOI:10.1016/j.ejso.2020.11.139 |
| [11] |
Koemans WJ, Lurvink RJ, Grootscholten C, et al. Synchronous peritoneal metastases of gastric cancer origin: Incidence, treatment and survival of a nationwide Dutch cohort[J]. Gastric Cancer, 2021, 24(4): 800-809. DOI:10.1007/s10120-021-01160-1 |
| [12] |
Maehara Y, Hasuda S, Koga T, et al. Postoperative outcome and sites of recurrence in patients following curative resection of gastric cancer[J]. Br J Surg, 2000, 87(3): 353-357. |
| [13] |
Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015[J]. CA Cancer J Clin, 2016, 66(2): 115-132. DOI:10.3322/caac.21338 |
| [14] |
朱正纲. 预防与治疗胃癌腹膜转移的若干关键问题[J]. 外科理论与实践, 2021, 26(1): 1-6. [Zhu ZG. Several key issues in the prevention and treatment of gastric cancer peritoneal metastasis[J]. Wai Ke Li Lun Yu Shi Jian, 2021, 26(1): 1-6. DOI:10.16139/j.1007-9610.2021.01.001] |
| [15] |
van Gestel YR, Thomassen I, Lemmens VE, et al. Metachronous peritoneal carcinomatosis after curative treatment of colorectal cancer[J]. Eur J Surg Oncol, 2014, 40(8): 963-969. DOI:10.1016/j.ejso.2013.10.001 |
| [16] |
Sánchez-Hidalgo JM, Rodríguez-Ortiz L, Arjona-Sánchez Á, et al. Colorectal peritoneal metastases: Optimal management review[J]. World J Gastroenterol, 2019, 25(27): 3484-3502. DOI:10.3748/wjg.v25.i27.3484 |
| [17] |
Quénet F, Elias D, Roca L, et al. Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy versus cytoreductive surgery alone for colorectal peritoneal metastases (prodige 7): A multicentre, randomised, open-label, phase 3 trial[J]. Lancet Oncol, 2021, 22(2): 256-266. DOI:10.1016/S1470-2045(20)30599-4 |
| [18] |
van de Vlasakker VCJ, Lurvink RJ, Cashin PH, et al. The impact of PRODIGE 7 on the current worldwide practice of CRS-HIPEC for colorectal peritoneal metastases: A web-based survey and 2021 statement by peritoneal surface oncology group international (PSOGI)[J]. Eur J Surg Oncol, 2021, 47(11): 2888-2892. DOI:10.1016/j.ejso.2021.05.023 |
| [19] |
Lemmens VE, Klaver YL, Verwaal VJ, et al. Predictors and survival of synchronous peritoneal carcinomatosis of colorectal origin: A population-based study[J]. Int J Cancer, 2011, 128(11): 2717-2725. DOI:10.1002/ijc.25596 |
| [20] |
Segelman J, Granath F, Holm T, et al. Incidence, prevalence and risk factors for peritoneal carcinomatosis from colorectal cancer[J]. Br J Surg, 2012, 99(5): 699-705. DOI:10.1002/bjs.8679 |
| [21] |
Kerscher AG, Chua TC, Gasser M, et al. Impact of peritoneal carcinomatosis in the disease history of colorectal cancer management: A longitudinal experience of 2406 patients over two decades[J]. Br J Cancer, 2013, 108(7): 1432-1439. DOI:10.1038/bjc.2013.82 |
| [22] |
Quere P, Facy O, Manfredi S, et al. Epidemiology, management, and survival of peritoneal carcinomatosis from colorectal cancer: A population-based study[J]. Dis Colon Rectum, 2015, 58(8): 743-752. DOI:10.1097/DCR.0000000000000412 |
| [23] |
Ravn S, Heide-Jørgensen U, Christiansen CF, et al. Overall risk and risk factors for metachronous peritoneal metastasis after colorectal cancer surgery: A nationwide cohort study[J]. BJS Open, 2020, 4(2): 284-292. DOI:10.1002/bjs5.50247 |
| [24] |
Steffen T, Häller L, Bijelic L, et al. Decision-making analysis for hyperthermic intraperitoneal chemotherapy in ovarian cancer: A survey by the executive committee of the peritoneal surface oncology group international (PSOGI)[J]. Oncology, 2021, 99(1): 41-48. DOI:10.1159/000510098 |
| [25] |
Prat J, FIGO Committee on Gynecologic Oncology. Staging classification for cancer of the ovary, fallopian tube, and peritoneum: Abridged republication of guidelines from the international federation of gynecology and obstetrics (FIGO)[J]. Obstet Gynecol, 2015, 126(1): 171-174. DOI:10.1097/AOG.0000000000000917 |
| [26] |
du Bois A, Reuss A, Pujade-Lauraine E, et al. Role of surgical outcome as prognostic factor in advanced epithelial ovarian cancer: A combined exploratory analysis of 3 prospectively randomized phase 3 multicenter trials: By the arbeitsgemeinschaft gynaekologische onkologie studiengruppe ovarialkarzinom (AGO-OVAR) and the groupe d'investigateurs nationaux pour les etudes des cancers de l'ovaire (GINECO)[J]. Cancer, 2009, 115(6): 1234-1244. DOI:10.1002/cncr.24149 |
| [27] |
Lheureux S, Gourley C, Vergote I, et al. Epithelial ovarian cancer[J]. Lancet, 2019, 393(10177): 1240-1253. DOI:10.1016/S0140-6736(18)32552-2 |
| [28] |
李雁, 许洪斌, 彭正, 等. 肿瘤细胞减灭术加腹腔热灌注化疗治疗腹膜假黏液瘤专家共识[J]. 中华医学杂志, 2019, 99(20): 1527-1535. [Li Y, Xu HB, Peng Z, et al. Expert consensus on cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy for the treatment of pseudomyxoma peritonei[J]. Zhonghua Yi Xue Za Zhi, 2019, 99(20): 1527-1535. DOI:10.3760/cma.j.issn.0376-2491.2019.20.003] |
| [29] |
Smeenk RM, van Velthuysen ML, Verwaal VJ, et al. Appendiceal neoplasms and pseudomyxoma peritonei: A population based study[J]. Eur J Surg Oncol, 2008, 34(2): 196-201. DOI:10.1016/j.ejso.2007.04.002 |
| [30] |
Patrick-Brown T, Carr NJ, Swanson DM, et al. Estimating the prevalence of pseudomyxoma peritonei in Europe using a novel statistical method[J]. Ann Surg Oncol, 2021, 28(1): 252-257. DOI:10.1245/s10434-020-08655-8 |
| [31] |
Moran B, Baratti D, Yan TD, et al. Consensus statement on the loco-regional treatment of appendiceal mucinous neoplasms with peritoneal dissemination (pseudomyxoma peritonei)[J]. J Surg Oncol, 2008, 98(4): 277-282. DOI:10.1002/jso.21054 |
| [32] |
Chua TC, Moran BJ, Sugarbaker PH, et al. Early- and long-term outcome data of patients with pseudomyxoma peritonei from appendiceal origin treated by a strategy of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy[J]. J Clin Oncol, 2012, 30(20): 2449-2456. DOI:10.1200/JCO.2011.39.7166 |
| [33] |
Cai SX, Zhang CH, Zhang X, et al. Epidemiology of occupational asbestos-related diseases in China[J]. Ind Health, 2001, 39(2): 75-83. DOI:10.2486/indhealth.39.75 |
| [34] |
唐慧娟, 陈天辉, 蒋曦依, 等. 石棉所致恶性间皮瘤的流行现状及其早期诊断[J]. 国际流行病学传染病学杂志, 2017, 44(4): 278-281. [Tang HJ, Chen TH, Jiang XY, et al. Advances on epidemic status of asbestos-related malignant mesothelioma and its early diagnosis[J]. Guo Ji Liu Xing Bing Xue Chuan Ran Bing Xue Za Zhi, 2017, 44(4): 278-281. DOI:10.3760/cma.j.issn.1673-4149.2017.04.014] |
| [35] |
黄晓云, 叶俏. 石棉所致肿瘤的流行病学研究进展[J]. 中华劳动卫生职业病杂志, 2021, 39(3): 233-236. [Huang XY, Ye Q. Asbestos exposure and asbestos related malignant diseases: an epidemiological review[J]. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi, 2021, 39(3): 233-236. DOI:10.3760/cma.j.cn121094-20200226-00089] |
| [36] |
Zhao J, Zuo T, Zheng R, et al. Epidemiology and trend analysis on malignant mesothelioma in China[J]. Chin J Cancer Res, 2017, 29(4): 361-368. DOI:10.21147/j.issn.1000-9604.2017.04.09 |
| [37] |
Yan TD, Deraco M, Baratti D, et al. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for malignant peritoneal mesothelioma: Multi-institutional experience[J]. J Clin Oncol, 2009, 27(36): 6237-6242. DOI:10.1200/JCO.2009.23.9640 |
| [38] |
Lim MC, Chang SJ, Park B, et al. Survival after hyperthermic intraperitoneal chemotherapy and primary or interval cytoreductive surgery in ovarian cancer: A randomized clinical trial[J]. JAMA Surg, 2022, 157(5): 374-383. DOI:10.1001/jamasurg.2022.0143 |
| [39] |
Bonnot PE, Lintis A, Mercier F, et al. Prognosis of poorly cohesive gastric cancer after complete cytoreductive surgery with or without hyperthermic intraperitoneal chemotherapy (CYTO-CHIP study)[J]. Br J Surg, 2021, 108(10): 1225-1235. DOI:10.1093/bjs/znab200 |
| [40] |
Yan TD, Deraco M, Baratti D, et al. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for malignant peritoneal mesothelioma: multi-institutional experience[J]. J Clin Oncol, 2009, 27(36): 6237-6242. DOI:10.1200/JCO.2009.23.9640 |
| [41] |
Kusamura S, Barretta F, Yonemura Y, et al. The role of hyperthermic intraperitoneal chemotherapy in pseudomyxoma peritonei after cytoreductive surgery[J]. JAMA Surg, 2021, 156(3): e206363. DOI:10.1001/jamasurg.2020.6363 |
| [42] |
国家卫生健康委员会. 中国卫生健康统计年鉴(2021)[M]. 北京: 中国协和医科大学出版社, 2021: 13-14. [National Health Commission of the People's Republic of China. China Health Statistical Yearbook[M]. Beijing: China Union Medical College Press, 2021: 13-14.]
|
| [43] |
于洋, 李鑫宝, 林育林, 等. 肿瘤细胞减灭术联合腹腔热灌注化疗治疗腹膜癌1 384例疗效分析[J]. 中华胃肠外科杂志, 2021, 24(3): 230-239. [Yu Y, Li XB, Lin YL, et al. Efficacy of 1, 384 cases of peritoneal carcinomatosis underwent cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy[J]. Zhonghua Wei Chang Wai Ke Za Zhi, 2021, 24(3): 230-239.] |