 2021, Vol. 48
2021, Vol. 48文章信息
- 老年食管癌患者三维适形放疗后发生放射性肺炎与剂量体积参数的相关性
- Correlation Between Dose Volume Parameters and Radiation Pneumonitis in Elderly Patients with Esophageal Cancer After Three-dimensional Conformal Radiotherapy
- 肿瘤防治研究, 2021, 48(2): 173-177
- Cancer Research on Prevention and Treatment, 2021, 48(2): 173-177
- http://www.zlfzyj.com/CN/10.3971/j.issn.1000-8578.2021.20.1323
- 收稿日期: 2020-11-16
- 修回日期: 2021-01-13
引用本文 |



2. 210009 南京,东南大学附属中大医院肿瘤科;
3. 224500 泰州,靖江市人民医院放疗科
2. Department of Oncology, Zhongda Hospital of Southeast University, Nanjing 210009, China;
3. Department of Radiotherapy, Jingjiang People's Hospital, Taizhou 224500, China
目前,食管癌的发病率和死亡率均较高(占恶性肿瘤总发病率的4.2%,总死亡率的6.6%)[1],且我国食管癌的发病率和死亡率均高于全球平均水平[2],放疗是食管癌重要的治疗手段之一,而放射性肺炎(radiation pneumonitis, RP)作为胸部放疗最常见的不良反应,短期内可引起咳嗽、气短、发热等症状,长期可引起肺纤维化、肺功能损伤,影响患者的生活质量,严重时甚至导致患者死亡,且放射性肺炎会限制临床医生给予的处方剂量,从而影响治疗效果和患者预后。RP的发病率也较高,有学者统计发现食管癌患者接受放疗后发生≥2级RP的风险约为22%[3],而老年食管患者接受放疗后发生RP的风险可高达52.4%[4],这提示老年食管癌患者在接受放射治疗时需要更多重视。为避免RP发生,剂量体积直方图(dose-volume histogram, DVH)常用于评估放疗计划,其中肺平均剂量(mean lung dose, MLD)和V20(接受≥20Gy肺体积占总肺体积百分比)常作为约束指标,但效果欠佳[5],且目前应用DVH参数预测放疗后发生RP的研究尚无统一定论[6-8]。因此,本研究分析来自不同中心的老年食管癌患者的剂量体积参数与三维适形放疗后发生≥2级放射性肺炎的相关性,旨在为预防老年患者发生放射性肺炎提供帮助。
1 资料与方法 1.1 临床资料本研究为回顾性分析,选择2018年1月至2020年1月在东南大学附属中大医院以及江苏省泰州市靖江市人民医院接受三维适形放疗的食管癌患者,收集资料包括:(1)临床特征:性别、年龄、一般体力状况ECOG评分、吸烟史、化疗史。(2)剂量体积参数:V5、V10、V20、V30、MLD。患者放疗开始及放疗期间每两周进行随访,放疗结束后每月进行随访,随访内容包括采集病史、体格检查及胸部CT平扫检查,随访时间为3月。纳入标准:(1)病理明确诊断为食管鳞癌;(2)年龄:60~80岁;(4)PS评分:ECOG 0~2分;(5)放疗期间及结束后完整接受随访(3月),包括病史采集、查体及胸部CT平扫。排除标准:合并肺部基础疾病:包括肺间质性疾病、慢性阻塞性肺疾病等。共收集符合标准的患者250例,其中男151例(60.4%)、女99例(39.6%),平均年龄71岁;东南大学附属中大医院病例110例(44%),靖江市人民医院140例(56%)。
1.2 治疗计划与实施所有患者均接受三维适形放疗,东南大学附属中大医院应用热塑模固定,定位CT以5 mm层厚扫描,包括中下颈部和全胸部及上腹部,传输图像至Release 4.3.1治疗系统,放疗使用西门子Primus-m直线加速器。靖江市人民医院应用真空垫体模固定,定位CT以3 mm层厚扫描,包括中下颈部和全胸部及上腹部,传输图像至Eclipse 8.6治疗计划系统,放疗使用Varian23 EX直线加速器。食管癌PTV为CTV外扩5~10 mm,根治性放疗处方剂量为60 Gy,术后辅助放疗处方剂量50~60 Gy,均应用2 Gy/F常规分割,以98%等剂量线包绕95%以上计划靶体积,正常组织限量:脊髓剂量 < 45 Gy;心脏V30 < 40%,V40 < 30%;双肺平均剂量 < 20 Gy,V20 < 30%,V30 < 20%,同步化疗时双肺V20限制 < 28%。250例老年食管癌患者中,113例食管鳞癌患者接受了小剂量顺铂/奈达铂同步放化疗(45.2%)。
1.3 放射性肺炎的诊断与分级放射性肺炎诊断标准采用肿瘤放射治疗学第5版标准:(1)既往6月内有肺受照射病史;(2)CT影像学改变主要局限在照射区域内,病变与正常肺组织的解剖结构不符;(3)多有咳嗽、气短、发热等临床症状;(4)排除能引起类似症状的其他因素[9]。放射性肺炎的分级标准采用不良事件通用术语标准第5版分为:1级:无症状,仅临床或影像学所见,无需治疗;2级:有症状,影响应用工具的日常活动,需治疗;3级:重度症状,影响自理性活动,需吸氧;4级:危及生命的呼吸障碍,需气管切开或插管;5级:死亡[10],由至少两名放疗专科医生评估分级。
1.4 统计学方法采用SPSS23.0软件对数据进行统计分析,卡方检验分析放射性肺炎组与非放射性肺炎组患者临床特征的差异;单因素Logistic回归分析DVH参数中与发生≥2级RP相关的因素;将单因素分析中有统计学意义的DVH参数纳入多因素Logistic回归,分析与发生≥2级RP独立相关的因素;应用ROC曲线分析发生≥2级RP独立相关的DVH参数的AUC值及最佳分界值,取约登指数最大时的值。样本量采用EPV法(events per variable)确定。P < 0.05为差异有统计学意义。
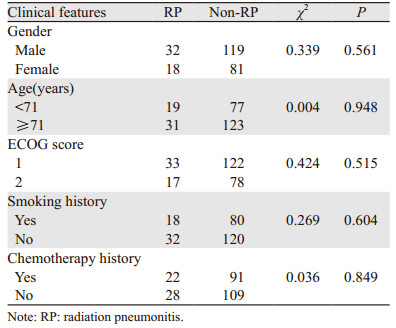
2 结果 2.1 患者的临床特征及放射性肺炎发生率将放射性肺炎组与非放射肺炎组患者的临床特征进行卡方检验,两组间性别(P=0.561)、平均年龄(P=0.948)、ECOG评分(P=0.515)、吸烟史(P=0.604)、化疗史(P=0.849)差异均无统计学意义,见表 1。
|
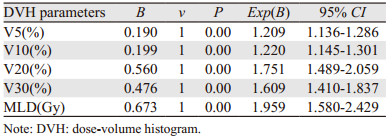
Logistic单因素分析与发生≥2级放射性肺炎相关的剂量体积参数,结果提示双肺V5(P < 0.05)、V10(P < 0.05)、V20(P < 0.05)、V30(P < 0.05)及MLD(P < 0.05)均是老年食管癌患者三维适形放疗后发生≥2级RP的相关因素,见表 2。
|
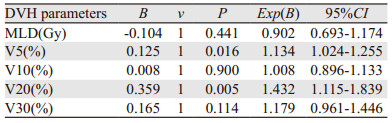
将单因素分析结果中与RP有显著相关性的DVH参数:双肺V5、V10、V20、V30、MLD进行Logistic多因素分析,结果显示仅双肺V5(P=0.016)、V20(P=0.005)有统计学意义,提示双肺V5、V20是老年食管癌患者三维适形放疗后发生≥2级RP的独立相关因素;双肺V10(P=0.900)、V30(P=0.114)及MLD(P=0.441)与发生≥2级RP有相关性,但不是发生≥2级RP的独立相关因素,见表 3。
|
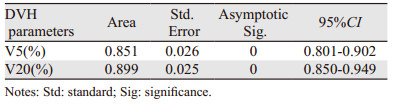
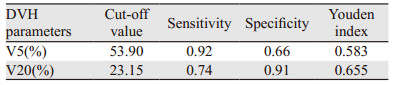
应用ROC曲线分析V5及V20预测≥2级放射性肺炎的效果及最佳分界值,见图 1。V5的ROC曲线下面积为0.851,95%CI: 0.801~0.902;V20的ROC曲线下面积为0.899,95%CI: 0.850~0.949,见表 4;V5预测≥2级RP的最佳分界值为53.90%,敏感度0.92,特异性0.66,约登指数为0.58;V20的最佳分界值为23.15%,敏感度为0.74,特异性为0.91,约登指数为0.66,见表 5。

|
| 图 1 250例老年食管癌患者发生≥2级RP的ROC曲线分析 Figure 1 ROC curve analysis for ≥grade 2 RP in 250 elderly patients with esophageal cancer |
放射性肺炎作为食管癌放疗较常见的并发症之一,是多种细胞和分子相互作用,引起大量成纤维细胞积累、增殖和分化,使细胞外基质沉积过多,最终导致肺纤维化的病理生理过程[11],但是RP发生的具体机制仍未明确,因此传统观点仍将剂量体积参数作为评估放疗计划的主要因素[12],以减少RP的发病风险,但目前尚无统一定论[13];临床工作中则应用V20 < 30%、MLD < 20~23Gy以规避RP的发生,但有研究表明效果欠佳[14];而老年患者的肺功能相对减弱,承受损伤的能力较差[15],在接受放射治疗时需要格外重视,因此本研究主要分析老年食管患者三维适形放疗后与≥2级RP相关的剂量体积参数,以便为控制、预防老年患者发生RP提供帮助。
本研究单因素分析表明双肺V5、V10、V20、V30及MLD均是老年食管癌放疗后发生≥2级RP的相关因素,提示DVH参数与RP发生紧密相关,与多数学者观点相符[16-18]。多因素分析结果示双肺V20是≥2级RP的独立相关因素,与多数学者的观点相符[19-21],且目前临床工作评估放疗计划时常约束双肺V20(低于28%~30%)以规避RP,但本研究则发现双肺V20应当 < 23.2%以规避≥2级RP发生,而Tonison的系统回顾也得出了类似的结论,认为应当将V20控制在23%以下[22]。这表明对于老年患者,剂量体积参数的控制应当更加严格,这可能与老年人的基础肺功能较差、肺生理结构改变有关[23]。另本研究还发现MLD与RP具有相关性,但不是RP的独立相关因素,部分关于食管癌患者发生RP的研究也得出了类似结论[24-26],提示对于食管癌患者,MLD预测RP发生的价值还有待进一步探讨。
本研究多因素分析还发现双肺V5也与≥2级RP独立相关,提示低剂量体积参数在预测RP发生方面具有重要价值。沈文斌等随访了222例接受三维适形放疗的食管癌患者,其中22.1%的患者发生了≥2级RP,回归分析发现V5和V20是RP的重要预测因素[27];Zhao等对68例食管癌患者的回顾分析发现,低剂量体积参数在预测RP方面更为重要[28];杜峰等将247例食管癌患者的V5~V40、MLD、GTV及吸烟指数等临床特征进行多因素回归分析,发现双肺V5是≥1级RP及≥3级RP的独立相关因素[29]。这些研究结果均认同了低剂量体积参数在预测RP方面的价值,但也有部分学者提出了不同观点:Zhao等通过对68例患者的回顾分析认为V30是RP的独立相关因素,而非V5和V20[28],但所研究的样本量较少;姚波等针对食管癌及肺癌患者的一项回顾性研究也发现V30与RP独立相关[30],但其研究样本量少(33例),并且在评估危及器官受量时,肺癌患者的双肺体积需扣除GTV后评估,而食管癌患者不存在此问题,因此将肺癌与食管癌患者的肺部DVH参数混合分析可能会对研究结果造成影响。
本研究则应用EPV法确定样本量,共收集了250例食管癌患者的数据,样本量较上述研究更多,并针对分析了5项与RP相关的DVH参数;且样本来源于不同等级的医疗中心,更具有代表性;且主要针对肺功能更为脆弱、更易发生RP的老年患者,具有临床意义。
综上所述,双肺V5和V20是老年食管癌患者三维适形放疗后发生≥2级放射性肺炎的独立相关因素;对于老年患者,剂量体积参数的约束应当更加严格,应当控制双肺V5 < 53.9%,V20 < 23.2%以规避≥2级放射性肺炎发生。
作者贡献:
汪盛:设计及实施研究、采集整理数据、统计分析及撰写论文
王彩莲:论文选题、修改论文
范丽华:采集整理数据
| [1] |
Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2018, 68: 394-424. DOI:10.3322/caac.21492 |
| [2] |
陈茹, 郑荣寿, 张思维, 等. 2015年中国食管癌发病和死亡情况分析[J]. 中华预防医学杂志, 2019, 53(11): 1094-1097. [Chen R, Zheng RS, Zhang SW, et al. Analysis of incidence and mortality of esophageal cancer in China, 2015[J]. Zhonghua Yu Fang Yi Xue Za Zhi, 2019, 53(11): 1094-1097.] |
| [3] |
Castillo R, Pham N, Castillo E, et al. Pre-radiation therapy fluorine 18 fluorodeoxyglucose PET helps identify patients with esophageal cancer at high risk for radiation pneumonitis[J]. Radiology, 2015, 275(3): 822-831. DOI:10.1148/radiol.14140457 |
| [4] |
马晓洁, 胡劲, 谭榜宪. 老年食管癌三维适形放疗致急性放射性肺炎的临床危险因素[J]. 中国老年学杂志, 2015, 35(2): 486-488. [Ma XJ, Hu J, Tan BX. Clinical risk factors of acute radiation pneumonia caused by three-dimensional conformal radiotherapy for esophageal cancer in the elderly patients[J]. Zhongguo Lao Nian Xue Za Zhi, 2015, 35(2): 486-488.] |
| [5] |
Lu C, Lei Z, Wu HB, et al. Evaluating risk factors of radiation pneumonitis after stereotactic body radiation therapy in lung tumor: meta-analysis of 9 observational studies[J]. PLoS One, 2018, 13(12): e0208637. DOI:10.1371/journal.pone.0208637 |
| [6] |
Tsujino K, Tekatli H, Shimada T, et al. Combinedanalysis of V20, VS5, pulmonary fibrosis score on baseline computed tomography, and patient age improves prediction of severe radiation pneumonitis after concurrent chemoradiotherapy for locally advanced nonsmall-cell lung cancer[J]. J Thorac Oncol, 2014, 9: 983-990. DOI:10.1097/JTO.0000000000000187 |
| [7] |
Boyle J, Ackerson B, Gu L, et al. Dosimetric advantages of intensity modulated radiation therapy in locally advanced lung cancer[J]. Adv Radiat Oncol, 2017, 2(1): 6-11. DOI:10.1016/j.adro.2016.12.006 |
| [8] |
Tekatli H, Duijm M, Oomen-de Hoop E, et al. Normal tissue complication probability modeling of pulmonary toxicity after stereotactic and hypofractionated radiation therapy for central lung tumors[J]. Int J Radiation Oncol Biol Phys, 2018, 100(3): 738-747. DOI:10.1016/j.ijrobp.2017.11.022 |
| [9] |
李晔雄. 肿瘤放射治疗学[M]. 5版. 北京: 中国协和医科大学出版社, 2018: 790. [Li YX. Radiation Oncology[M]. 5th. Edition. Beijing: Peking Union Medical College Press, 2018: 790.]
|
| [10] |
National Cancer Institute (NIH). Common Terminology Criteria for Adverse Events (CTCAE)[EB/OL]. (2018-01-25). https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm#ctc_50.
|
| [11] |
Huang Y, Zhang W, Yu F, et al. The cellular and molecular mechanism of radiation-induced lung injury[J]. Med Sci Monit, 2017, 23: 3446-3450. DOI:10.12659/MSM.902353 |
| [12] |
Yorke ED, Jackson A, Rosenzsweig KE, et al. Dose-volume factors contributing to the incidence of radiation pneumonitis in non-small cell lung cancer patients treated with three-dimensional conformal radiation therapy[J]. Int J Radiat Oncol Biol Phys, 2002, 54(2): 329-339. |
| [13] |
Marks LB, Bentzen SM, Deasy JO, et al. Radiation dose-volume effects in the lung[J]. Int J Radiat Oncol Biol Phys, 2010, 76(3 Suppl): S70-S76. |
| [14] |
Palma DA, Senan S, Tsujino K, et al. Predicting radiation pneumonitis after chemoradiation therapy for lung cancer: An international individual patient data meta-analysis[J]. Int J Radiat Oncol Biol Phys, 2013, 85(2): 444-450. DOI:10.1016/j.ijrobp.2012.04.043 |
| [15] |
Roman MA, Rossiter HB, Casaburi R. Exercise, ageing and the lung[J]. Eur Respir J, 2016, 48(5): 1471-1486. DOI:10.1183/13993003.00347-2016 |
| [16] |
Deng G, Liang N, Xie J, et al. Pulmonary toxicity generated from radiotherapeutic treatment of thoracic malignancies[J]. Oncol Lett, 2017, 14(1): 501-511. DOI:10.3892/ol.2017.6268 |
| [17] |
Graves PR, Siddiqui F, Anscher MS, et al. Radiation pulmonary toxicity: from mechanisms to management[J]. Semin Radiat Oncol, 2010, 20(3): 201-207. DOI:10.1016/j.semradonc.2010.01.010 |
| [18] |
Liang B, Tian Y, Chen X, et al. Prediction of radiation pneumonitis with dose distribution: a convolutional neural network (CNN) based model[J]. Front Oncol, 2020, 9: 1500. DOI:10.3389/fonc.2019.01500 |
| [19] |
Cui Z, Tian Y, He B, et al. Associated factors of radiation pneumonitis induced by precise radiotherapy in 186 elderly patients with esophageal cancer[J]. Int J Clin Exp Med, 2015, 8(9): 16646-16651. |
| [20] |
Kong M, Lim YJ, Kim Y, et al. Diabetes mellitus is a predictive factor for radiation pneumonitis after thoracic radiotherapy in patients with lung cancer[J]. Cancer Manag Res, 2019, 11: 7103-7110. DOI:10.2147/CMAR.S210095 |
| [21] |
Wen G, Tan YT, Lan XW, et al. New clinical features and dosimetric predictor identification for symptomatic radiation pneumonitis after tangential irradiation in breast cancer patients[J]. J Cancer, 2017, 8(18): 3795-3802. DOI:10.7150/jca.21158 |
| [22] |
Tonison JJ, Fischer SG, Viehrig M, et al. Radiation pneumonitis after intensity-modulated radiotherapy for esophageal cancer: institutional data and a systematic review[J]. Sci Rep, 2019, 9(1): 2255. DOI:10.1038/s41598-018-38414-5 |
| [23] |
Skloot GS. The effects of aging on lung structure and function[J]. Clin Geriatr Med, 2017, 33(4): 447-457. DOI:10.1016/j.cger.2017.06.001 |
| [24] |
Lan K, Zhu J, Zhang J, et al. Propensity score-based comparison of survival and radiation pneumonitis after definitive chemoradiation for esophageal cancer: Intensity-modulated radiotherapy versus three-dimensional conformal radiotherapy[J]. Radiother Oncol, 2020, 149: 228-235. DOI:10.1016/j.radonc.2020.05.036 |
| [25] |
Kumar G, Rawat S, Puri A, et al. Analysis of dose-volume parameters predicting radiation pneumonitis in patients with esophageal cancer treated with 3D-conformal radiation therapy or IMRT[J]. Jpn J Radiol, 2012, 30(1): 18-24. DOI:10.1007/s11604-011-0002-2 |
| [26] |
Lin JB, Hung LC, Cheng CY, et al. Prognostic significance of lung radiation dose in patients with esophageal cancer treated with neoadjuvant chemoradiotherapy[J]. Radiat Oncol, 2019, 14(1): 85. DOI:10.1186/s13014-019-1283-3 |
| [27] |
沈文斌, 祝淑钗, 高红梅, 等. 肺脏低剂量区体积预测食管癌三维适形放疗所致急性放射性肺炎的价值[J]. 中华肿瘤杂志, 2013, 35(1): 45-49. [Shen WB, Zhu SC, Gao HM, et al. Low dose volume histogram analysis of the lungs in prediction of acute radiation pneumonitis in patients with esophageal cancer treated with three-dimensional conformal radiotherapy[J]. Zhonghua Zhong Liu Za Zhi, 2013, 35(1): 45-49.] |
| [28] |
Zhao Y, Chen L, Zhang S, et al. Predictive factors for acute radiation pneumonitis in postoperative intensity modulated radiation therapy and volumetric modulated arc therapy of esophageal cancer[J]. Thorac Cancer, 2015, 6(1): 49-57. DOI:10.1111/1759-7714.12142 |
| [29] |
杜峰, 王强, 王玮, 等. 胸段食管癌放疗后放射性肺炎相关因素分析[J]. 中华放射医学与防护杂志, 2020, 40(11): 832-839. [Du F, Wang Q, Wang W, et al. Analysis of related factors of radiation pneumonitis after radiotherapy for thoracic segment esophageal cancer[J]. Zhonghua Fang She Yi Xue Yu Fang Hu Za Zhi, 2020, 40(11): 832-839.] |
| [30] |
姚波, 王雅棣, 刘清志, 等. 肺癌与食管癌螺旋断层放疗致放射性肺炎的临床观察[J]. 临床肿瘤学杂志, 2014, 19(1): 52-56. [Yao B, Wang YL, Liu QZ, et al. Radiation pneumonitis in patients with lung cancer and esophageal cancer treated by helical tomotherapy[J]. Lin Chuang Zhong Liu Xue Za Zhi, 2014, 19(1): 52-56.] |