 2020, Vol. 47
2020, Vol. 47文章信息
- 阳性淋巴结对数比在胸段食管鳞癌患者长期预后中的预测作用
- Role of Log Odds of Positive Lymph Nodes in Predicting Long-term Prognosis of Patients with Thoracic Esophageal Squamous Cell Carcinoma
- 肿瘤防治研究, 2020, 47(3): 185-189
- Cancer Research on Prevention and Treatment, 2020, 47(3): 185-189
- http://www.zlfzyj.com/CN/10.3971/j.issn.1000-8578.2020.19.0417
- 收稿日期: 2019-03-29
- 修回日期: 2019-10-10
引用本文 |



2. 050011 石家庄,河北医科大学第四医院放疗科
2. Department of Radiotherapy, The Fourth Hospital of Hebei Medical University, Shijiazhuang 050011, China
食管癌为我国高发消化道恶性肿瘤,中晚期食管癌的治疗仍是以手术为主的综合治疗[1]。目前,临床上对于预测食管癌术后患者预后的指标中淋巴结状态最常用且最具有临床意义。但由于目前食管癌术式未统一,各肿瘤治疗中心在术中清扫淋巴结数目及临床送检病理淋巴结检测数目上存在较大差异,因此相同pN分期的患者可能预后相差较大。据既往研究报道,阳性淋巴结对数比(log odds of positive lymph nodes, LODDS)可以有效预测非小细胞肺癌、壶腹癌、直肠癌及乳腺癌等实体肿瘤的预后[2-5],且在食管癌术后患者预后的预测方面亦有相关报道[6-8],本研究旨在进一步明确LODDS能否在淋巴结阴性和术中淋巴结清扫数目不够的食管癌术后患者中显示出较好的预测功能,以便指导此部分患者术后治疗方案的制定。
1 资料与方法 1.1 临床资料收集2007年1月至2010年12月于河北医科大学第四医院胸外科接受根治性手术的731例胸段食管鳞癌(thoracic esophageal squamous cell carcinoma, TESCC)患者的临床病理资料,年龄37~80岁,平均年龄62岁;左侧开胸676例,其他术式55例(其中19例为右侧开胸,16例为颈腹两切口,另20例为颈+右胸+腹部三切口);手术清除淋巴结数目为6 566枚,平均9.0枚/例,见表 1。
|
(1)患者临床、病理和随访资料齐全;(2)术前均未行新辅助治疗及其他肿瘤相关的治疗;(3)术后未接受辅助治疗;(4)围手术期死亡患者排除在外;(5)术前辅助检查和术后病理证实无远处转移。
1.3 LODDS的计算公式[2]LODDS=Log(阳性淋巴结数+0.5)/(阴性淋巴结数+0.5)。
1.4 随访方法随访方式以电话随访、门诊复查为主,结合病例资料查阅。自患者手术之日起,随访截止日期为2019年1月31日,患者第1年每3~6月复查一次,随后每6~12月复查一次,失访32例,随访率95.6%,失访病例按死亡统计以末次随访日期作为死亡日期。
1.5 统计学方法应用SPSS19.0软件进行统计分析。应用Spearman分析方法进行相关性分析,应用受试者工作特征(receive operating characteristic, ROC)曲线及曲线下面积(AUC)确定LODDS的最佳截点(灵敏度与特异度之和最大点即约登指数最大点)。采用Log rank检验和Kaplan-Meier法进行单因素生存分析,采用Cox比例风险模型进行多因素分析。检验水准α=0.05, P < 0.05为差异有统计学意义。
2 结果 2.1 与LODDS相关指标的相关性分析结果显示LODDS与阳性淋巴结个数正相关(r=0.696, P=0.000),与术中清扫淋巴结数目显著性负相关(r=-0.530, P=0.000)。
2.2 LODDS的ROC曲线分析全组患者LODDS中位数为-1.114(-1.814~1.279),当LODDS为-1.028时,其约登指数最大(1.310),以此为最佳截点值,评估全组患者预后的敏感度为79.7%,特异度为52.3%,此时ROC曲线下面积为0.680(95%CI: 0.642~0.718),P=0.000。以阳性淋巴结数目预测本研究组患者食管癌术后患者生存的ROC曲线下面积为0.666,AUC小于LODDS,但差异无统计学意义,见图 1。

|
| 图 1 食管鳞癌根治术后患者LODDS的ROC曲线图 Figure 1 ROC curves of LODDS of esophageal cancer patients after radical surgery |
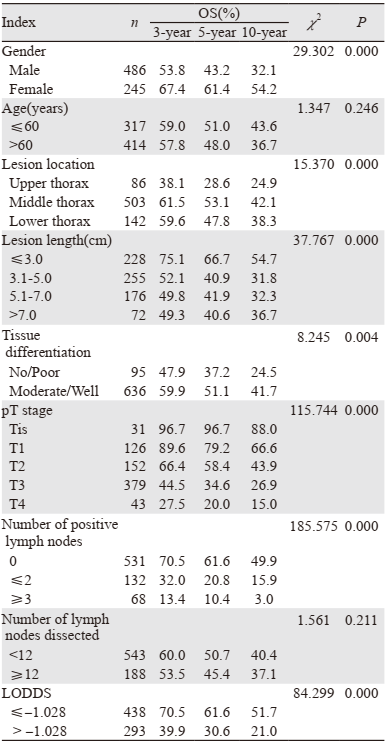
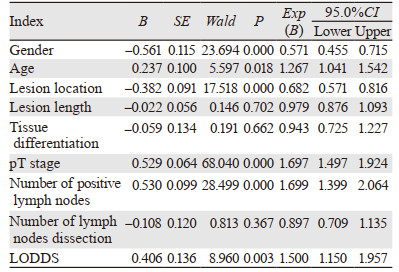
全组患者3、5、10年OS分别为58.3%、49.3%和39.4%,中位生存59.0月(95%CI: 47.58~70.42)。单因素分析结果显示:性别、食管病变部位、食管病变长度、组织分化程度、pT分期、阳性淋巴结个数和LODDS值为患者的预后影响因素(χ2=29.302、15.370、37.767、8.245、115.744、185.575、84.299, 均P < 0.005),见表 1。多因素分析结果显示:性别、年龄、食管病变部位、pT分期、阳性淋巴结个数和LODDS值为患者的独立预后影响因素(P < 0.05),见表 2。
|
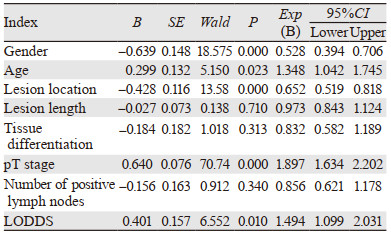
本组731例患者中术后病理显示淋巴结阴性患者为531例,Cox多因素分析结果显示:性别、年龄、食管病变部位、pT分期和LODDS值为患者的独立预后影响因素(P < 0.05),见表 3。
|
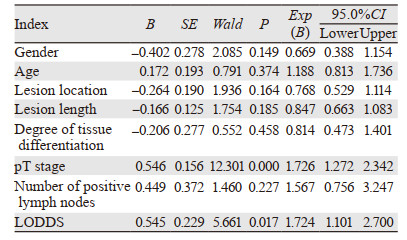
731例患者中543例术中清扫淋巴结数目 < 12枚,188例≥12枚。Cox多因素分析结果显示:性别、年龄、食管病变部位、pT分期、阳性淋巴结数目和LODDS值为术中清扫淋巴结数目≥12枚患者的独立预后影响因素(P < 0.05),见表 4。pT分期和LODDS值为术中清扫淋巴结数目 < 12枚患者的独立预后影响因素(P < 0.05),见表 5。

|
|
淋巴结转移为食管癌术后患者预后不良的重要指标,目前国际抗癌联盟(Union for International Cancer Control, UICC)的食管癌术后病理TNM分期中的N分期主要依据阳性淋巴结转移个数来定义,但由于各研究中心的食管癌手术方式有差异,导致术中淋巴结清扫数目不同而容易引起分期偏倚,另外由于临床送检淋巴结数目的不足也可能造成pN分期准确性降低[9],以上情况均可导致N分期相同的情况下患者生存差异明显不同。因此,有研究提出可将术前血小板与淋巴细胞比值和中性粒细胞与淋巴细胞比值作为食管癌患者的预后指标[10]。LODDS为阳性淋巴结对数比,其公式内既包含有阳性淋巴结,又含有阴性淋巴结,也将清扫淋巴结数目纳入了范围,有报道认为LODDS可以在一定程度上克服术中淋巴结清扫数目不足,从而可以弥补pN分期的缺陷[11],而且LODDS也可以很好地预测淋巴结阴性的食管癌术后患者的预后[7, 12-13]。本研究对731例食管鳞癌术后患者进行了回顾性分析,单因素分析结果显示LODDS值为患者的预后影响因素,多因素分析显示LODDS值为全组患者的独立性预后影响因素,依据ROC曲线分析LODDS的临界值取-1.028时,曲线下面积最大,且LODDS值越大,患者预后越差,同时证实LODDS可以预测术后病理淋巴结阴性患者和清扫淋巴结数目 < 12枚患者的预后。
Yang等[7]对260例食管鳞癌术后患者的预后进行了分析,结果亦显示LODDS越大,预后越差,多因素分析显示LODDS是所有患者的独立和重要预后因素(HR=1.309, P=0.003),且为淋巴结阴性患者的独立性预后影响因素(HR=1.610, P=0.038),由此认为LODDS可用于评估无淋巴结转移的晚期食管鳞癌术后患者OS。汪亮等[11]回顾性分析了905例pT3期食管鳞癌术后患者,以评价淋巴结转移数目、淋巴结转移率(MLR)和LODDS为基础的不同分期在预测患者预后中的价值,认为LODDS分期是pT3期食管鳞癌术后患者的独立预后因素,且LODDS分期对食管癌患者预后的预测价值或优于以pN分期为基础的TNM分期。杨明建等[12]分析了LODDS对136例pN0期胸段食管鳞癌术后患者预后的评估价值,结果显示-1.2为LODDS最佳截点值,LODDS值越大的患者预后越差(5年OS为48.3% vs. 29.7%, P=0.026),肿瘤复发和LODDS > -1.2为此组患者的独立性预后影响因素,他们认为对于淋巴结阴性的胸段食管鳞癌术后患者,LODDS分期具有预测预后的独特优势。Wu等[13]比较了LODDS、阳性淋巴结数目(pN)、淋巴结转移率(LNR)、淋巴结清除数目(RLN)和阴性淋巴结数目(NLN)对食管鳞癌术后患者的预测效能,研究共纳入589例患者,结果表明pN、LNR、RLN及NLN与LODDS均显著相关(P < 0.05),多因素分析结果显示LODDS为该组患者的独立性预后影响因素(HR=3.297, 95%CI: 2.684~4.050, P < 0.001),他们认为对于食管癌术后患者改良的LODDS分期系统对患者的预测效果优于以上其他淋巴结分期系统,并建议将LODDS纳入食管分期系统。以上结论与本研究的结论相似。
目前,我国食管癌的术式主要包括左侧开胸入路和右侧开胸入路,不同开胸模式的术中淋巴结清扫范围和程度有差异[14-15],毛友生等[14]对559例食管癌术后患者进行了不同手术入路对预后影响的研究,接受左、右胸入路的患者分别为282和277例,术中平均清扫淋巴结分别为23.4和24.6枚(P < 0.001)、胸部淋巴结转移率分别为34.8%和50.5%(P < 0.001)、腹部淋巴结的转移率分别为29.1%和17.7%(P=0.001)、5年生存率分别为38.2%和42.1%(P=0.620)。Li等[16]对300例胸中、下段食管癌术后患者的不同术式进行了比较,结果显示左胸入路和右胸入路的平均术中淋巴结清扫数目分别为18和22枚(P < 0.001),遗憾的是该研究未对患者预后进行比较。这种差异与食管癌病变部位亦有关联[17]。本组患者中接受左侧开胸术为676例,占92.5%,依据上述报道,对本组患者采用LODDS来评估患者预后可能更有效,且本研究结果显示无论对于全组患者、淋巴结阴性患者或清扫淋巴结数目 < 12枚的患者,LODDS均为独立性预后因素。
综上所述,LODDS可作为术后淋巴结阴性、术中淋巴结清扫数目不足等不同类型的胸段食管鳞癌术后患者的独立性预后指标,建议临床医师在制定胸段食管鳞癌术后患者治疗计划时将LODDS作为重要预后参考指标,以制定个体化治疗方案,改善患者预后。
作者贡献
高红梅:课题设计、临床资料收集及论文撰写
池书平:病例收集、随访和统计学处理
沈文斌:课题设计、统计学指导和论文修改
| [1] |
Taylor LJ, Greenberg CC, Lidor AO, et al. Utilization of surgical treatment for local and locoregional esophageal cancer: analysis of the National Cancer Data Base[J]. Cancer, 2017, 123(3): 410-419. DOI:10.1002/cncr.30368 |
| [2] |
Wen J, Ye F, He X, et al. Development and validation of a prognostic nomogram based on the log odds of positive lymph nodes (LODDS) for breast cancer[J]. Oncotarget, 2016, 7(15): 21046-21053. DOI:10.18632/oncotarget.8091 |
| [3] |
Agalar C, Aysal A, Unek T, et al. The Role of Log Odds of Positive Lymph Nodes in Predicting the Survival after Resection for Ampullary Adenocarcinoma[J]. Pathol Oncol Res, 2019. [Epub ahead of print] http://link.springer.com/article/10.1007/s12253-019-00584-6
|
| [4] |
Dziedzic D, Piotr R, Langfort R, et al. Log odds of positive lymph nodes as a novel prognostic indicator in NSCLC staging[J]. Surg Oncol, 2017, 26(1): 80-85. DOI:10.1016/j.suronc.2017.01.004 |
| [5] |
Huang B, Chen C, Ni M, et al. Log odds of positive lymph nodes is a superior prognostic indicator in stage Ⅲ rectal cancer patients: A retrospective analysis of 17, 632 patients in the SEER database[J]. Int J Surg, 2016, 32: 24-30. DOI:10.1016/j.ijsu.2016.06.002 |
| [6] |
Sun Z, Xu Y, Li de M, et al. Log odds of positive lymph nodes:a novel prognostic indicator superior to the number based and the ratio-based N category for gastric cancer patients with R0 resection[J]. Cancer, 2010, 116(11): 2571-2580. DOI:10.1002/cncr.24989 |
| [7] |
Yang M, Zhang H, Ma Z, et al. Log odds of positive lymph nodes is a novel prognostic indicator for advanced ESCC after surgical resection[J]. J Thorac Dis, 2017, 9(5): 1182-1189. DOI:10.21037/jtd.2017.03.187 |
| [8] |
Cao J, Yuan P, Ma H, et al. Log Odds of Positive Lymph Nodes Predicts Survival in Patients After Resection for Esophageal Cancer[J]. Ann Thorac Surg, 2016, 102(2): 424-432. DOI:10.1016/j.athoracsur.2016.03.030 |
| [9] |
Twine CP, Lewis WG, Morgan MA, et al. The assessment of prognosis of surgically resected oesophageal cancer is dependent on the number of lymph nodes examined pathologically[J]. Histopathology, 2009, 55(1): 46-52. DOI:10.1111/j.1365-2559.2009.03332.x |
| [10] |
张思思, 袁来. 术前血小板与淋巴细胞比值和中性粒细胞与淋巴细胞比值对食管癌预后的预测价值[J]. 肿瘤防治研究, 2017, 44(12): 811-815. [Zhang SS, Yuan L. Preoperative platelet-to-lymphocyte ratio and neutrophil-to-lymphocyto ratio for predicting prognosis of esophageal cancer patients[J]. Zhong Liu Fang Zhi Yan Jiu, 2017, 44(12): 811-815. DOI:10.3971/j.issn.1000-8578.2017.17.0547] |
| [11] |
汪亮, 蔡磊, 陈倩, 等. pN分期淋巴结转移率分期和阳性淋巴结对数比分期预测T3期食管鳞癌患者预后的价值[J]. 中华肿瘤杂志, 2017, 39(10): 749-753. [Wang L, Cai L, Chen Q, et al. Prognostic value of three different staging schemes based on pN, MLR and LODDS in patients with T3 esophageal cancer[J]. Zhonghua Zhong Liu Za Zhi, 2017, 39(10): 749-753. DOI:10.3760/cma.j.issn.0253-3766.2017.10.006] |
| [12] |
杨明建, 张洪典, 霍小东, 等. 阳性淋巴结对数比对pN0期胸段食管鳞癌术后患者预后的评估价值[J]. 中华胃肠外科杂志, 2016, 19(5): 535-539. [Yang MJ, Zhang HD, Huo XD, et al. Predictive value of log odds of positive lymph nodes for the prognosis of patients with node-negative squamous cell carcinoma of the thoracic esophagus after radical esophagectomy[J]. Zhonghua Wei Chang Wai Ke Za Zhi, 2016, 19(5): 535-539. DOI:10.3760/cma.j.issn.1671-0274.2016.05.013] |
| [13] |
Wu SG, Sun JY, Yang LC, et al. Prognosis of patients with esophageal squamous cell carcinoma after esophagectomy using the log odds of positive lymph nodes[J]. Oncotarget, 2015, 6(34): 36911-36922. DOI:10.18632/oncotarget.5366 |
| [14] |
毛友生, 赫捷, 董静思, 等. 胸段食管癌左右胸入路清扫淋巴结的结果比较[J]. 中华肿瘤杂志, 2012, 34(4): 296-300. [Mao YS, He J, Dong JS, et al. Comparison of the results of lymph node dissection via left versus right thoracotomy[J]. Zhonghua Zhong Liu Za Zhi, 2012, 34(4): 296-300. DOI:10.3760/cma.j.issn.0253-3766.2012.04.013] |
| [15] |
Tanaka Y, Ueno T, Yoshida N, et al. The effect of an elemental diet on oral mucositis of esophageal cancer patients treated with DCF chemotherapy: a multi-center prospective feasibility study (EPOC study)[J]. Esophagus, 2018, 15(4): 239-248. DOI:10.1007/s10388-018-0620-1 |
| [16] |
Li B, Xiang J, Zhang Y, et al. Comparison of Ivor-Lewis vs Sweet esophagectomy for esophageal squamous cell carcinoma: a randomized clinical trial[J]. JAMA Surg, 2015, 150(4): 292-298. DOI:10.1001/jamasurg.2014.2877 |
| [17] |
许茜, 刘志坤, 曹彦坤, 等. 食管癌大体肿瘤靶区体积与淋巴结转移及预后的关系[J]. 中华肿瘤杂志, 2012, 34(9): 684-687. [Xu Q, Liu ZK, Cao YK, et al. Relationship of gross tumor volume with lymph node metastasis and prognosis of esophageal carcinoma[J]. Zhonghua Zhong Liu Za Zhi, 2012, 34(9): 684-687. DOI:10.3760/cma.j.issn.0253-3766.2012.09.009] |