 2019, Vol. 46
2019, Vol. 46文章信息
- 腹部纤维母细胞/肌纤维母细胞性肿瘤的PET/CT影像学特点及其应用价值
- PET/CT Imaging Characteristics of Abdominal Fibroblastic/Myofibroblastic Tumors and Its Application Value
- 肿瘤防治研究, 2019, 46(3): 243-247
- Cancer Research on Prevention and Treatment, 2019, 46(3): 243-247
- http://www.zlfzyj.com/CN/10.3971/j.issn.1000-8578.2019.18.1817
- 收稿日期: 2018-11-19
- 修回日期: 2019-01-02
引用本文 |



纤维母细胞/肌纤维母细胞性肿瘤是软组织肿瘤中的一类,是一种比较少见的间叶源性肿瘤,包含良性、中间型、恶性三大类[1],发生于腹部的较为少见,国内外关于此类肿瘤的PET/CT报道不多,多为个案报道[2-5],本研究对28例患者的PET/CT图像进行回顾性分析,总结影像学表现的差异,以提高对该病变的认识。
1 资料与方法 1.1 一般资料搜集2010年1月—2018年10月经我院腹膜后与软组织肿瘤中心治疗的腹部纤维母细胞/肌纤维母细胞性肿瘤患者28例,包括初治与复发患者,所有病例经手术或穿刺病理证实并于手术或穿刺前后2周内行PET/CT检查。
1.2 PET/CT成像方法18F-FDG PET/CT扫描采用飞利浦公司PET/CT显像仪(Gemini TF 16, Philips, 荷兰),其中PET/CT部分采用LYSO晶体和微电子设备,CT为16排高分辨螺旋CT。所有患者检查前均空腹6 h以上,测定患者空腹血糖水平 < 10 mmol/L。按患者体重(3.0~3.7 MBq/kg)静脉注射18F-FDG后,患者平静休息,60 min左右行颅脑及躯干部PET/CT图像采集。躯干部PET采集1分钟/床位,9或10床位; 头部PET:7~10分钟/床位,1床位。衰减校正平扫CT:120 kV,100 mAs; OSEM法重建(重建层厚3 mm)。
1.3 图像分析由两名核医学主治医师以上职称的医师利用Philips GEMINI TR16软件共同阅片。分析肿瘤的PET/CT表现,包括局部浸润情况,肿瘤边缘模糊被认为浸润周围脂肪组织,肿瘤推及压迫周围组织无明显脂肪间隙被认为可疑脏器浸润,肿瘤侵及脏器与之无分界被认为脏器浸润,另外分析淋巴结及远处转移情况。选取病灶中实性成分勾画ROI进行SUVmax测量。
1.4 统计学方法采用SPSS17.0软件进行数据统计分析,统计学方法采用t检验、单因素方差分析,P < 0.05为差异有统计学意义。
2 结果 2.1 患者一般情况28例患者中,男17例,女11例,年龄23~66岁,平均47岁。28例患者中,中间型组26例,包括:13例侵袭性纤维瘤病(aggressive fibromatosis, AFT)(原发9例、复发4例)、10例孤立性纤维性肿瘤(solitary fibrous tumors, SFT)(原发6例、复发4例)和3例炎性肌纤维母细胞瘤(inflammatory myofibroblastic tumors, IMT)(原发2例、复发1例),恶性组2例:原发纤维肉瘤(fibrosarcoma, FSC)2例。21例接受手术治疗,7例未手术。
2.2 肿瘤的PET/CT表现病灶均表现为肿块,16例位于腹腔内,12例位于腹膜后。病灶多较大,平均直径为12.4 cm。原发病灶与复发病灶直径大小无明显差异(12.93±5.85 vs. 11.15±7.0, P > 0.05),病灶直径与SUVmax间无相关性(P > 0.05)。19例原发病灶中,17例单发,2例多发; 9例复发病例中,4例单发,5例多发。病灶表现为软组织肿块,密度多不均匀,1例SFT及1例IMT可见出血,1例AFT、1例SFT、2例IMT、2例FSC可见肿瘤坏死,表现为放射性稀疏的低密度区。中间型的肿瘤伴轻度代谢,SUVmax为2.2~11.7,平均值为4.5,纤维肉瘤伴明显高代谢,SUVmax为9.9~25.9,平均值为17.9,见表 1、图 1~4。

|

|
| A: PET image; B: CT image; C: PET/CT fusion image; 1: coronal image; 2: sagittal image; 3: axial image; A 52-year-old female patient was with a large retroperitoneal soft tissue mass, with a diameter of 15.3cm and SUVmax 6.4. There was no distinct demarcation between the mass and the left iliac artery or ureter. Postoperative pathology was retroperitoneal aggressive fibromatosis. The tumor invaded the iliac artery, iliac vein, ureter and mesentery. 图 1 1例腹膜后侵袭性纤维瘤病PET/CT图像 Figure 1 PET/CT image of one case of retroperitoneal aggressive fibromatosis |

|
| A: PET image; B: CT image; C: PET/CT fusion image; 1: coronal image; 2: sagittal image; 3: axial image; A 58 years old male patient was with a right retroperitoneal solitary soft tissue mass, with a diameter of 17.7cm and SUVmax 4.2, blurred margin. Postoperative pathology showed solitary fibrous tumors, invading mesocolon sigmoides 图 2 1例孤立性纤维性肿瘤PET/CT图像 Figure 2 PET/CT image of one case of solitary fibrous tumor |

|
| A: PET image; B: CT image; C: PET/CT fusion image; 1: coronal image; 2: sagittal image; 3: axial image; A 33-year-old male patient was with a soft tissue mass in the left abdominal cavity, with a diameter of 10.9cm and SUVmax 2.2. There was high-density hemorrhage with no distinct demarcation from the gastric wall. Postoperative pathology showed inflammatory myofibroblastoma involving the serosa and muscularis propria of the gastric wall. 图 3 1例炎性肌纤维母细胞瘤的PET/CT图像 Figure 3 PET/CT image of one case of inflammatory myofibroblastoma |

|
| A: PET image; B: CT image; C: PET/CT fusion image; 1: coronal image; 2: sagittal image; 3: axial image; A 39-year-old male patient was with a soft tissue mass in the left abdominal cavity, with a diameter of 13.3 cm and SUVmax 25.9. There was a low-density necrosis area in the tumor. There was no obvious demarcation between the tumor and the right iliopsoas. Postoperative pathology showed fibrosarcoma which invaded the surrounding skeletal muscle, ileocecal region and the ureter 图 4 1例纤维肉瘤的PET/CT图像 Figure 4 PET/CT image of one case of fibrosarcoma |
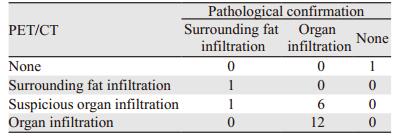
PET/CT可清楚显示肿瘤与周围组织的关系,21例有手术病理结果的病例中(AFT 9例、SFT 7例、IMT 3例、FSC 2例),1例孤立性纤维性肿瘤边缘光滑无周围脂肪浸润,1例孤立性纤维性肿瘤边缘模糊浸润周围脂肪,同病理结果一致,7例PET/CT可疑脏器浸润中1例脂肪浸润、6例脏器浸润,余12例PET/CT判断脏器浸润的同术后病理一致。28例患者PET/CT均未见淋巴结转移,21例经病理证实。4例患者出现远处病灶,其中1例侵袭性纤维瘤病发现肺占位,根据PET/CT表现疑诊原发肺癌,后经病理证实,1例恶性孤立性纤维性肿瘤肝肺转移、1例恶性孤立性纤维性肿瘤骶骨转移、1例纤维肉瘤双肺转移,见表 2、图 5~6。
|

|
| A: axis PET; B: window CT; C: PET/CT fusion image; D: PET MIP image 图 5 1例复发恶性孤立性纤维性肿瘤骶骨转移 Figure 5 One case of recurrent malignant solitary fibrous tumor with sacral metastasis |

|
| A: axis PET; B: window CT; C: PET/CT fusion image; D: PET MIP image 图 6 1例原发恶性孤立性纤维性肿瘤肺转移 Figure 6 One case of primary malignant solitary fibrous tumor with pulmonary metastasis |
原发与复发的中间型纤维性肿瘤SUVmax差异无统计学意义(4.15±2.2 vs. 5.03±2.35, P > 0.05),但均低于纤维肉瘤(17.9±11.31, P=0.001)。按病理类型分,纤维瘤病、孤立性纤维性肿瘤、肌纤维母细胞瘤三种中间型肿瘤的SUVmax差异无明显统计学意义(4.87±2.17, 3.56±0.95, 5.63±4.86, P > 0.05),但均低于纤维肉瘤(17.9±11.31, P=0.001),见图 7~8。

|
| AFT: aggressive fibromatosis; SFT: solitary fibrous tumors; IMT: inflammatory myofibroblastic tumors; FSC: fibrosarcoma; There was no difference in SUVmax among the three intermediate tumors, but they were lower than that of fibrosarcoma 图 7 四种纤维性肿瘤的SUVmax值 Figure 7 SUVmax of four fibrous tumors |

|
| PIT: primary intermediate tumor; RIT: recurrent intermediate tumor; PMT: primary malignant tumor; There was no difference in SUVmax between primary and recurrent intermediate tumors, but both of them were lower than that of primary malignant tumors 图 8 原发、复发中间型肿瘤与原发恶性肿瘤的SUVmax值 Figure 8 SUVmax of primary intermediate tumor, recurrent intermediate tumor and primary malignant tumor |
发生于腹部者主要为中间型肿瘤及恶性肿瘤,未见良性肿瘤。AFT呈侵袭性生长及局部易复发的特征,但不发生远处转移。镜下显示由不同形态的梭形、细长、肥胖的纤维母细胞组成,衬在一个包含许多血管的黏液样结构、血管周围胶质间质背景。免疫组织化学显示强表达波形蛋白,而肌纤维母细胞还不同程度地表达平滑肌肌动蛋白(SMA)[2-5]。发生于腹部的少见SFT肉眼观为孤立性软组织肿块,质韧,与周围组织境界清楚,多数呈良性肿瘤征象。镜下肿瘤主要为无异型性的梭形细胞,可见致密胶原纤维及黏液变性区,瘤内血管丰富,部分肿瘤间质内纤维组织增生。目前研究认为大多数SFTs均CD34阳性,但CD34的阳性表达率与肿瘤的分化有关,恶性SFTs的CD34阳性表达率低[6-8]。SMA阳性反应被认为是IMT的重要标志[9]。AFT和SFT在CT和MRI增强扫描常表现为渐进性明显强化,坏死少见[10-11],IMT影像学表现缺乏特异性征象,IMT内不同程度的纤维组织增生、炎性细胞浸润、凝固性坏死以及炎性过程中的动态变化是其影像表现多样性的病理基础,增强扫描呈均匀或不均匀中度至显著强化,无明显特异性表现[9],纤维肉瘤亦缺乏特征性表现,形态多不规则,浸润性生长,常伴有出血或坏死[12-13]。PET/CT通过CT密度及代谢情况亦可显示病灶的不均质性及其内的出血、坏死。本组病例1例AFT、1例SFT、2例IMT、2例FSC可见肿瘤坏死,与文献报道一致。腹部纤维母细胞/肌纤维母细胞性肿瘤体积多较大,中间型与恶性肿瘤均以浸润周围脏器为主(20/21),相对于肿瘤边界,肿瘤内的坏死与较高SUVmax值可能更有助于恶性程度的提示。
3.2 PET/CT检查的价值本组病例中间型的三种肿瘤纤维瘤病、孤立性纤维性肿瘤、肌纤维母细胞瘤的SUVmax无明显差异,但均低于恶性的纤维肉瘤,提示PET/CT于术前可以对肿瘤的恶性程度进行初判。
肿瘤的完全切除是目前治疗腹部及腹膜后间叶组织肿瘤的有效方法,联合脏器切除,能明显降低局部复发率、改善生存[14]。局部复发性肿瘤的治疗原则上与原发肿瘤相同。本组病例28例中21例行肿物联合脏器切除,其中有7例为复发后再次手术。术前PET/CT对于原发及复发肿瘤,均能明确显示病变范围、毗邻脏器、淋巴结及远处转移情况,有助于外科手术计划的制定。
本研究对少见的腹部纤维母细胞/肌纤维母细胞性肿瘤进行了较大样本量的总结,分析其PET/CT表现特点,提高了对该病的PET/CT影像学表现的认识,并讨论了PET/CT的应用价值。不足之处在于每种亚型的病例数尚较少,需进一步增加样本量进行更加细致的对比研究。
综上,腹部纤维母细胞/肌纤维母细胞性肿瘤可发生于腹腔及腹膜后, 病灶以局部浸润为主,少有淋巴结转移,罕见远处转移,恶性肿瘤代谢程度高于中间型的肿瘤代谢,PET/CT有助于术前肿瘤分期,SUVmax值可提示肿瘤恶性程度。
作者贡献
周妮娜:课题设计,病例资料收集,图像分析,论文写作; 于江媛:图像分析; 朱华:数据统计; 赵伟:图像采集及处理; 杨志:课题指导
| [1] | Fletchero CDM, Bridge JA, Hogendoorn PCW, et al. World Health Organization classification of soft tissue and bone tumours[M]. Lyon: IARCP Press, 2013: 10-238. |
| [2] | Lee JC, Thomas JM, Phillips S, et al. Aggressive fibromatosis:MRI features with pathologic correlation[J]. AJR Am J Roentgenol, 2006, 186(1): 247–54. DOI:10.2214/AJR.04.1674 |
| [3] | 邓新源, 梁菊香, 罗志程. 韧带样型纤维瘤病MR征象及病理[J]. 影像诊断与介入放射学, 2010, 19(4): 216–8. [ Deng XY, Liang JX, Luo ZC. Clinical, MR imaging and pathological features of desmoid-type fibromatosis[J]. Ying Xiang Zhen Duan Yu Jie Ru Fang She Xue, 2010, 19(4): 216–8. DOI:10.3969/j.issn.1005-8001.2010.04.009 ] |
| [4] | 彭俊萍, 张雪林, 吕晓飞, 等. 韧带样纤维瘤的影像表现与病理对照[J]. 临床放射学杂志, 2011, 30(8): 1166–9. [ Peng JP, Zhang XL, Lyu XF, et al. Imaging Findings of Desmoid Type Fibromatoses: Comparison with Pathological Results[J]. Lin Chuang Fang She Xue Za Zhi, 2011, 30(8): 1166–9. ] |
| [5] | 杨吉龙, 王坚, 朱雄增. 韧带样型纤维瘤病的病理学和遗传学研究进展[J]. 中华病理学杂志, 2005, 34(8): 537–9. [ Yang JL, Wang J, Zhu XZ. Progress in the research of pathology and genetics of desmoid tumor[J]. Zhonghua Bing Li Xue Za Zhi, 2005, 34(8): 537–9. DOI:10.3760/j.issn:0529-5807.2005.08.039 ] |
| [6] | Ginat DT, Bokhari A, Bhatt S, et al. Imaging features of solitary fibrous tumors[J]. AJR Am J Roentgenol, 2011, 196(3): 487–95. DOI:10.2214/AJR.10.4948 |
| [7] | 刘毅, 刘剑羽, 王宏磊, 等. 孤立性纤维瘤的影像表现[J]. 中华放射学杂志, 2012, 46(5): 441–4. [ Liu Y, Liu JY, Wang HL, et al. Imaging findings of solitary fibrous tumors[J]. Zhonghua Fang She Xue Za Zhi, 2012, 46(5): 441–4. DOI:10.3760/cma.j.issn.1005-1201.2012.05.014 ] |
| [8] | Nagasako Y, Misawa K, Kohashi S, et al. Solitary fibrous tumor in the retroperitoneum[J]. J Am Coll Surg, 2004, 198(2): 322–3. DOI:10.1016/j.jamcollsurg.2003.07.023 |
| [9] | 吕绍茂, 段少银, 韩丹, 等. 炎性肌纤维母细胞瘤影像学表现与病理学分析[J]. 中国临床医学影像杂志, 2010, 21(5): 331–4. [ Lv SM, Duan SY, Han D, et al. The imaging and pathology of inflammatory myofibroblastic tumor[J]. Zhongguo Lin Chuang Yi Xue Ying Xiang Za Zhi, 2010, 21(5): 331–4. DOI:10.3969/j.issn.1008-1062.2010.05.008 ] |
| [10] | 赵登玲, 邓钢, 张丽华, 等. 孤立性纤维瘤的影像学特征及良恶性对比分析[J]. 肿瘤, 2013, 33(5): 454–9. [ Zhao DL, Deng G, Zhang LH, et al. Solitary fibrous tumors: Imaging features and differentiation between benign and malignant tumors[J]. Zhong Liu, 2013, 33(5): 454–9. ] |
| [11] | 苏金亮, 周利民, 纪建松, 等. 侵袭性纤维瘤病的CT及MRI特征[J]. 放射学实践, 2011, 26(5): 497–500. [ Su JL, Zhou LM, Ji JS, et al. CT and MRI feaatures of abdominal aggresive fibromatosis[J]. Fang She Xue Shi Jian, 2011, 26(5): 497–500. DOI:10.3969/j.issn.1000-0313.2011.05.006 ] |
| [12] | 丁重阳, 李天女, 吉爱兵. 原发性腹膜后恶性肿瘤的18F-FDG PET/CT显像特征[J]. 中国临床医学影像杂志, 2014, 25(9): 674–6. [ Ding CY, Li TN, Ji AB. Manifestations of 18F-FDG PET/CT scanning in primary retroperitoneal malignant tumors[J]. Zhongguo Lin Chuang Yi Xue Ying Xiang Za Zhi, 2014, 25(9): 674–6. ] |
| [13] | Azadi J, Subhawong A, Durand DJ. F-18-FDG PET/CT and Tc-99m sulfur colloid SPECT imaging in the diagnosis and treatment of a case of dual solitary fibrous tumors of the retro peritoneum and pancreas[J]. J Radiol Case Rep, 2012, 6(3): 32–7. |
| [14] | Ballo MT, Zagars GK, Pollock RE, et al. Retroperitoneal soft tissue sarcoma: an analysis of radiation and surgical treatment[J]. Int J Radiat Oncol Biol Phys, 2007, 67(1): 158–63. DOI:10.1016/j.ijrobp.2006.08.025 |