 2019, Vol. 46
2019, Vol. 46文章信息
- 骨巨细胞瘤术后复发原因分析
- Risk Factors of Postoperative Recurrence for Giant Cell Tumor of Bone
- 肿瘤防治研究, 2019, 46(4): 345-349
- Cancer Research on Prevention and Treatment, 2019, 46(4): 345-349
- http://www.zlfzyj.com/CN/10.3971/j.issn.1000-8578.2019.18.1369
- 收稿日期: 2018-12-17
- 修回日期: 2019-01-10
引用本文 |



2. 350800 福州, 闽清县医院骨科
2. Department of Orthopaedics, Minqing County Hospital, Fuzhou 350800, China
骨巨细胞瘤(giant cell tumor, GCT)是青壮年高发的原发性骨肿瘤,亚洲人的发病率是欧美的3倍左右,呈局部侵袭性生长,进展快。因大多发病于大关节周围,大段切除后严重影响肢体功能,而常用的囊内刮除术复发率较高[1-2]。该病的生物学特性和预后多样,随着对该疾病的进一步认识和手术理念的更新,复发率逐渐下降[3-4]。现对本科室治疗的骨巨细胞瘤的病例进行分析,以探究发病部位、病理性骨折、手术方式、Campanacci分级、肺转移与骨巨细胞瘤术后复发率的相关性,报道如下。
1 资料与方法 1.1 一般资料选取2000年1月—2017年1月期间于福建医科大学附属第一医院骨科行手术治疗的骨巨细胞瘤患者486例为研究对象进行回顾性分析,所有患者术前均经病理诊断证实,同时收集患者肿瘤发病部位、病理性骨折、手术方式、Campanacci分级、肺转移等相关资料及数据。手术方式分为单纯刮除、扩大刮除和瘤段或分块切除。
1.2 手术方法 1.2.1 单纯刮除自肿瘤部位入路显露,有软组织肿块的包膜外显露,切除软组织肿块后骨性开窗,囊内彻底刮除病灶,苯酚酒精灭活囊腔,瘤腔内植骨或填充骨水泥,根据力学稳定性酌情应用内固定物。
1.2.2 扩大刮除在单纯刮除的基础上,高速磨钻再去除皮质骨 > 1 mm、松质骨 > 10 mm。
1.2.3 瘤段或分块切除肢体的骨巨细胞瘤行瘤段切除,切除范围为以MR信号异常为边界的瘤体外2 cm,酌情行自体骨移植、肿瘤型人工关节重建或旷置;脊柱骨盆的骨巨细胞瘤行分块切除或整块切除,根据力学稳定情况酌情使用钉棒系统固定或重建。
1.3 术后随访术后2年内每3月复诊,第3~5年每6月复诊,复查局部X线片和肺部CT,根据需要复查局部CT或MR,重点观察肢体功能、局部骨愈合、有无复发、假体或内固定物在位情况。
1.4 统计学方法采用SPSS19.0软件进行统计学处理,符合正态分布的计量资料以均数±标准差(x±s)表示。计数资料比较采用χ2检验或Fisher’s精确检验;两组间比较、三组间两两比较以及四组间两两比较分别以P < 0.05、P < 0.017和P < 0.013为差异有统计学意义。
2 结果 2.1 骨巨细胞瘤患者临床资料获得随访的患者451例,其中男178例,女273例,年龄12~54岁,平均(29.8±1.9)岁;各部位发病例数,见表 1;病理性骨折41例、无病理性骨折410例;初治者391例、复发再治者60例;行单纯刮除术者212例、扩大刮除术者185例、瘤段切除术者31例、分块切除术者23例;Campanacci分级分别为:Ⅰ级15例、Ⅱ级241例、Ⅲ级195例;截止至末次随访日期,12例出现肺转移,56例复发,总复发率12.4%,复发时间为3~60月,平均(11±2.1)月。
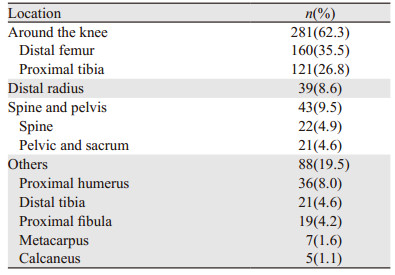
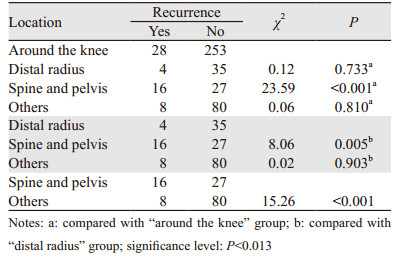
膝关节周围骨巨细胞瘤术后复发率为10%(28/281),桡骨远端骨巨细胞瘤术后复发率为10.3%(4/39),脊柱或骨盆骨巨细胞瘤术后复发率为37.2%(16/43),其他部位骨巨细胞瘤复发率为9.1%(8/88)。两两比较四组部位间骨巨细胞瘤术后复发率的差异,结果显示脊柱骨盆骨巨细胞瘤的复发率较其余三组高(P < 0.013),其余各组部位间的复发率差异无统计学意义(P > 0.013),见表 2。
|
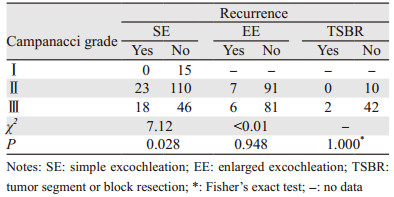
CampanacciⅠ级骨巨细胞瘤行单纯刮除术后均无复发;CampanacciⅡ级骨巨细胞瘤行单纯刮除术、扩大刮除术及瘤段或分块切除术后复发率分别为17.3%(23/133)、7.1%(7/98)、0(0/10);CampanacciⅢ级骨巨细胞瘤行单纯刮除术、扩大刮除术及瘤段或分块切除术后复发率分别为28.1%(18/64)、6.9%(6/87)、4.5%(2/44),见图 1~3。两两比较三种手术后复发率的差异,结果显示Ⅲ级骨巨细胞瘤单纯刮除术后复发率明显高于扩大刮除术(P < 0.001)以及瘤段或分块切除术(P=0.002),差异有统计学意义,而扩大刮除术与瘤段或分块切除术后复发率差异无统计学意义(P=0.885);Ⅱ级骨巨细胞瘤三种手术后复发率的差异无统计学意义(P > 0.017),见表 3。

|
| 图 1 骨巨细胞瘤扩大刮除术后复发病例X线结果 Figure 1 X-ray of one recurrence case with giant cell tumor of bone after enlarged excision |

|
| A 24-year-old male with giant cell tumor of bone in the left distal tibia suffered tumor recurrence 3 months after anterior approach surgery with simple excochleation and inactivation of bone graft because of exposure difficulty in the internal posterior side and insufficient scraping range; A: before operation; B: 3 months after surgery 图 2 骨巨细胞瘤单纯刮除术后复发病例CT结果 Figure 2 CT scan of one recurrence case with giant cell tumor of bone after simple excochleation |

|
| A 26-year-old female with giant cell tumor of bone in the 1st sacrum found no evidence of recurrence 53 months after surgery with the whole block below the 3rd sacrum resected and nerve-retained enlarged excochleation above the 3rd sacrum. A, B: preoperative CT scan; C: preoperative MRI; D: X-ray 53 months after surgery; E: CT scan 53 months after surgery 图 3 骨巨细胞瘤大块切除术后病例影像学检查结果 Figure 3 Imaging results of one case with giant cell tumor of bone after block resection |

|
Ⅰ级、Ⅱ级、Ⅲ级骨巨细胞瘤行单纯刮除术后复发率分别为0、17.3%(23/133)、28.1%(18/64),差异有统计学意义(P=0.028);Ⅱ级、Ⅲ级骨巨细胞瘤行扩大刮除术后复发率分别为7.1%(7/98)、6.9%(6/87),差异无统计学意义(P > 0.05);Ⅱ级、Ⅲ级骨巨细胞瘤行瘤段或分块切除术后复发率分别为0(0/10)、4.5%(2/44),差异无统计学意义(P > 0.05),见表 4。
|
术前发生病理性骨折患者术后复发率为12.2%(5/41),术前无病理性骨折者术后复发率为12.4%(51/410),差异无统计学意义(P > 0.05),见表 5。

|
获得随访的451病例中,总的肺转移率为2.7%(12/451)。其中无复发病例肺转移率为1.0%(4/395),复发病例肺转移率为14.3%(8/56),与无复发病例相比,复发病例肺转移率明显升高,差异有统计学意义(P < 0.001),见表 5。
3 讨论1818年Astlay Cooper首次描述骨巨细胞瘤,因为该肿瘤进展快,最初被认为是一种恶性肿瘤;随后有研究发现它并不像其他恶性肿瘤一样致命,部分患者可通过刮除植骨治愈,存活期长,有部分学者认为其是一种良性肿瘤,所以囊内刮除一直以来都是骨巨细胞瘤最常用的治疗方法,但复发率高达27%~54%[1-4]。文献报道有3%左右的骨巨细胞瘤是恶性的或逐渐恶性变,而且3%~5%的良性骨巨细胞瘤也可能发生肺部转移,所以最新的WHO骨肿瘤分类中骨巨细胞被定性为侵袭性或潜在恶性病变,是一种生物学行为不可预测的肿瘤[5-6]。
组织学研究表明,骨巨细胞瘤的细胞学成分有三种:梭形的基质细胞、圆形的单核细胞和破骨细胞样的多核细胞。目前观点认为,梭形的基质细胞才是骨巨细胞瘤真正意义上的肿瘤细胞,它起源于间充质干细胞,具有成骨活性,其发病机制是具有肿瘤活性的梭形基质细胞吸引血液系统的单核细胞,在局部形成破骨细胞样的多核细胞,产生溶骨性破坏,形成骨巨细胞瘤的临床生物学特点[7]。
目前文献报道与骨巨细胞的复发相关因素有:病变大小、发病位置、Campanacci分级、病理性骨折、填充物、发病年龄、是否辅助治疗等,但多方报道不一,结论矛盾[8-10]。
多种分级系统曾用于评价骨巨细胞瘤,但还是无法预测骨巨细胞瘤的临床生物学行为,目前最常用的是Campanacci分级,即根据影像学上溶骨特点的边界进行分级,但是骨巨细胞瘤的溶骨是由破骨样巨细胞引起的影像学改变,而破骨样细胞不是真正意义的肿瘤细胞,只是基质细胞的伴随细胞,所以无法预测骨巨细胞的生物学特性[11]。Ⅰ级骨巨细胞瘤属静止期病变,本研究中Ⅰ级骨巨细胞瘤行单纯刮除术后均无复发;行扩大刮除术及瘤段或分块切除术的Ⅱ级、Ⅲ级骨巨细胞瘤的复发率差异均无统计学意义,说明Campanacci分级不是骨巨细胞瘤的局部复发相关因素,与已有的研究结论一致[9]。但是行简单刮除术的Ⅱ级、Ⅲ级骨巨细胞瘤术后复发率显著高于Ⅰ级骨巨细胞瘤,可能是由于手术边界不够导致复发率增高。有研究报道,相对于其他部位,桡骨远端的骨巨细胞瘤行刮除术后局部复发率较高,主要是由于该部位的骨质以及临近腕骨与尺骨等小块骨使得肿瘤治疗的并发症较其他部位高,而行切除术可明显降低肿瘤复发率[9, 12]。本科室早期桡骨远端骨巨细胞瘤行刮除术后植骨,骨愈合多不满意,后期多改用瘤段切除术。本研究中桡骨远端骨巨细胞瘤39例,复发率为10.3%,与除脊柱与骨盆外的其他部位相比差异无统计学意义;脊柱及骶骨或骨盆骨巨细胞瘤复发率较其他部位高,文献报道主要是由于其毗邻大血管、血供丰富、周围解剖结构复杂、手术过程中不易将肿瘤彻底切除,手术并发症多,导致术后复发率高[13-14]。郭卫等一项研究结果表明,与刮除术相比,行大块切除术可明显降低骶骨或骨盆骨巨细胞瘤局部复发率[15]。另一项研究也表明,脊柱、骶骨或骨盆位置不是肿瘤复发的独立危险因素,而手术边界大小和辅助治疗手段是复发的主要影响因素[2]。本研究中,脊柱骨盆骨巨细胞瘤行刮除术的复发率为50%,而行整块切除的病例术后复发率仅为13.3%,提示脊柱或骨盆的骨巨细胞瘤,如果切除足够广泛,可有效防止骨巨细胞瘤的复发。
骨巨细胞瘤如何进行标准手术目前仍有争议。目前比较受到大家认可的经验是开大窗,足够大的长径和纵径,充分显露,刮除后磨钻磨去皮质骨1 mm,松质骨10 mm,瘤腔再进行多种方式灭活,取得良好疗效,肢体复发率在7%左右[4]。骨巨细胞瘤在局部侵袭性生长,可累及周围的软组织、皮质骨、松质骨和关节面,王臻等[16]报道,Ⅲ级骨巨细胞瘤常突破软组织,在病灶外正常松质骨内可存在跳跃病灶,皮质内有“指状突起”的生长行为,但关节软骨一般未累及,这些特性可以解释为什么骨巨细胞瘤单纯刮除后复发率高。但是对于伴软组织内、松质骨、皮质或关节软骨侵袭的骨巨细胞瘤的手术安全范围的大小,目前仍无明确定论,仍需大样本的研究结果证实。这对如何在降低复发率的基础上最大程度保留功能,具有重要意义。
肿瘤切除的彻底与否是影响骨巨细胞瘤复发的最根本因素,发病部位、手术方式等因素也是通过影响手术边界进而影响复发率,安全的手术边界是降低复发率、改善疗效的最主要措施。
作者贡献
吴朝阳: 资料收集
黄琳珊、王生淋: 起草文稿
沈荣凯: 参与统计分析
陈飞、林建华: 参与文稿撰写及修改
朱夏: 研究的构思,帮助修改文稿
| [1] | Van der Heijden L, Dijkstra PD, van de Sande MA, et al. The clinical approach toward giant cell tumor of bone[J]. Oncologist, 2014, 19(5): 550–61. DOI:10.1634/theoncologist.2013-0432 |
| [2] | Klenke FM, Wenger DE, Inwards CY, et al. Giant cell tumor of bone: risk factors for recurrence[J]. Clin Orthop Relat Res, 2011, 469(2): 591–9. DOI:10.1007/s11999-010-1501-7 |
| [3] | Niu X, Zhang Q, Hao L, et al. Giant cell tumor of the extremity: retrospective analysis of 621 Chinese patients from one institution[J]. J Bone Joint Surg Am, 2012, 94(5): 461–7. DOI:10.2106/JBJS.J.01922 |
| [4] | 牛晓辉. 病灶刮除骨水泥填充治疗四肢骨巨细胞瘤的效果评价[J]. 中国骨与关节杂志, 2016, 5(1): 29–31. [ Niu XH. Evaluation of curettage and cement reconstruction as treatment of giant cell tumors in the extremitjes[J]. Zhongguo Gu Yu Guan Jie Za Zhi, 2016, 5(1): 29–31. DOI:10.3969/j.issn.2095-252X.2016.01.007 ] |
| [5] | Sobti A, Agrawal P, Agarwala S, et al. Giant Cell Tumor of Bone-An Overview[J]. Arch Bone Jt Surg, 2016, 4(1): 2–9. |
| [6] | Reid R, Banerjee S, Sciot R. Giant cell tumours//Fletcher CDM, Unni KK, Mertens F, eds. World Health Organization classification of tumors. Pathology and genetics of tumors of soft tissue and bone[M]. Lyon: IARC Press, 2002: 309-13. |
| [7] | Wülling M, Delling G, Kaiser E. The origin of the neoplastic stromal cell in giant cell tumor of bone[J]. Hum Pathol, 2003, 34(10): 983–93. DOI:10.1053/S0046-8177(03)00413-1 |
| [8] | Klenke FM, Wenger DE, Inwards CY, et al. Recurrent giant cell tumor of long bones: analysis of surgical management[J]. Clin Orthop Relat Res, 2011, 469(4): 1181–7. DOI:10.1007/s11999-010-1560-9 |
| [9] | Errani C, Ruggieri P, Asenzio MA, et al. Giant cell tumor of the extremity: A review of 349 cases from a single institution[J]. Cancer Treat Rev, 2010, 36(1): 1–7. |
| [10] | Deheshi BM, Jaffer SN, Griffin AM, et al. Joint salvage for pathologic fracture of giant cell tumor of the lower extremity[J]. Clin Orthop Relat Res, 2007, 459: 96–104. DOI:10.1097/BLO.0b013e31805d85e4 |
| [11] | Campanacci M, Baldini N, Boriani S, et al. Giant-cell tumor of bone[J]. J Bone Joint Surg Am, 1987, 69(1): 106–14. DOI:10.2106/00004623-198769010-00018 |
| [12] | Cheng CY, Shih HN, Hsu KY, et al. Treatment of giant cell tumor of the distal radius[J]. Clin Orthop Relat Res, 2001, 383: 221–8. DOI:10.1097/00003086-200102000-00026 |
| [13] | 中国医师协会骨科医师分会, 骨肿瘤专业委员会. 骨巨细胞瘤临床循证诊疗指南[J]. 中华骨与关节外科杂志, 2018, 11(4): 276–87. [ Zhongguo Yi Shi Xie Hui Gu Ke Yi Shi Fen Hui, Gu Zhong Liu Zhuan Ye Wei Yuan Hui. Guideline for clinical evidence-based diagnosis and treatment of giant cell tumor of bone[J]. Zhonghua Gu Yu Guan Jie Wai Ke Za Zhi, 2018, 11(4): 276–87. DOI:10.3969/j.issn.2095-9958.2018.04.004 ] |
| [14] | 郭卫, 李大森, 杨毅, 等. 脊柱骨巨细胞瘤的手术治疗策略[J]. 中国脊柱脊髓杂志, 2009, 19(12): 899–903. [ Guo W, Li DS, Yang Y, et al. Surgical strategy for spinal giant cell tumor[J]. Zhongguo Ji Zhu Ji Sui Za Zhi, 2009, 19(12): 899–903. DOI:10.3969/j.issn.1004-406X.2009.12.04 ] |
| [15] | 郭卫, 汤小东, 李晓, 等. 骨盆和骶骨骨巨细胞瘤的治疗策略[J]. 中华外科杂志, 2008, 46(7): 501–5. [ Guo W, Tang XD, Li X, et al. The analysis of the treatment of giant cell tumor of the peIvis and sacrum[J]. Zhonghua Wai Ke Za Zhi, 2008, 46(7): 501–5. DOI:10.3321/j.issn:0529-5815.2008.07.006 ] |
| [16] | 王臻, 郭征, 李松建, 等. 骨巨细胞瘤组织周边生物学行为研究[J]. 中国骨科临床与基础研究杂志, 2012, 4(1): 36–41. [ Wang Z, Guo Z, Li JS, et al. Study on the oncobiological behavior at the peripheral tissues of bone giant cell tumor[J]. Zhonguo Gu Ke Lin Chuang Yu Ji Chu Yan Jiu Za Zhi, 2012, 4(1): 36–41. DOI:10.3969/j.issn.1674-666X.2012.01.006 ] |