 2018, Vol. 45
2018, Vol. 45文章信息
- 哈尔滨市南岗区1992—2013年甲状腺癌的发病趋势
- Trend of Thyroid Cancer Incidence in Nangang District of Harbin City, 1992-2013
- 肿瘤防治研究, 2018, 45(3): 167-170
- Cancer Research on Prevention and Treatment, 2018, 45(3): 167-170
- http://www.zlfzyj.com/CN/10.3971/j.issn.1000-8578.2018.17.0819
- 收稿日期: 2017-07-10
- 修回日期: 2017-10-23
引用本文 |



2. 150081 哈尔滨,哈尔滨医科大学肿瘤防治研究所;
3. 150044 哈尔滨,哈尔滨市南岗区疾病预防控制中心慢性病科
2. Cancer Prevention Institute, Harbin Medical University, Harbin 150081, China;
3. Department of Chronic Disease, Center for Disease Control and Prevention of Nangang District in Harbin City, Harbin 150044, China
甲状腺癌的发病趋势在世界范围呈现增高趋势,根据美国SEER数据分析,1974—2013年甲状腺癌的发病率从4.56/10万人年增长到14.42/10万人年,年增长3.6%,随访发病甲状腺癌患者,死亡率每年增长1.1%[1]。欧洲29个国家87个肿瘤登记处的数据表明,女性甲状腺癌5年生存率为88%,男性为81%,且其生存情况与诊断的年份无关,但与发病年龄和诊断分期有关[2]。广泛性和持续性增长是全球甲状腺癌的发病现状,随着诊断时微小肿瘤体积病例所占比例的增加,有理由认为该趋势与过度诊断有关[3]。
在中国,甲状腺癌已成为恶性肿瘤发病的重要构成部分。根据我国2013年人口监测数据,甲状腺癌的粗发病率为10.58/10万,女性发病率高于男性,已跃居女性恶性肿瘤的第五位[4]。中国甲状腺癌发病率以东部沿海地区最高,中部内陆地区较低,城市发病率高于农村[5]。2012年中国癌症中心发布的数据显示,2003—2007年间甲状腺癌的发病率每年增长14.5%[6]。甲状腺的5年相对生存率为67.5%,是仅次于乳腺癌之后的预后较好的癌种[7]。
哈尔滨市南岗区自1992年开始建立肿瘤登记系统,已对辖区内约100万人口进行连续22年监测,对黑龙江省肿瘤的发病和死亡变化情况具有一定的指导意义。为掌握哈尔滨市南岗区甲状腺癌22年间发病情况及发病趋势,本研究分析该地区肿瘤登记数据,以期为哈尔滨市乃至黑龙江省的甲状腺癌防治工作提供依据。
1 资料与方法 1.1 数据来源甲状腺癌新发病监测范围为户籍在哈尔滨市南岗区的居民,收集途径主要为诊断医院填写报告卡、医疗保险、社区健康管理系统等,病例信息由哈尔滨市南岗区疾病预防控制中心肿瘤登记处负责收集。
以年中人口数作为当年人口基数,数据主要来源于辖区的公安户籍管理部门和统计部门,1992—2013年间平均监测人口19 883 076人年。
1.2 肿瘤编码1992—2001年肿瘤登记病例编码采用国际疾病分类第9版ICD9,2002—2013肿瘤分类采用第10版ICD10和国际疾病分类肿瘤学分册第3版ICD-O-3编码,所有ICD9编码为193,ICD10编码为C73甲状腺恶性肿瘤记录被提取进行分析。
1.3 统计学方法分别计算性别、年龄别发病粗率和人口标准化发病率和截缩率。标准化人口采用Segi’s世界标准人口构成进行计算。反映发病率的变化趋势的年度变化百分比(APC)和平均年度变化百分比(AAPC)采用Joinpoint回归分析进行分析。所有计算采用Excel表格和美国国立癌症研究中心提供的Joinpoint分析软件进行,P < 0.05为差异有统计学意义。
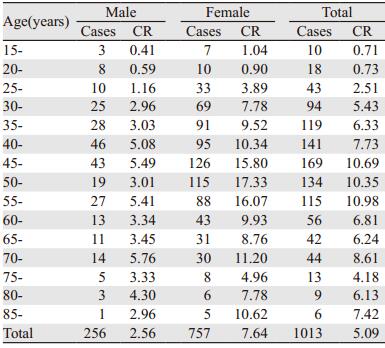
2 结果 2.1 甲状腺癌的发病情况1992—2013年间,哈尔滨市南岗区甲状腺癌累计发病1 013例,其中男256例,女757例,男女发病比为1:2.96。平均发病率5.09/10万,其中男性发病率为2.56/10万,女性发病率为7.64/10万。各年度发病率见表 1。

|
根据1992—2013年间肿瘤登记数据,甲状腺癌的最小发病年龄为15岁,最大发病年龄为89岁。男性最高发病年龄在45~49岁间,发病率为5.49/10万;女性最高发病年龄在50~54岁间,发病率为17.33/10万。各年龄组别中,女性甲状腺癌的发病率均较男性发病率高,见表 2,图 1。
|

|
| 图 1 1992—2013年哈尔滨市南岗区甲状腺癌年龄别发病率曲线(1/10万) Figure 1 Age-specific thyroid cancer incidence curves in Nangang District of Harbin City, 1992-2013 (1/105) |
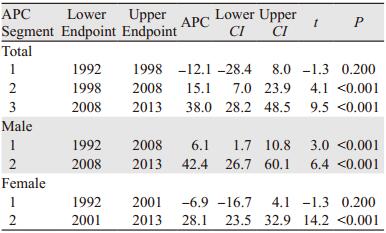
1992—2013年间,哈尔滨市南岗区甲状腺癌发病率平均年度变化百分比(AAPC)为12.6%(95%CI: 6.1%~19.5%),女性AAPC为11.7%(95%CI: 6.4%~17.3%),男性AAPC为13.8%(95%CI: 6.4%~17.3%)。经Joinpoint回归分析,22年间,总体甲状腺癌发病率共分为三个阶段,1992—1998年呈下降趋势,1999—2008年和2008—2013年呈上升趋势,其中2008—2013年甲状腺癌的发病率呈快速增高趋势(APC: 38.0%),见表 3、图 2。
|

|
| ^: the annual percent change(APC) was significantly different from zero at alpha=0.05. A: Final selected model: 2 Joinpoints; B, C: Final selected model: 1 Joinpoint 图 2 1992—2013年哈尔滨市南岗区甲状腺癌发病率年度变化百分比曲线(1/10万) Figure 2 APC curves of thyroid cancer incidence rate in Nangang District of Harbin City, 1992-2013 (1/105) |
本研究基于哈尔滨市南岗区全人群22年肿瘤登记数据进行分析,累积监测19 883 076人年,共报告甲状腺癌新发病例1 013人,甲状腺癌的年平均发病率5.09/10万,女性发病率高于男性,最高发病年龄在45~59岁之间。甲状腺癌的发病率以平均每年12.6%的速度增长。甲状腺癌发病率是否存在地域性差异,报道尚不统一。Hanley等[8]采用时空分析发现,甲状腺癌的分布与地理位置无关,与当地医疗资源无关,但是该研究仅在一个州进行,地理范围存在局限性。Brown等[9]分析了加拿大多伦多城市中甲状腺癌东北地区的发病率高于东南地区,这一部分原因是由于移民造成,也有部分原因是个体原因。江苏省昆山市2011年甲状腺癌男性发病率为4.85/10万,2012年为5.57/10万,女性2011年和2012年的中标发病率为12.16/10万和16.54/10万[10]。与昆山地区甲状腺癌发病率相比,南岗区男性发病率略高于昆山地区,而女性的发病率略低,这可能提示甲状腺癌的发病存在一定的地域性,特别是性别地域性。
甲状腺癌相对于肺癌、肝癌等肿瘤的发病率低,但是在我国的恶性肿瘤发病谱中居第七位[4],且增长势头迅猛。北京市2010年较1995年甲状腺癌发病增长538.71%,APC值为12.12%[11]。天津市2002—2006年甲状腺癌的发病率比1981年增长了26.7%,年均增长3.1%[12]。广州市主城区2011年甲状腺癌的世标率为9.13/10万,较2000年增加了204.73%, APC为10.5%[13]。哈尔滨市南岗区甲状腺癌的APC与北京市结果接近,但高于天津和广州,这可能与分析的年限有关。哈尔滨市南岗区1992—1998年甲状腺癌一度出现负增长,APC为-12.1%,但在1998—2008年呈增长趋势,2009—2013增长幅度加快。1992—1998年间甲状腺癌发病率呈下降趋势,一方面是由于该期间发病人数在5~14之间,发病例数少会导致数据波动大;另一方面这一时期甲状腺癌的诊疗水平和人群主动体检意识还比较低,如CT扫描的增加导致甲状腺癌的检出率增加[14];最后还可能与肿瘤登记漏报有关。
国内外报道均提示女性甲状腺癌发病率约是男性的3倍,本研究中女性甲状腺癌的发病率是男性的2.96倍,与国际上报道的基本一致[6, 15]。研究认为,女性雌激素和生育产次是甲状腺癌发病的重要病因,绝经后女性发病风险增加,特别是口服避孕药,绝经后激素疗法可以减少1/3的风险[16]。伊朗2010年报告男性甲状腺癌的发病高峰在45~49岁之间,女性在40~45岁之间,女性的发病高峰早于男性[17],本研究中男性的发病高峰与伊朗报道的接近,而女性在50~54岁之间,晚于伊朗女性,这可能与人种、环境有关,也可能是观察的年限不一致,但总体发病高峰的年龄分布比较接近,因此40~54岁的人群可作为甲状腺癌防治的重点人群。
随着研究广度和深度的增加,环境因素、放射性污染、遗传因素等与甲状腺癌发病有关的因素不断被报道,筛查技术和人群对癌症认知水平的上升也增加了甲状腺癌的检出率,从而加速甲状腺癌发病率的上升。监测甲状腺癌的人群发病率,研究其发病趋势,有利于甲状腺癌防治工作的开展。
| [1] | Lim H, Devesa SS, Sosa JA, et al. Trends in thyroid cancer incidence and mortality in the United States, 1974-2013[J]. JAMA, 2017, 317(13): 1338–48. DOI:10.1001/jama.2017.2719 |
| [2] | Dal Maso L, Tavilla A, Pacini F, et al. Survival of 86, 690 patients with thyroid cancer: A population-based study in 29 European countries from EUROCARE-5[J]. Eur J Cancer, 2017, 77: 140–52. DOI:10.1016/j.ejca.2017.02.023 |
| [3] | Turcotte LM, Liu Q, Yasui Y, et al. Temporal trends in treatment and subsequent neoplasm risk among 5-year survivors of childhood cancer, 1970-2015[J]. JAMA, 2017, 317(8): 814–24. DOI:10.1001/jama.2017.0693 |
| [4] | 陈万青, 郑荣寿, 张思维, 等. 2013年中国恶性肿瘤发病和死亡分析[J]. 中国肿瘤, 2017, 26(1): 1–7. [ Chen WQ, Zheng RS, Zhang SW, et al. Report of cancer incidence and mortality in China, 2013[J]. Zhongguo Zhong Liu, 2017, 26(1): 1–7. ] |
| [5] | 董芬, 张彪, 单广良. 中国甲状腺癌的流行现状和影响因素[J]. 中国癌症杂志, 2016, 26(1): 47–52. [ Dong F, Zhang B, Shan GL. Distribution and risk factors of thyroid cancer in China[J]. Zhongguo Ai Zheng Za Zhi, 2016, 26(1): 47–52. ] |
| [6] | 刘玉琴, 张书全, 陈万青, 等. 中国2003-2007年甲状腺癌发病死亡现状及流行趋势分析[J]. 中华流行病学杂志, 2012, 33(10): 1044–8. [ Liu YQ, Zhang SQ, Chen WQ, et al. Trend of ineidence and mortality on thyroid cancer in China during 2003-2007[J]. Zhonghua Liu Xing Bing Xue Za Zhi, 2012, 33(10): 1044–8. DOI:10.3760/cma.j.issn.0254-6450.2012.10.011 ] |
| [7] | Zeng H, Zheng R, Guo Y, et al. Cancer survival in China, 2003-2005: a population-based study[J]. Int J Cancer, 2015, 136(8): 1921–30. DOI:10.1002/ijc.29227 |
| [8] | Hanley JP, Jackson E, Morrissey LA, et al. Geospatial and temporal analysis of thyroid cancer incidence in a rural population[J]. Thyroid, 2015, 25(7): 812–22. DOI:10.1089/thy.2015.0039 |
| [9] | Brown P, Jiang H, Ezzat S, et al. A detailed spatial analysis on contrasting cancer incidence patterns in thyroid and lung cancer in Toronto women[J]. BMC Public Health, 2016, 16: 950. DOI:10.1186/s12889-016-3634-4 |
| [10] | 胡文斌, 张婷, 秦威, 等. 昆山市2006~2012年甲状腺癌发病率趋势分析[J]. 中国肿瘤, 2014, 23(7): 558–62. [ Hu WB, Zhang T, Qin W, et al. An analysis of the trend of incidence of thyroid cancer from 2006 to 2012 in Kunshan, Jiangsu province[J]. Zhongguo Zhong Liu, 2014, 23(7): 558–62. DOI:10.11735/j.issn.1004-0242.2014.07.A006 ] |
| [11] | 杨雷, 孙婷婷, 袁延楠, 等. 1995-2010年北京城区甲状腺癌发病趋势及病理特征分析[J]. 中华预防医学杂志, 2013, 47(2): 109–12. [ Yang L, Sun TT, Yun YN, et al. Time trends and pathological characteristics of thyroid cancer in urban Beijing, 1995-2010[J]. Zhonghua Yu Fang Yi Xue Za Zhi, 2013, 47(2): 109–12. ] |
| [12] | 钱碧云, 何敏, 高明, 等. 2002-2006年天津市甲状腺癌发病率与26年间长期趋势分析[J]. 中华普通外科杂志, 2011, 26(4): 275–8. [ Qian BY, He M, Gao M, et al. Thyroid cancer incidence in the city of Tianjin during 2002-2006 and its secular trend in recent 26 year[J]. Zhonghua Pu Tong Wai Ke Za Zhi, 2011, 26(4): 275–8. ] |
| [13] | 李科, 林国桢, 周琴, 等. 2000-2011年广州市城区甲状腺癌的发病趋势分析[J]. 中华预防医学杂志, 2015, 49(2): 142–6. [ Li K, Lin GZ, Zhou Q, et al. Time trends of the incidence of thyroid cancer in urban Guangzhou, 2000-2011[J]. Zhonghua Yu Fang Yi Xue Za Zhi, 2015, 49(2): 142–6. ] |
| [14] | Hoang JK, Choudhury KR, Eastwood JD, et al. An exponential growth in incidence of thyroid cancer: trends and impact of CT imaging[J]. AJNR Am J Neuroradiol, 2014, 35(4): 778–83. DOI:10.3174/ajnr.A3743 |
| [15] | Bann DV, Goyal N, Camacho F, et al. Increasing incidence of thyroid cancer in the commonwealth of Pennsylvania[J]. JAMA Otolaryngol Head Neck Surg, 2014, 140(12): 1149–56. DOI:10.1001/jamaoto.2014.1709 |
| [16] | Cordina-Duverger E, Leux C, Neri M, et al. Hormonal and reproductive risk factors of papillary thyroid cancer: A population-based case-control study in France[J]. Cancer Epidemiol, 2017, 17: 78–84. |
| [17] | Modirian M, Cheraghi Z, Rahimzadeh S, et al. Burden assessment of thyroid cancer in Iran from 1990 to 2010: Lessons obtained from global burden of disease report 2010[J]. Asian Pac J Cancer Prev, 2015, 16(17): 7743–8. DOI:10.7314/APJCP.2015.16.17.7743 |