 2020, Vol. 31
2020, Vol. 31扩展功能
文章信息
- 王桢, 凌锋, 刘营, 任江萍, 孙继民
- WANG Zhen, LING Feng, LIU Ying, REN Jiang-ping, SUN Ji-min
- 浙江省2015-2019年登革热流行特征分析
- Epidemiological characteristics of dengue fever in Zhejiang province, China, 2015-2019
- 中国媒介生物学及控制杂志, 2020, 31(6): 643-647
- Chin J Vector Biol & Control, 2020, 31(6): 643-647
- 10.11853/j.issn.1003.8280.2020.06.003
-
文章历史
- 收稿日期: 2020-09-20




登革热是由登革病毒引起的急性病毒性传染病,其传播媒介主要为埃及伊蚊(Aedes aegypti)和白纹伊蚊(Ae. albopictus),是《中华人民共和国传染病防治法》规定的乙类传染病。登革病毒感染大多数以隐性感染为主,以突发高热、剧烈头痛、眼眶后痛、肌肉和关节痛为主要临床表现,可伴有皮疹、淋巴结肿大和白细胞减少,严重者可出现出血、休克以致死亡,目前尚无特效的治疗药物[1]。
浙江省位于中国东南沿海,属于亚热带季风气候,适宜白纹伊蚊的生长繁殖,全省白纹伊蚊密度普遍较高,而且浙江省对外经贸和旅游发达,登革热病例输入较多,导致不断有本地疫情发生,自2015年以来浙江省每年均有登革热本地疫情发生[2-4],登革热已成为浙江省最重要的传染病之一。本研究系统收集了浙江省2015-2019年登革热病例信息,分析了其流行特征,并比较了输入病例和本地病例流行特征的差异,为浙江省登革热精准防控提供科学依据。
1 材料与方法 1.1 病例诊断2018年8月1日前,根据中华人民共和国卫生行业标准《登革热诊断标准》(WS 216-2008)进行病例诊断,自2018年8月1日起根据中华人民共和国卫生行业标准《登革热诊断》(WS 216-2018)进行病例诊断。
1.2 数据收集从中国疾病预防控制信息系统收集浙江省2015-2019年登革热病例信息,主要包括性别、年龄、职业、现住地址、发病日期、诊断日期等。
1.3 数据分析采用SPSS 20.0软件对登革热病例的性别、年龄、职业、季节分布、地区分布、发病到确诊时间间隔进行描述性分析,采用ArcGIS 10.2软件绘制不同年份登革热病例的地区分布,采用χ2检验分析登革热输入病例和本地病例性别、职业差异是否有统计学意义;采用Kruskal-Wallis H检验分析输入病例和本地病例的年龄、发病至确诊时间间隔差异是否有统计学意义。P<0.05为差异有统计学意义。
2 结果 2.1 一般情况浙江省2015-2019年共报告2 532例登革热病例,其中961例输入病例,1 571例本地病例,输入病例和本地病例比例为0.61:1。2015-2019年每年均有病例报告,分别报告了63、63、1 237、249和920例病例,其中输入病例逐年递增,分别为46、55、87、164和609例,本地病例分别为17、8、1 150、85和311例。输入病例和本地病例比例分别为2.71:1、6.88:1、0.08:1、1.93:1和1.96:1,除2017年外,其他年份输入病例均多于本地病例。
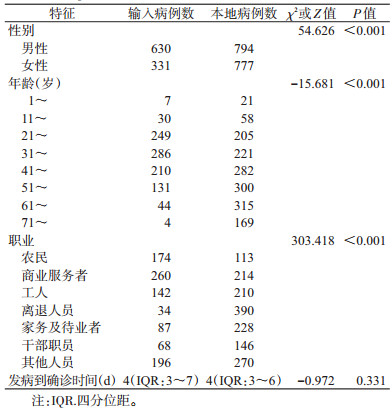
2.2 人群分布特征2 532例病例中,男性1 424例,女性1 108例,男女性别比为1.29:1。输入病例中,男性630例,女性331例;本地病例中,男性794例,女性777例。经χ2检验,输入病例中男性构成比显著高于本地病例中男性构成比(χ2=54.626,P<0.001)。见表 1。
|
2 532例病例的中位年龄为44岁,四分位数间距为32~58岁,年龄最小为1岁,最大为94岁。输入病例的中位年龄为37岁,四分位数间距为29~47岁,最小年龄为2岁,最大为76岁;本地病例的中位年龄为50岁,四分位数间距为35~63岁,年龄最小为1岁,最大为94岁。经Kruskal-Wallis H检验,输入病例年龄显著小于本地病例年龄(Z=-15.681,P<0.001)。见表 1。
输入病例的年龄主要在21~60岁之间,占91.16%(876/961),其中31~40岁年龄组病例最多(286例);本地病例的年龄主要在21~70岁之间,占84.21%(1 323/1 571),其中61~70岁年龄组病例数最多(300例)。见图 1。

|
| 图 1 浙江省2015-2019年登革热输入病例和本地病例年龄(岁)分布 Figure 1 Age distribution of imported cases and local cases of dengue fever in Zhejiang province, 2015-2019 |
| |
2 532例病例中商业服务人员最多(474例),其次是离退人员、工人、家务及待业者、农民和干部职员,分别为424、352、315、287和214例,其他职业为466例。输入病例的职业主要为商业服务者、农民和工人,共占59.94%(576/961);本地病例的职业主要为离退人员、家务及待业者、商业服务者和工人,共占66.33%(1 042/1 571)。经χ2检验,输入病例和本地病例的职业分布差异有统计学意义(χ2=303.418,P<0.001)。见表 1。
2.3 季节分布特征2015年1月至2019年12月的60个月中除2015年1月、2016年6月、2017年3月和2018年3月外,其余56个月浙江省均有登革热病例报告。病例主要发生在6-10月,占89.42%(2 264/2 532)。输入病例每月均有发生,但大多数在6-10月之间,共有699例;本地病例发生在7-11月,其他月份无本地病例发生。见图 2。

|
| 图 2 浙江省2015-2019年登革热输入病例和本地病例发病时间分布 Figure 2 Seasonal distribution of imported cases and local cases of dengue fever in Zhejiang province, 2015-2019 |
| |
2015-2019年浙江省90个县(市、区)中共有86个报告过登革热病例,其中有44个报告过本地病例。全省所有地市均有病例报告,报告病例数前5位的是杭州、温州、宁波、台州和金华市,分别为1 450、327、192、173和135例。报告病例的县(市、区)数量逐年增多,2015-2019年分别为23、27、37、52和85个(图 3),其中报告本地病例的县(市、区)数分别为5、1、22、12和34个。全省所有地市均有输入病例发生,除湖州和丽水市外,其他9个地市均有本地病例发生。

|
| 图 3 浙江省2015—2019年登革热病例地区分布 Figure 3 Geographic distribution of imported cases and local cases of dengue fever in Zhejiang province, 2015-2019 |
| |
东南亚的国家和地区是输入病例的主要来源,柬埔寨输入的最多为397例,其次是泰国(116例)、越南(74例)、印度(70例)、菲律宾(52例)、马来西亚(38例)、缅甸(31例)、印度尼西亚(25例)、马尔代夫(24例)和孟加拉国(15例),还有119例来源于非洲、东南亚等地的其他国家以及我国广东和云南省。见图 4。

|
| 图 4 浙江省2015—2019年登革热输入病例来源 Figure 4 Origin of imported cases of dengue fever in Zhejiang province, 2015-2019 |
| |
2 532例登革热发病到确诊时间间隔中位数为4 d,四分位数间距为3~6 d,最短的为发病当天确诊,最长的为42 d。输入病例发病到确诊时间间隔中位数为4 d,四分位数间距为3~7 d,最短的为发病当天确诊,最长的为27 d。本地病例发病到确诊时间间隔中位数为4 d,四分位数间距为3~6 d,最短的为发病当天确诊,最长的为42 d。经Kruskal-Wallis H检验,输入病例与本地病例发病到确诊时间间隔差异无统计学意义(Z=-0.972,P=0.331)。见表 1。
3 讨论由于全球气候变暖,城市化迅速发展、国际间交往日益频繁等因素,登革热流行区域不断扩大,其发病率在过去50年增加了30倍,疾病负担日趋严重,已成为世界性的公共卫生问题。Bhatt等研究结果显示,全球每年有25亿~40亿人口的健康受到登革热的威胁,每年约有3.9亿登革病毒感染者,其中确诊病例9 600万例,约2.5万人因登革热死亡[5-7]。2019年,我国大陆地区登革热疫情形势非常严峻,有28个省(直辖市、自治区)共报告22 599例登革热病例,其中13个省(直辖市、自治区)发生了本地疫情,是登革热本地疫情波及范围最广的一年[8]。
本研究系统分析了浙江省近5年登革热流行状况,发现浙江省除了4个县(市、区)外,其余86个县(市、区)均有登革热病例报告,其中44个发生了登革热本地疫情,而且报告病例的县(市、区)呈逐年增多趋势,提示浙江省登革热防控形势非常严峻,浙江省各级政府要进一步加强对登革热防控的重视程度,广泛开展爱国卫生运动,降低蚊媒密度,并进一步推广快速检测试剂,及时发现登革热输入病例,有效预防登革热本地疫情的发生[9]。
与其他研究类似[10-11],本研究发现浙江省登革热主要发生在6-10月,病例主要为中老年的商业服务人员、离退人员、家务及待业者、工人和农民,提示浙江省应该在6月份之前就要针对重点地区的重点人群广泛采取综合性登革热防控措施,严防本地疫情发生。
此外,本研究还比较了浙江省输入病例和本地病例的流行特征,发现输入病例中男性病例的构成比较高、年龄更小,商业服务人员的构成比也较高,这可能与境外旅游和商业人员中青壮年男性更多有关[12]。本地病例中离退人员最多主要是因为:2017年杭州市登革热暴发时病例数较多,占所有本地病例数的70%左右,此次暴发发生的区域主要在杭州市的老城区,老城区的居民中离退人员比例较高,导致离退人员的病例数较多。输入病例全年每个月均有发生,但自7月开始才有本地病例发生,这充分说明浙江省不存在登革热的自然疫源地,病例输入后传给当地白纹伊蚊,白纹伊蚊经过外潜伏期后叮咬当地居民,导致本地疫情的发生。
登革热病例的传染期为发病前1 d到发病后5 d,浙江省输入病例和本地病例发病到确诊时间间隔中位数均为4 d,很多登革热病例的确诊时间较晚,传染期未能确诊,没有得到有效管理,可能造成登革热的本地传播。因此,建议浙江省各级卫生行政部门加强医疗机构医务人员的培训和督导,有效提高医务人员登革热诊断的意识和能力,缩短发病到确诊时间间隔,降低本地疫情发生的风险。
综上所述,本研究系统总结了浙江省近5年登革热流行特征,明确了浙江省登革热防控的重点时间、重点地区和重点人群,比较了输入病例和本地病例流行特征的差异,为浙江省登革热的精准防控提供了科学依据。
| [1] |
World Health Organization. Dengue guidelines for diagnosis, treatment, prevention and control[R]. Geneva: World Health Organization, 2009: 14.
|
| [2] |
陈奕, 易波, 劳旭影, 等. 浙江省宁波市登革热疾病经济负担研究[J]. 中国媒介生物学及控制杂志, 2020, 31(4): 385-388. Chen Y, Yi B, Lao XY, et al. A study of economic burden of dengue fever in Ningbo, Zhejiang province, China[J]. Chin J Vector Biol Control, 2020, 31(4): 385-388. DOI:10.11853/j.issn.1003.8280.2020.04.001 |
| [3] |
孙昼, 陈珺芳, 竹军伟, 等. 杭州市2018年一起农村登革热暴发疫情调查研究[J]. 中国媒介生物学及控制杂志, 2020, 31(4): 465-468. Sun Z, Chen JF, Zhu JW, et al. An investigation of a dengue outbreak in a rural area in Hangzhou, Zhejiang province, China, 2018[J]. Chin J Vector Biol Control, 2020, 31(4): 465-468. DOI:10.11853/j.issn.1003.8280.2020.04.018 |
| [4] |
叶凌, 谭启龙, 赵剑刚, 等. 浙江省一起海岛地区登革热本地暴发疫情的隐性感染情况调查[J]. 中国媒介生物学及控制杂志, 2020, 31(3): 353-357. Ye L, Tan QL, Zhao JG, et al. An investigation of inapparent infections in a local outbreak of dengue fever in an island area of Zhejiang province, China[J]. Chin J Vector Biol Control, 2020, 31(3): 353-357. DOI:10.11853/j.issn.1003.8280.2020.03.022 |
| [5] |
Bhatt S, Gething PW, Brady OJ, et al. The global distribution and burden of dengue[J]. Nature, 2013, 496(7446): 504-507. DOI:10.1038/nature12060 |
| [6] |
World Health Organization. Dengue and severe dengue[EB/OL]. (2020-06)[2020-09-20]. https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue.
|
| [7] |
Brady OJ, Gething PW, Bhatt S, et al. Refining the global spatial limits of dengue virus transmission by evidence-based consensus[J]. PLoS Negl Trop Dis, 2012, 6(8): e1760. DOI:10.1371/journal.pntd.0001760 |
| [8] |
刘起勇. 我国登革热流行新趋势、防控挑战及策略分析[J]. 中国媒介生物学及控制杂志, 2020, 31(1): 1-6. Liu QY. Dengue fever in China:new epidemical trend, challenges and strategies for prevention and control[J]. Chin J Vector Biol Control, 2020, 31(1): 1-6. DOI:10.11853/j.issn.1003.8280.2020.01.001 |
| [9] |
孟凤霞, 王义冠, 冯磊, 等. 我国登革热疫情防控与媒介伊蚊的综合治理[J]. 中国媒介生物学及控制杂志, 2015, 26(1): 4-10. Meng FX, Wang YG, Feng L, et al. Review on dengue prevention and control and integrated mosquito management in China[J]. Chin J Vector Biol Control, 2015, 26(1): 4-10. DOI:10.11853/j.issn.1003.4692.2015.01.002 |
| [10] |
周航, 李昱, 牟笛, 等. 中国2013年登革热流行病学分析[J]. 公共卫生与预防医学, 2015, 26(2): 12-15. Zhou H, Li Y, Mu D, et al. Analysis on epidemiological characteristics of dengue in China, 2013[J]. J Public Health Prev Med, 2015, 26(2): 12-15. |
| [11] |
Lai SJ, Huang ZJ, Zhou H, et al. The changing epidemiology of dengue in China, 1990-2014:a descriptive analysis of 25 years of nationwide surveillance data[J]. BMC Med, 2015, 13(1): 100. DOI:10.1186/s12916-015-0336-1 |
| [12] |
林君芬, 李傅冬, 刘社兰, 等. 浙江省2005-2013年输入性登革热流行特征分析[J]. 浙江预防医学, 2014, 26(12): 1233-1235. Lin JF, Li FD, Liu SL, et al. Analysis of epidemic characteristics of imported dengue fever in Zhejiang from 2005 to 2013[J]. Zhejiang J Prev Med, 2014, 26(12): 1233-1235. |