 2020, Vol. 31
2020, Vol. 31扩展功能
文章信息
- 徐朦, 刘小波, 宋秀平, 王艳华, 漆莉, 郭亚菲, 李文, 刘起勇
- XU Meng, LIU Xiao-bo, SONG Xiu-ping, WANG Yan-hua, QI Li, GUO Ya-fei, LI Wen, LIU Qi-yong
- 基于伤残调整寿命年的2010-2019年中国登革热疾病负担评估研究
- Assessment research on the disease burden of dengue fever in China from 2010 to 2019 based on disability-adjusted life years
- 中国媒介生物学及控制杂志, 2020, 31(5): 509-512
- Chin J Vector Biol & Control, 2020, 31(5): 509-512
- 10.11853/j.issn.1003.8280.2020.05.001
-
文章历史
- 收稿日期: 2020-07-17




2 中国疾病预防控制中心传染病预防控制所鼠疫室, 传染病预防控制国家重点实验室, 北京 102206;
3 重庆市疾病预防控制中心, 重庆 400042
2 National Institute for Communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention;
3 Chongqing Center for Disease Control and Prevention
登革热(dengue fever)是由登革病毒引起的急性虫媒传染病, 主要通过埃及伊蚊(Aedes aegypti)和白纹伊蚊(Ae. albopictus)传播[1]。全世界每年约有3.9亿人感染登革热, 9600万例出现临床症状[2]。我国自2010年以来登革热报告病例数几乎呈逐年增加趋势, 其中2014和2019年是我国登革热暴发的高峰年, 报告病例数分别超过了4.6万例和2.2万例, 登革热的病例空间分布范围和境外输入风险也逐渐增大, 对人群的生命安全和生产生活造成了很大影响。面对日益严峻的防控形势, 量化与评估登革热对我国造成的损失十分重要。
疾病负担(burden of disease, BOD)是衡量疾病、伤害和早死对社会和国家造成的健康及经济影响的一项指标[3], 包括疾病的流行病学负担和经济负担。合理进行疾病负担的测算对于国家分配卫生资源监测人群健康状况、制定疾病预防和干预措施可起到重要作用, 引起各国政府和卫生决策者的高度重视。疾病负担的评价方法演变经历了很长的过程, 目前,伤残调整寿命年(disability adjusted life years, DALY)是最具代表性、运用最多的疾病负担评价指标[4]。
本研究利用世界卫生组织(WHO)提出的研究方法, 采用DALY作为疾病负担综合评价指标, 以2010-2019年我国法定传染病监测系统的报告病例数据为基础, 测算我国登革热的疾病负担, 为登革热可持续控制及卫生资源的合理配置提供参考。
1 材料与方法 1.1 数据来源登革热的发病数据和死亡数据来源于中国疾病预防控制中心(CDC)的传染病信息监测系统, 包括31个省(自治区、直辖市)和新疆生产建设兵团的报告病例数、死亡数。主要信息包括性别、年龄、发病日期、诊断日期、死亡日期和病例类型.等。人口数据来源于中国CDC信息中心, 使用2010年第6次人口普查数据。
1.2 数据处理利用Excel 2013软件对登革热原始发病数据进行汇总、处理及分析, 并对其按年份、年龄、性别进行统计。
1.3 DALY的估算DALY的估算采用WHO推荐的方法。DALY以时间(年)为度量单位, 包括早死损失寿命年(years of life lost due to mortality, YLL)和伤残损失寿命年(years lived with disability, YLD)两部分[5], 即DALY=YLL+YLD。它被广泛地应用于全球的疾病负担评价[6-7]。计算公式:
|
(1) |
其中, D为伤残权重(0~1之间取值, 0代表完全健康, 1代表死亡), 针对登革热伤残权重的选择尚没有统一定论, 本研究参考其他文献, 对于伤残权重D设置为0.81[8-9]; L为伤残平均持续时间, 根据以往的研究采取保守估计, 将残疾的平均持续时间设置为14d[10]; a为发病导致失能或死亡时的年龄; r为社会贴现率; β为年龄加权函数的参数; C为连续调整系数。在本研究中使用了完整的年龄权重并根据WHO推荐设置了其他参数[6]。年龄组的划分依据WHO推荐方法,划分为0~、5~、15~、30~、45~、60~、70~和≥80岁共8个年龄组。利用WHO官网下载的负担计算工具, 将发病、死亡数据以及相关参数输人相关电子表格并完成YLL、YLD及DALY的计算。
1.4 统计学分析利用Excel 2013软件统计和计算2010-2019年间登革热YLD、YLL及DALY负担水平及变化趋势; 比较2010-2019年我国不同性别、年龄人群归因于登革热的DALY水平。
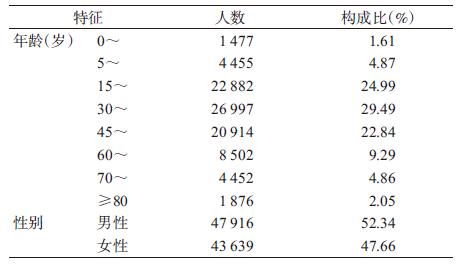
2 结果 2.1 基本情况2010-2019年我国31个省(自治区、直辖市)和新疆生产建设兵团累计报告登革热新发病例91 555例, 其中男性47 916例(52.34%)、女性43639例(47.66%)。每个年龄段均有病例分布,主要集中在15~59岁, 占总病例数的77.32%, 见表 1。我国登革热死亡人数共13例, 仅2011、2014、2017-2019年有零星分布。
|
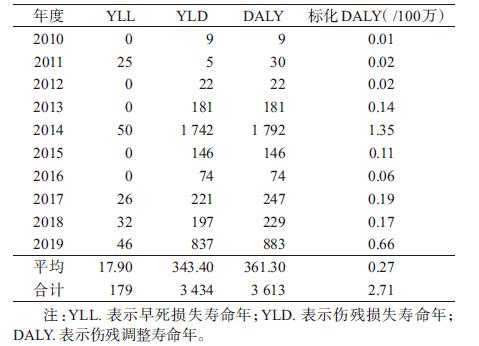
2010-2019年登革热的累计YLL为179人年,累计YLD为3 434人年,累计DALY为3613人年, 标化后为2.71人年/100万。10年间平均DALY为361.30人年, 2014和2019年为疫情高峰年, 其DALY达到了1 792和883人年,远高于平均水平。2010- 2019年DALY负担水平变化较大, 由9人年增至883人年, YLD与DALY负担水平变化基本-致。见表 2。
|
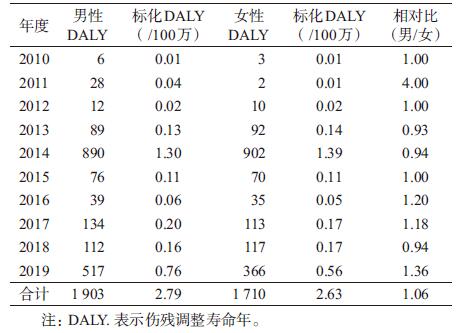
2010-2019年男性DALY负担累计1 903人年,女性DALY负担累计1 710人年,标化后的DALY男性为2.79人年/100万,女性为2.63人年/100万, 男性. DALY负担水平略高于女性,相对比(男女)为1.06。男性与女性登革热的DALY负担大体趋势一致, 2011年男性与女性的DALY负担水平差异较大,相对比为4.00。在2013、2014和2018年男性DALY负担水平略低于女性,相对比分别为0.93、0.94和0.94, 2010、2012和2015年男性与女性DALY负担水平相同, 其余年份男性DALY负担水平均高于女性。见表 3。
|
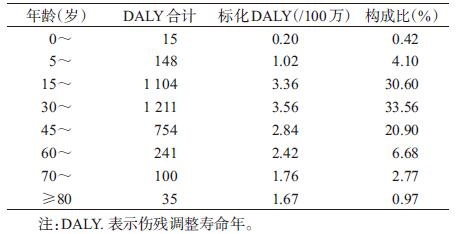
2010-2019年间,我国登革热的DALY负担年.龄分布主要集中在15~、30~、45~岁年龄段, 共占85.06%。其中, 0~岁的DALY最少, 占0.42%, 60岁以上人群的DALY负担占10.42%。见表 4。
|
我国在虫媒传染病领域的疾病负担研究较少, 登革热作为我国法定报告乙类传染病之一, 目前尚未见使用我国法定传染病监测系统数据估算其疾病负担的相关报道。本研究首次结合我国法定传染病监测系统数据, 参考WHO提出的方法, 应用DALY指标对登革热疾病负担进行分析。
近年来, 登革热在我国呈现多点暴发态势,境外输人病例的风险也日益增加, 因此了解登革热造成的疾病负担对于我国登革热防控策略、措施完善和资源合理配置非常重要。本研究发现, 我国登革热疾病负担有如下特点:①2010年DALY负担最轻, 仅9人年, 2011年登革热发病数少于2010年,总DALY负担却大于2010年,原因是2010年无死亡病例, 而2011年的死亡病例贡献了很大一部分的疾病负担, 其余年份的DALY负担均与发病例数呈正比,因中国登革热死亡数较少, 总DALY负担中YLL负担的贡献较小,疾病负担主要归因于YLD; ②男性与女性疾病负担水平基本一致, 男性略高于女性; ③归因于登革热的疾病负担在每个年龄段均有分布,年龄跨度较大, 主要集中在15~岁、30~岁、45~岁3个年龄段, 占比达到85%以上; 儿童和60岁以,上老年人造成的疾病负担占比较少。中年人群对于疾病负担贡献较大, 该年龄段发病可能会导致误工进而造成劳动力损失,这意味着这一部分病例除个人负担外还可能会造成沉重的社会负担。
本研究发现, 2010-2019年我国登革热标化的DALY总计为2.71人年/100万, 在2014年达到峰值(1.35人年/100万),其余年份均 < 1人年,明显低于巴西(22人年/100万)[11]、墨西哥(65人年/100万)[12]和菲律宾(535人年/100万)[13]的水平, 原因可能与近年来中国登革热的发病水平低于上述国家, 相应的疾病负担相对较低有关。研究结果显示,近年来我国登革热疾病负担总体呈现波动上升趋势, 当前我国尚无可推广使用的登革热疫苗和特效治疗药物, 加之多维因素的综合驱动作用, 如气候变化引起媒介伊蚊分布区不断向西向北扩大[14], 全球化及城市化造成登革热传播风险增加, 未来我国登革热疫情防控形势日趋严峻[15]。因此,科学评估登革热的疾病负担对于我国登革热防控资源优化配置十分重要。
本研究的优势在于首次根据我国法定传染病监测系统数据进行疾病负担的计算,选用数据真实可靠, 保证结果的合理性。本研究未考虑漏报病例, 由于登革热绝大多数为轻型病例且症状不明显, 存在漏报及低估登革热疾病负担的风险[16]。今后, 可开展主动监测工作从而弥补现有登革热报告系统存在的不足。
综上所述,本研究基于我国传染病监测系统资料, 对我国登革热疾病负担进行了系统分析, 为我国登革热可持续控制提供了科学依据。
志谢 伦敦卫生与热带医学院的专家OliverBrady与WHO的专家Raman Velayudhan对登革热疾病负担研究进行指导与帮助, 特此志谢| [1] |
王莹, 周良才. 登革热风险评估方法的研究及应用进展[J]. 现代预防医学, 2018, 45(15): 2832-2835. Wang Y, Zhou LC. Research and application of dengue risk assessment methods[J]. Mod Prevent Med, 2018, 45(15): 2832-2835. |
| [2] |
Bhatt S, Gething PW, Brady OJ, et al. The global distribution and burden of dengue[J]. Nature, 2013, 496(7446): 504-507. DOI:10.1038/nature12060 |
| [3] |
吕繁, 曾光. 疾病负担评价的理论框架及其发展[J]. 中华流行病学杂志, 2001, 22(4): 259-261. Lyu F, Zeng G. Theoretical framework for disease burden assessment and its development[J]. Chin J Epidemiol, 2001, 22(4): 259-261. DOI:10.3760/j.issn:0254-6450.2001.04.009 |
| [4] |
李茜瑶, 周莹, 黄辉, 等. 疾病负担研究进展[J]. 中国公共卫生, 2018, 34(5): 777-780. Li XY, Zhou Y, Huang H, et al. Progress in disease burden researches[J]. Chin J Public Health, 2018, 34(5): 777-780. DOI:10.11847/zgggws1118319 |
| [5] |
GBD 2016 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2016:a systematic analysis for the Global Burden of Disease Study 2016[J]. Lancet, 2017, 390(10100): 1260-1344. DOI:10.1016/S0140-6736(17)32130-X |
| [6] |
Murray CJL. Quantifying the burden of disease:the technical basis for disability-adjusted life years[J]. Bull World Health Organ, 1994, 72(3): 429-445. DOI:10.1146/annurev.pu.15.050194.002121 |
| [7] |
Mathers CD, Vos T, Lopez AD, et al. National burden of disease studies: a practical guide[R]. Geneva: World Health Organization, 2001: 9-10.
|
| [8] |
Shepard DS, Undurraga EA, Halasa YA. Economic and disease burden of dengue in southeast Asia[J]. PLoS Negl Trop Dis, 2013, 7(2): e2055. DOI:10.1371/journal.pntd.0002055 |
| [9] |
Anderson KB, Chunsuttiwat S, Nisalak A, et al. Burden of symptomatic dengue infection in children at primary school in Thailand:a prospective study[J]. Lancet, 2007, 369(9571): 1452-1459. DOI:10.1016/S0140-6736(07)60671-0 |
| [10] |
中华医学会感染病学分会, 中华医学会热带病与寄生虫学分会, 中华中医药学会急诊分会. 中国登革热临床诊断和治疗指南[J]. 中华临床感染病杂志, 2018, 11(5): 321-329. Chinese Association of Infectious Diseases, Chinese Association of Tropical Diseases and Parasitology, Chinese Association of Traditional Chinese Medicine. Chinese guidelines for diagnosis and treatment of dengue fever[J]. Chin J Clin Infect Dis, 2018, 11(5): 321-329. DOI:10.3760/cma.j.issn.1674-2397.2018.05.001 |
| [11] |
Luz PM, Grinsztejn B, Galvani AP. Disability adjusted life years lost to dengue in Brazil[J]. Trop Med Int Health, 2009, 14(2): 237-246. DOI:10.1111/j.1365-3156.2008.02203.x |
| [12] |
Undurraga EA, Betancourt-Cravioto M, Ramos-Castañeda J, et al. Economic and disease burden of dengue in Mexico[J]. PLoS Negl Trop Dis, 2015, 9(3): e0003547. DOI:10.1371/journal.pntd.0003547 |
| [13] |
Undurraga EA, Edillo FE, Erasmo JNV, et al. Disease burden of dengue in the Philippines:adjusting for underreporting by comparing active and passive dengue surveillance in Punta Princesa, Cebu city[J]. Am J Trop Med Hyg, 2017, 96(4): 887-898. DOI:10.4269/ajtmh.16-0488 |
| [14] |
孟凤霞, 王义冠, 冯磊, 等. 我国登革热疫情防控与媒介伊蚊的综合治理[J]. 中国媒介生物学及控制杂志, 2015, 26(1): 4-10. Meng FX, Wang YG, Feng L, et al. Review on dengue prevention and control and integrated mosquito management in China[J]. Chin J Vector Biol Control, 2015, 26(1): 4-10. DOI:10.11853/j.issn.1003.4692.2015.01.002 |
| [15] |
刘起勇. 我国登革热流行新趋势、防控挑战及策略分析[J]. 中国媒介生物学及控制杂志, 2020, 31(1): 1-6. Liu QY. Dengue fever in China:new epidemical trend, challenges and strategies for prevention and control[J]. Chin J Vector Biol Control, 2020, 31(1): 1-6. DOI:10.11853/j.issn.1003.8280.2020.01.001 |
| [16] |
Wichmann O, Yoon IK, Vong S, et al. Dengue in Thailand and Cambodia:an assessment of the degree of underrecognized disease burden based on reported cases[J]. PLoS Negl Trop Dis, 2011, 5(3): e996. DOI:10.1371/journal.pntd.0000996 |