 2023, Vol. 34
2023, Vol. 34扩展功能
文章信息
- 王艳旭, 赵继民, 刘翠玉, 吴晓敏, 王彦富, 肖虹
- WANG Yan-xu, ZHAO Ji-min, LIU Cui-yu, WU Xiao-min, WANG Yan-fu, XIAO Hong
- 黑龙江省佳木斯市2004-2021年肾综合征出血热流行特征及发病趋势预测
- Epidemiological characteristics and trend prediction of hemorrhagic fever with renal syndrome in Jiamusi, Heilongjiang, China, 2004-2021
- 中国媒介生物学及控制杂志, 2023, 34(4): 536-541
- Chin J Vector Biol & Control, 2023, 34(4): 536-541
- 10.11853/j.issn.1003.8280.2023.04.017
-
文章历史
- 收稿日期: 2023-02-08


2 黑龙江省疾病预防控制中心, 黑龙江 哈尔滨 150081
2 Heilongjiang Province Center for Disease Control and Prevention, Harbin, Heilongjiang 150081, China
肾综合征出血热(hemorrhagic fever with renal syndrome,HFRS)是自然疫源性疾病[1-2],由汉坦病毒引起,《中华人民共和国传染病防治法》将其归为乙类传染病,其主要传染源和自然宿主为鼠类等啮齿动物。该疾病病情重、波及范围广、病死率高,临床上以出血、肾脏损害和发热为主要表现[3-4]。我国报告HFRS数占全世界90%以上[5],不仅威胁群众的身体健康和生命安全[6],还严重影响社会经济发展,已成为社会主要公共卫生问题之一[7]。黑龙江省HFRS近3年发病率一直位居全国前2位,为高发省份,疫情形势复杂。佳木斯市是黑龙江省HFRS高发地区,2004-2017年HFRS年均发病率为15.33/10万,明显高于全国多地[8]。近年来虽然发病率逐渐下降,但佳木斯市在全国仍属于HFES高发地区。本文通过整理、分析2004-2021年佳木斯市HFRS疫情数据,对该病进行流行病学描述,并建立差分整合移动平均自回归模型(autoregressive integrated moving average model,ARIMA)最优时间序列模型,预测其发展趋势,为HFRS防控提供依据。
1 材料与方法 1.1 资料来源2004-2021年佳木斯市HFRS发病资料来源于中国疾病预防控制信息系统。人口学资料来自《佳木斯市经济统计年鉴》。
1.2 方法用描述流行病学方法分析2004-2021年佳木斯市HFRS疫情资料;用Excel 2010和SPSS 22.0软件对数据进行整理及统计分析,率的比较采用χ2检验,并用SPSS 22.0软件构建ARIMA模型进行时间序列分析及趋势预测;用Eview 10.0软件进行扩展的迪基-福勒检验(augmented Dickey-Fuller test,ADF)。检验水准α=0.05。
2 结果 2.1 流行概况2004-2021年佳木斯市共报告HFRS病例5 772例,年均发病率为13.15/10万。2006年发病率最高,为34.75/10万,2021年最低,为4.31/10万。HFRS发病率总体呈下降趋势。见图 1。

|
| 图 1 2004-2021年黑龙江省佳木斯市肾综合征出血热发病数和发病率变化趋势 Figure 1 Changing trend of number of hemorrhagic fever with renal syndrome cases and the incidence rate in Jiamusi, Heilongjiang, 2004-2021 |
| |
HFRS以11月发病人数最多,共988例,占17.10%;9月最少,共191例,占3.31%。时间分布有2个高峰:5-7月的春夏季小高峰和10-12月的秋冬季大高峰;5-7月HFRS共发病1
758例,占30.46%,10-12月共2 052例,占35.55%。HFRS每年发病趋势大致相同,但并不完全一致,2004、2015和2021年的春夏高峰均在5月,2019年为7月,其余年度春夏高峰均在6月,各年度秋冬季高峰均在11月。见图 2。

|
| 图 2 2004-2021年黑龙江省佳木斯市肾综合征出血热时间分布热图 Figure 2 Time distribution heatmap of hemorrhagic fever with renal syndrome in Jiamusi, Heilongjiang, 2004-2021 |
| |
各县(市、区)均有HFRS病例报告,年均发病率前2位依次为同江(23.92/10万)和抚远市(21.47/10万),最低为前进区(4.78/10万),各县(市、区)HFRS年均发病率差异有统计学意义(χ2=994.541,P < 0.001)。各县(市、区)发病情况随时间的变化大多为2004年开始呈上升趋势,2008年下降明显且之后逐年下降,但同江和抚远市2012-2014和2020年、富锦市2017年、抚远市2016年分别出现了小高峰。
2.2.3 人群分布 2.2.3.1 性别分布共报告男性病例4 531例,占78.50%,女性1 241例,占21.50%,男女性别比例为3.65∶1。年均发病率男性为20.39/10万,女性为5.72/10万,男性高于女性(χ2=1 797.142,P < 0.001)。2004-2021年各年度男性发病率均高于女性(均P < 0.001)。
2.2.3.2 年龄分布各年龄组HFRS年均发病率比较,差异有统计学意义(χ2=1 191.137,P < 0.001),30~34岁年龄组年均发病率最高,为19.28/10万,0~4岁最低,为0.50/10万。从发病年龄构成看,HFRS发病主要集中在15~69岁,合计占比为95.88%。35~39岁年龄组构成比最高,占13.95%,其次为40~44岁年龄组,占13.22%。
2.2.3.3 职业分布HFRS患者职业发病数前5位依次为农民4 013例,占69.53%;工人328例,占5.68%;家务及待业327例,占5.67%;学生193例,占3.34%;民工181例,占3.14%。各年职业构成农民占比较高,始终在59.26%以上;从2017年开始,工人、离退休及家务待业人员占比有升高趋势。职业发病数随时间变化情况为:农民和工人2007年最高,家务及待业、学生和民工2006年最高,以后逐年均呈下降趋势。
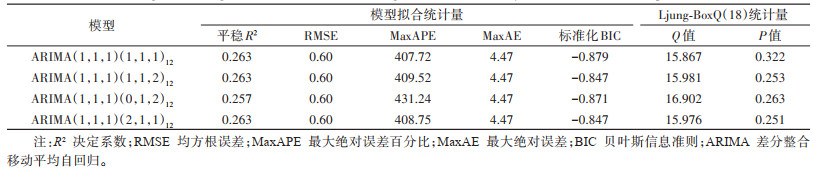
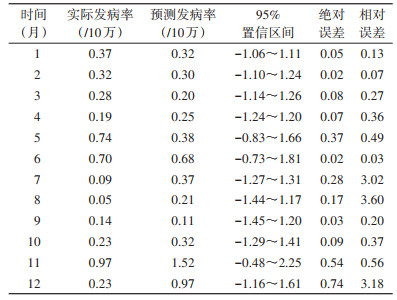
2.3 时间序列分析及预测绘制2004-2021年佳木斯市HFRS月发病率序列图,将不平稳序列进行一阶差分和一阶季节性差分,ADF检验其平稳性,有统计学意义(t=-6.542,P < 0.001)。模型为以12个月为周期的季节乘积模型:ARIMA(p,1,q)(P,1,Q)12。对平稳后的时间序列作自相关和偏自相关分析,确定q为1,p为1,P、Q取值一般在0~2,将各阶数从低阶到高阶进行全面组合,并对模型进行参数估计和白噪声检验,共筛选出4种备选模型,选取贝叶斯信息准则(Bayesian information criterions,BIC)-0.879最小者为最优模型,确定ARIMA(1,1,1)(1,1,1)12为最优模型。绘制最优模型残差序列自相关系数(autocorrelation function,ACF)和偏自相关系数(partial autocorrelation function,PAF)图,结果均在95%置信区间内,均P > 0.05(表 1)。应用ARIMA(1,1,1)(1,1,1)12模型对佳木斯市2021年1-12月HFRS发病率进行预测,并与实际月发病率进行比较,平均绝对百分比误差为43.67%,且实际月发病率均落在预测月发病率的95%置信区间内(表 2)。应用ARIMA(1,1,1)(1,1,1)12模型预测佳木斯市2022年HFRS各月发病率,结果显示2022年HFRS发病率有小幅升高趋势,但仍处于较低水平。见图 3。
|
|

|
| 图 3 2022年黑龙江省佳木斯市肾综合征出血热发病率预测 Figure 3 Prediction of incidence rate of hemorrhagic fever with renal syndrome in Jiamusi, Heilongjiang, 2022 |
| |
2004-2021年佳木斯市HFRS发病率由2004年的22.60/10万逐渐升高至2006年的34.75/10万,然后大幅下降至2021年的4.31/10万,全市HFRS疫情总体呈下降趋势,原因可能是健康科普知识的宣传,促进人们养成了良好的卫生习惯;疫苗接种的实施,增强了重点人群的免疫力;通过开展灭鼠等环境整治措施,生活环境得到了改善;通过监测疫情,防控方案能够及时制定,有利于疫情的控制[9]。但年均发病率仍明显高于黑龙江省哈尔滨市[10]、山东省淄博市[11]、广东省深圳市[12]和江西省抚州市[13]等地,因此还需加强防控工作力度。
HFRS整体发病呈散发,且具有明显季节性,呈秋冬峰高于春夏峰的双峰型分布,这一研究结果与全国及多地省市同期报道结果一致[14-16]。春夏季高发可能是由于正值农忙时节,气温回升,农业和户外活动增多,同时鼠类繁殖加快,因此人群感染和发病的机会增加。秋季收取农作物,人们饮食环境容易受到鼠类排泄物或分泌物污染;冬季天气寒冷,户外活动减少,鼠类因食物紧缺,觅食困难,从而将活动范围扩大至室内,增加了人们感染发病的概率[17]。发病较高县(市、区)为边境口岸的同江和抚远市,可能原因为该地区以农业为主,辖区内有大面积农场,卫生条件较差,人们田间劳作容易暴露于鼠类生活环境;群众不清楚HFRS防控知识,对其危害性不重视,缺乏自我防护意识,主动接种疫苗意愿较弱。在报告的HFRS病例中,男性年均发病率和发病数均高于女性,这一研究结果与沈阳市[18]、云南省[19]等结果一致。原因可能是男女社会分工不同,男性是从事农业生产或其他野外工作的主要劳动力,接触鼠类及其排泄物与分泌物的概率增加,相对于女性致病因素暴露机会多,容易发病。HFRS发病人群主要为15~69岁之间的青壮年,其中35~39岁年龄组构成比最高,职业以农民为主,这一研究结果与全国报道结果一致[20-22],该人群是务农、生产的主要劳动力,与宿主接触的概率增加。根据流行特征结果,提示佳木斯市HFRS预防控制措施应根据时间制定,提前做好2个高峰期的防控工作;根据地区制定,对于发展农业的县(市、区),要重点宣传、教育,开展预防接种工作及环境整治措施,尤其是15~69岁男性青壮年农民,提高这些人群对疾病的认知程度;大力推广接种HFRS疫苗,并每年进行查漏补种[23],形成有效的免疫保护屏障。
ARIMA模型是一种精确度高且实用性强的短期预测方法[24],在以往许多ARIMA模型研究HFRS发病的文献中,预测均取得了较好的效果。如杨其松等[25]利用2005-2016年宜春市HFRS逐月发病率,得到最优模型ARIMA(0,1,2)(0,1,1)12,平均绝对百分比误差(mean absolute percentage error,MAPE)为15.64%。刘红慧等[26]利用2010-2017年湖北省HFRS各月发病数,得到最优模型ARIMA(0,0,2)(0,1,1)12,MAPE为40%。程聪等[27]利用2014-2019年深圳市HFRS各月发病数,得到最优模型SARIMA(0,1,1)(0,1,1)12,MAPE为33.3%。本研究利用2004-2021年佳木斯市HFRS月发病率,得到最优模型ARIMA(1,1,1)(1,1,1)12,MAPE为43.67%,预测精度相对较高,2021年HFRS发病趋势预测结果表明,实际发病率和预测发病率波动范围一致,且二者绝对误差和相对误差均较低,预测2022年各月HFRS发病率有小幅升高趋势,但仍处于较低水平,实际值始终在模型预测值的95%置信区间内,这一研究结果与全国多地报道结果一致[28-29],说明此模型ARIMA(1,1,1)(1,1,1)12对佳木斯市HFRS发病具有一定预测价值和实际意义。同时,本研究存在一定的局限性,一是疫情资料均来源于各医疗机构上报的信息系统,可能存在漏报现象;二是2020年新型冠状病毒肺炎疫情以来,人民群众积极响应国家抗击疫情的号召,有疫情发生时减少出门,因此减少了与鼠类及其分泌物、排泄物接触的机会,从而可能改变了HFRS实际发病率趋势,使得预测值与实际值有出入。根据国家疾病预防控制局、国家统计局公开数据,2017-2021年全国HFRS发病数分别为11 262、11 966、9 596、8 121和9 483例,发病率分别为0.82、0.86、0.69、0.58和0.67/10万[30-35],2020年全国HFRS发病数、发病率均为近5年来最低,因此,佳木斯市近几年实际发病率很可能受到疫情影响;三是有关部门对HFRS防控越来越重视,大力开展防鼠、灭鼠等环境整治措施及疫苗接种工作,取得了一定的实际效果。
利益冲突 无
| [1] |
Li CP, Cui Z, Li SL, et al. Association between hemorrhagic fever with renal syndrome epidemic and climate factors in Heilongjiang province, China[J]. Am J Trop Med Hyg, 2013, 89(5): 1006-1012. DOI:10.4269/ajtmh.12-0473 |
| [2] |
李兰娟, 任红. 传染病学[M]. 9版. 北京: 人民卫生出版社, 2018: 92-101. Li LJ, Ren H. Infectious diseases[M]. 9th ed. Beijing: People's Medical Publishing House, 2018: 92-101. |
| [3] |
路淋. 2005-2020年辽宁省丹东市肾综合征出血热流行特征分析[J]. 预防医学论坛, 2022, 28(7): 552-554. Lu L. Analysis on epidemiological characteristics of hemorrhagic fever with renal syndrome, Dandong city, Liaoning province, 2005-2020[J]. Prev Med Trib, 2022, 28(7): 552-554. DOI:10.16406/j.pmt.issn.1672-9153.2022.07.017 |
| [4] |
朱珊, 胡益飞. 血常规在成人肾综合征出血热中的应用价值[J]. 中国卫生检验杂志, 2021, 31(16): 2006-2010. Zhu S, Hu YF. Application value of complete blood count in adult hemorrhagic fever with renal syndrome[J]. Chin J Health Lab Technol, 2021, 31(16): 2006-2010. |
| [5] |
陈俊江, 国天赐, 宋姝璇, 等. 中国肾综合征出血热流行特征及时空分析模型进展[J]. 中华流行病学杂志, 2020, 41(10): 1735-1740. Chen JJ, Guo TC, Song SX, et al. Epidemiological characteristics and the development of spatiotemporal analysis models on hemorrhagic fever with renal syndrome in China[J]. Chin J Epidemiol, 2020, 41(10): 1735-1740. DOI:10.3760/cma.j.cn112338-20191108-00794 |
| [6] |
郑兆磊. 山东省肾综合征出血热流行特征与疫源地现状分析[D]. 济南: 山东大学, 2019. Zheng ZL. The analysis of current situation of epidemic foci and epidemiological characteristics of hemorrhagic fever with renal syndrome in Shandong province[D]. Ji'nan: Shandong University, 2019. (in Chinese) |
| [7] |
Lin HL, Zhang ZT, Lu L, et al. Meteorological factors are associated with hemorrhagic fever with renal syndrome in Jiaonan county, China, 2006-2011[J]. Int J Biometeorol, 2014, 58(6): 1031-1037. DOI:10.1007/s00484-013-0688-1 |
| [8] |
吴晓敏, 王艳旭, 包名家, 等. 佳木斯市2004-2017年肾综合征出血热流行病学特征及疫苗效果[J]. 实用预防医学, 2020, 27(3): 300-302. Wu XM, Wang YX, Bao MJ, et al. Epidemiological characteristics of hemorrhagic fever with renal syndrome and effect of vaccination in Jiamusi city, 2004-2017[J]. Pract Prev Med, 2020, 27(3): 300-302. DOI:10.16462/j.cnki.zhjbkz.2019.02.013 |
| [9] |
王敬磊, 赵亚双. 1949-2012年佳木斯市肾综合征流行性出血热流行特征分析[J]. 中华疾病控制杂志, 2015, 19(2): 211-212. Wang JL, Zhao YS. Analysis of the epidemiological characteristics of epidemic hemorrhagic fever with renal syndrome in Jiamusi, 1949-2012[J]. Chin J Dis Control Prev, 2015, 19(2): 211-212. DOI:10.16462/j.cnki.zhjbkz.2015.02.029 |
| [10] |
冯茜, 唐道洲, 李世娥, 等. 2013-2017年哈尔滨市肾综合征出血热流行特征分析[J]. 现代预防医学, 2019, 46(12): 2122-2124, 2178. Feng Q, Tang DZ, Li SE, et al. Epidemicological characteristics of hemorrhagic fever with renal syndrome in Harbin from 2013 to 2017[J]. Mod Prev Med, 2019, 46(12): 2122-2124, 2178. |
| [11] |
王玲, 张艳, 张玲, 等. 2015-2018年淄博市肾综合征出血热流行特征和宿主动物监测[J]. 中华疾病控制杂志, 2020, 24(2): 237-240. Wang L, Zhang Y, Zhang L, et al. Analysis of epidemiological characteristics and surveillance result of host animal on hemorrhagic fever with renal syndrome in Zibo city from 2015 to 2018[J]. Chin J Dis Control Prev, 2020, 24(2): 237-240. DOI:10.16462/j.cnki.zhjbkz.2020.02.022 |
| [12] |
王敬忠, 廖异, 程聪. 深圳市2010-2019年肾综合征出血热流行病学特征[J]. 中国热带医学, 2021, 21(3): 244-246. Wang JZ, Liao Y, Cheng C. Epidemiologic characteristics of hemorrhagic fever with renal syndrome in Shenzhen, 2010-2019[J]. China Trop Med, 2021, 21(3): 244-246. DOI:10.13604/j.cnki.46-1064/r.2021.03.10 |
| [13] |
吴斐琳, 上官致洋, 朱小康, 等. 2011-2016年抚州市肾综合征出血热流行特征分析[J]. 现代预防医学, 2018, 45(2): 204-207, 233. Wu FL, Shangguan ZY, Zhu XK, et al. Analysis on the epidemiological characteristics of hemorrhagic fever with renal syndrome in Fuzhou in 2011-2016[J]. Mod Prev Med, 2018, 45(2): 204-207, 233. |
| [14] |
王芹, 李建东, 张全福, 等. 2014年全国肾综合征出血热监测总结和疫情分析[J]. 疾病监测, 2016, 31(3): 192-199. Wang Q, Li JD, Zhang QF, et al. Surveillance for hemorrhagic fever with renal syndrome in China, 2014[J]. Dis Surveill, 2016, 31(3): 192-199. DOI:10.3784/j.issn.1003-9961.2016.03.005 |
| [15] |
王笑辰, 刘文东, 秦圆方, 等. 江苏省2011-2016年肾综合征出血热流行特征及时空聚类分析[J]. 中华疾病控制杂志, 2017, 21(10): 1057-1060, 1065. Wang XC, Liu WD, Qin YF, et al. Epidemiological characteristics and temporal-spatial clustering analysis on hemorrhagic fever with renal syndrome in Jiangsu province, 2011-2016[J]. Chin J Dis Control Prev, 2017, 21(10): 1057-1060, 1065. DOI:10.16462/j.cnki.zhjbkz.2017.10.021 |
| [16] |
华华, 陈淑红, 杨明, 等. 2007-2016年黑龙江省肾综合征出血热疫情分析[J]. 现代预防医学, 2017, 44(22): 4033-4035, 4041. Hua H, Chen SH, Yang M, et al. Analysis on the prevalence of hemorrhagic fever with renal syndrome in Heilongjiang province from 2007 to 2016[J]. Mod Prev Med, 2017, 44(22): 4033-4035, 4041. |
| [17] |
张琼娜, 段春丽, 张绍琼, 等. 2009-2019年祥云县流行性出血热流行特征分析[J]. 国际病毒学杂志, 2021, 28(1): 28-31. Zhang QN, Duan CL, Zhang SQ, et al. Epidemiology characteristics of epidemic hemorrhagic fever in Xiangyun county from 2009 to 2019[J]. Int J Virol, 2021, 28(1): 28-31. DOI:10.3760/cma.j.issn.1673-4092.2021.01.007 |
| [18] |
张春青, 戴孟阳. 2013-2017年沈阳市肾综合征出血热流行特征分析[J]. 预防医学论坛, 2018, 24(9): 688-690. Zhang CQ, Dai MY. Analysis on epidemiological characteristics of hemorrhagic fever with renal syndrome, Shenyang city, 2013-2017[J]. Prev Med Trib, 2018, 24(9): 688-690. DOI:10.16406/j.pmt.issn.1672-9153.2018.09.015 |
| [19] |
周济华, 张云智, 章域震, 等. 云南省2012-2020年肾综合征出血热流行特征分析[J]. 中国媒介生物学及控制杂志, 2021, 32(6): 715-719. Zhou JH, Zhang YZ, Zhang YZ, et al. Epidemiological characteristics of hemorrhagic fever with renal syndrome in Yunnan province, China, 2012-2020[J]. Chin J Vector Biol Control, 2021, 32(6): 715-719. DOI:10.11853/j.issn.1003.8280.2021.06.012 |
| [20] |
傅明慧, 杨华富. 2004-2012年全国流行性出血热流行特征分析[J]. 中国卫生产业, 2014, 11(28): 35-36. Fu MH, Yang HF. Epidemiological characteristics of epidemic hemorrhagic fever in China from 2004 to 2012[J]. China Health Ind, 2014, 11(28): 35-36. DOI:10.16659/j.cnki.1672-5654.2014.28.042 |
| [21] |
王璟. 大庆市2005-2015年肾综合征出血热疫情分析[J]. 中国公共卫生管理, 2017, 33(2): 230-232. Wang J. Epidemiological analysis of hemorrhagic fever with renal syndrome in Daqing, 2005-2015[J]. Chin J Public Health Manag, 2017, 33(2): 230-232. DOI:10.19568/j.cnki.23-1318.2017.02.025 |
| [22] |
马涛, 谢国祥, 徐庆, 等. 2011-2016年南京市肾综合征出血热流行特征分析[J]. 现代预防医学, 2017, 44(23): 4231-4234, 4247. Ma T, Xie GX, Xu Q, et al. Epidemiological characteristics of hemorrhagic fever with renal syndrome, Nanjing, 2011-2016[J]. Mod Prev Med, 2017, 44(23): 4231-4234, 4247. |
| [23] |
董建凤, 常方媛, 赵久飞, 等. 2007-2018年青岛市黄岛区肾综合征出血热流行特征分析[J]. 预防医学论坛, 2020, 26(4): 287-289. Dong JF, Chang FY, Zhao JF, et al. Analysis on the epidemiological characteristics of hemorrhagic fever with renal syndrome, Huangdao district, Qingdao city, 2007-2018[J]. Prev Med Trib, 2020, 26(4): 287-289. DOI:10.16406/j.pmt.issn.1672-9153.2020.04.014 |
| [24] |
郑名烺. 湖北省麻城市1984-2008年自杀死亡水平趋势分析及ARIMA预测研究[D]. 武汉: 华中科技大学, 2011. DOI: http://dx.doi.org/10.7666/d.D231096. Zheng ML. Long-term trend analysis on suicide in Macheng city from 1984 to 2008 and predictive applications of ARIMA model[D]. Wuhan: Huazhong University of Science and Technology, 2011. DOI: http://dx.doi.org/10.7666/d.D231096.(in Chinese) |
| [25] |
杨其松, 朱蒙曼, 张天琛, 等. ARIMA模型在宜春市肾综合征出血热发病率预测中的应用[J]. 中国卫生统计, 2018, 35(5): 713-715, 719. Yang QS, Zhu MM, Zhang TC, et al. Application of ARIMA model in predicting the incidence of hemorrhagic fever with renal syndrome in Yichun city[J]. Chin J Health Stat, 2018, 35(5): 713-715, 719. |
| [26] |
刘红慧, 刘天, 邢学森. 2010-2017年湖北省肾综合征出血热流行特征及时空分布与发病趋势预测[J]. 疾病监测, 2019, 34(1): 21-26. Liu HH, Liu T, Xing XS. Epidemiological characteristics, spatial and temporal distribution and incidence trend of hemorrhagic fever with renal syndrome in Hubei, 2010-2017[J]. Dis Surveill, 2019, 34(1): 21-26. DOI:10.3784/j.issn.1003-9961.2019.01.007 |
| [27] |
程聪, 陈志高, 李媛, 等. 2014-2019年深圳市肾综合征出血热疫情流行特征及趋势预测分析[J]. 医学动物防制, 2021, 37(6): 517-521. Cheng C, Chen ZG, Li Y, et al. Epidemiological characteristics and trend prediction on hemorrhagic fever with renal syndrome in Shenzhen from 2014 to 2019[J]. J Med Pest Control, 2021, 37(6): 517-521. DOI:10.7629/yxdwfz202106002 |
| [28] |
常楠, 周若冰, 马德龙, 等. 新型冠状病毒肺炎疫情防控措施对中国肾综合征出血热流行的影响研究[J]. 中国媒介生物学及控制杂志, 2023, 34(1): 58-64. Chang N, Zhou RB, Ma DL, et al. Influence of COVID-19 intervention on the epidemic of hemorrhagic fever with renal syndrome in China[J]. Chin J Vector Biol Control, 2023, 34(1): 58-64. DOI:10.11853/j.issn.1003.8280.2023.01.011 |
| [29] |
付仁龙, 郑卫青, 柳小青, 等. 南昌市2005-2016年肾综合征出血热疫情分析及预测[J]. 实用预防医学, 2019, 26(2): 232-234. Fu RL, Zheng WQ, Liu XQ, et al. Epidemic analysis and prediction of hemorrhagic fever with renal syndrome in Nanchang city, 2005-2016[J]. Pract Prev Med, 2019, 26(2): 232-234. DOI:10.3969/j.issn.1006-3110.2019.02.033 |
| [30] |
中华人民共和国国家卫生健康委员会疾病预防控制局. 2017年全国法定传染病疫情概况[EB/OL]. (2018-02-26)[2022-03-17]. http://www.nhc.gov.cn/jkj/s3578/201802/de926bdb046749abb7b0a8e23d929104.shtml. Disease Prevention and Control Bureau of the National Health Commission of the People's Republic of China. Epidemic situation of notifiable infectious diseases in China in 2017[EB/OL]. (2018-02-26)[2022-03-17]. http://www.nhc.gov.cn/jkj/s3578/201802/de926bdb046749abb7b0a8e23d929104.shtml. (in Chinese) |
| [31] |
中华人民共和国国家卫生健康委员会. 2018年全国法定传染病疫情概况[J]. 中华人民共和国国家卫生健康委员会公报, 2019(3): 38-40. National Health Commission of the People's Republic of China. Survey of notifiable infectious diseases in China in 2018[J]. Gazette Natl Health Commiss, 2019(3): 38-40. |
| [32] |
中华人民共和国国家卫生健康委员会疾病预防控制局. 2019年全国法定传染病疫情概况[EB/OL]. (2020-04-20)[2022-03-17]. http://www.nhc.gov.cn/jkj/s3578/202004/b1519e1bc1a944fc8ec176db600f68d1.shtml. Disease Prevention and Control Bureau of the National Health Commission of the People's Republic of China. Epidemic situation of notifiable infectious diseases in China in 2019[EB/OL]. (2020-04-20)[2022-03-17]. http://www.nhc.gov.cn/jkj/s3578/202004/b1519e1bc1a944fc8ec176db600f68d1.shtml. (in Chinese) |
| [33] |
中华人民共和国国家卫生健康委员会疾病预防控制局. 2020年全国法定传染病疫情概况[J]. 中国病毒病杂志, 2021(11): 111. Disease Prevention and Control Bureau of the National Health Commission of the People's Republic of China. Survey of notifiable infectious diseases in China in 2020[J]. Chin J Viral Dis, 2021(11): 111. |
| [34] |
中华人民共和国国家卫生健康委员会疾病预防控制局. 2021年12月全国法定传染病疫情概况[EB/OL]. (2022-01-21)[2022-03-17]. http://www.nhc.gov.cn/jkj/s3578/202201/ad8a655dec234bf78d42ece54f5dd282.shtml. Disease Prevention and Control Bureau of the National Health Commission of the People's Republic of China. Survey of notifiable infectious diseases in China in December 2021[EB/OL]. (2022-01-21)[2022-03-17]. http://www.nhc.gov.cn/jkj/s3578/202201/ad8a655dec234bf78d42ece54f5dd282.shtml. (in Chinese) |
| [35] |
王萍萍. 人口总量保持增长城镇化水平稳步提升[EB/OL]. (2022-01-18)[2022-03-17]. http://www.ce.cn/xwzx/gnsz/gdxw/202201/18/t20220118_37264987.shtml. Wang PP. The total population keeps growing and the level of urbanization is steadily improving[EB/OL]. (2022-01-18)[2022-03-17]. http://www.ce.cn/xwzx/gnsz/gdxw/202201/18/t20220118_37264987.shtml. (in Chinese) |