 2023, Vol. 34
2023, Vol. 34扩展功能
文章信息
- 常楠, 周若冰, 马德龙, 张璐, 韦晓慧, 王君, 刘起勇
- CHANG Nan, ZHOU Ruo-bing, MA De-long, ZHANG Lu, WEI Xiao-hui, WANG Jun, LIU Qi-yong
- 新型冠状病毒肺炎疫情防控措施对中国肾综合征出血热流行的影响研究
- Influence of COVID-19 intervention on the epidemic of hemorrhagic fever with renal syndrome in China
- 中国媒介生物学及控制杂志, 2023, 34(1): 58-64
- Chin J Vector Biol & Control, 2023, 34(1): 58-64
- 10.11853/j.issn.1003.8280.2023.01.011
-
文章历史
- 收稿日期: 2022-08-24




2 中国疾病预防控制中心传染病预防控制所媒介生物控制室, 传染病预防控制国家重点实验室, 北京 102206;
3 山东第一医科大学, 山东 济南 250000
2 State Key Laboratory of Infectious Disease Prevention and Control, Department of Vector Biology and Control, National Institute for Communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 102206, China;
3 Shandong First Medical University, Ji'nan, Shandong 250000, China
肾综合征出血热(hemorrhagic fever with renal syndrome,HFRS)又称流行性出血热,是一种由汉坦病毒(Hantavirus)感染所致的媒介传染病。我国汉坦病毒的主要宿主动物是黑线姬鼠(Apodemus agrarius)和褐家鼠(Rattus norvegicus)[1],带病毒啮齿动物通过气溶胶排泄物传播病毒,易感人群可通过呼吸道、消化道和直接接触等多种途径被感染。患者会出现发热、出血和肾功能衰竭等临床症状[2]。HFRS是我国法定报告传染病中发病率及死亡率最高的媒介生物传染病之一,是我国的重要公共卫生问题[3]。
研究证据显示,2020年新型冠状病毒肺炎(新冠肺炎)疫情暴发以来,我国采取的非药物干预政策使多种法定报告传染病的发病率发生了显著下降,其中也包括登革热等媒介生物传染病[4-5]。本研究旨在分析我国2006-2021年HFRS的流行特征,并通过自回归积分移动平均(autoregressive integrated moving average,ARIMA)模型探究新冠肺炎疫情相关防疫政策对HFRS发病数及发病率的影响,为后续制定HFRS的防控措施及对其流行特征的进一步研究提供证据,具有重要参考意义。
1 材料与方法 1.1 数据来源数据来源于中国疾病预防控制中心传染病报告信息管理系统,包括2006年1月1日-2021年12月31日我国HFRS的发病数、死亡数,病例性别、年龄、职业等。
1.2 研究方法本研究应用描述性流行病学方法,通过Excel 2019和R 4.0.4建立数据库,并使用SPSS 22.0软件对2006-2021年我国HFRS流行特征进行统计分析。使用2006-2019年的病例数据建立ARIMA模型,预测2020-2021年的发病数,将预测值与实际观测值进行比较,确认新冠肺炎疫情防控政策是否对HFRS的传播产生影响。检验水准α=0.05。
ARIMA模型是一种差分后的自回归积分移动平均过程,也是拟合时间序列数据的一个非常有效的工具,它结合了自回归(历史时期变量值对未来值的影响)和移动平均线(误差项的累加)方法,通过追踪过去变量及其随机项的值来预测未来时期的该变量值[6-7]。因HFRS发病数有明显的季节性,选择拟合(p,d,q)(P,D,Q)s模型,其中p是自回归的阶数,d是差分阶数,q是移动平均的阶数,P、D、Q分别代表季节自回归、季节差分和季节移动平均的阶数,s为季节周期长度,取值12。本研究选择使用R软件进行模拟[8],首先确定时间序列平稳,即序列的统计性质不随时间推移而改变,然后检验数据是否为非白噪声,之后结合R语言和时间序列的自相关(ACF)、偏自相关(PACF)图选择合适的(p,d,q)(P,D,Q)s值,最后通过赤池信息量准则(Akaike information criterion,AIC)选择最佳模型后进行拟合评估,比较最适模型的预测值与实际观测值,分析差异是否有统计学意义。
2 结果 2.1 HFRS流行特征 2.1.1 时间分布2006-2021年我国共报告HFRS 172 646例,死亡病例数为1 490例,其中2006年的发病数和死亡数均为最高(图 1)。在Mann-Kendall趋势检验的结果中,发病数和死亡数的Z值均为负,即呈下降趋势,发病数的P值为0.224,下降趋势不显著,死亡病例数P < 0.001,为显著降低。HFRS的流行具有明显的季节性特征,在国家尺度上,1年中有2个发病高峰,小高峰出现在5-6月,大高峰出现在11月。见图 2。

|
| 图 1 2006-2021年中国肾综合征出血热报告发病数及死亡数 Figure 1 Reported numbers of hemorrhagic fever with renal syndrome cases and deaths in China, 2006-2021 |
| |

|
| 图 2 2006-2021年各月中国肾综合征出血热报告病例分布 Figure 2 Reported cases of hemorrhagic fever with renal syndrome in each month in China, 2006-2021 |
| |
2006年以来,我国大陆31个省级行政区均有HFRS病例报告,主要集中在东北地区、陕西以及山东省(图 3)。其中东北地区作为HFRS的传统高发区病例数有所降低,但陕西和山东省仍存在暴发流行。另外,河南、湖北、福建、广东、四川、云南省的病例也有增加。见图 4。

|
| 图 3 2006-2021年中国肾综合征出血热报告病例空间分布 Figure 3 Spatial distribution of reported cases of hemorrhagic fever with renal syndrome in China, 2006-2021 |
| |

|
| 图 4 2006-2021年中国肾综合征出血热病例空间分布变化 Figure 4 Spatial distribution change of reported cases of hemorrhagic fever with renal syndrome in China from 2006 to 2021 |
| |
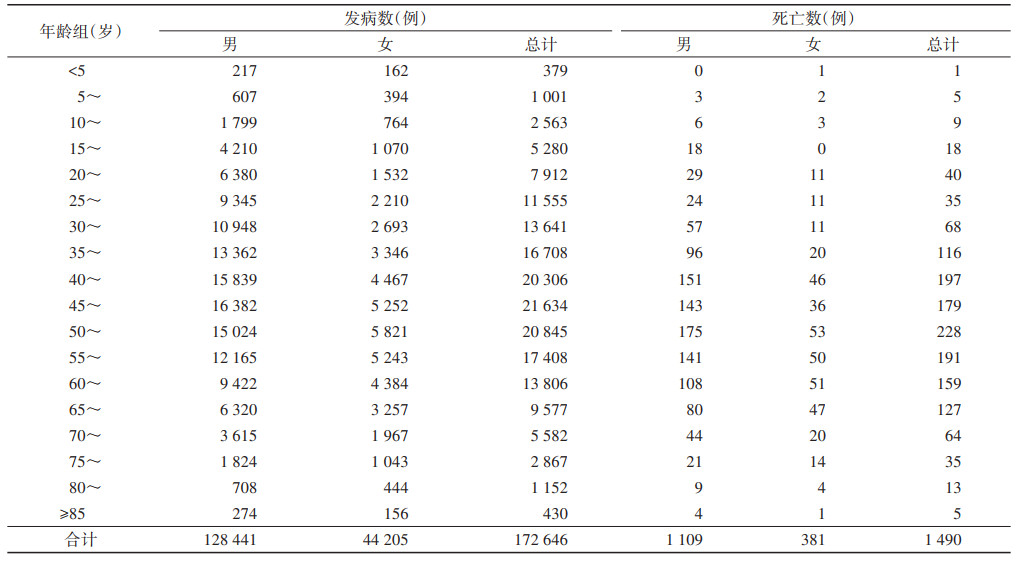
我国2006-2021年HFRS男性患者共128 441例,死亡1 109例,分别占发病总数的74.40%和死亡总数的74.43%,女性患者44 205例,死亡病例381例,分别占25.60%和25.57%。男性高发年龄段为35~49岁,占男性病例的35.49%,女性高发年龄段为45~59岁,占女性病例的36.91%(表 1)。经χ2检验,不同性别的发病年龄构成比差异有统计学意义(χ2=2 802.807,P < 0.001)。发病人群中有67.81%的病例职业为农民。见图 5。
|

|
| 图 5 2006-2021年中国肾综合征出血热报告病例职业分布 Figure 5 Occupational distribution of hemorrhagic fever with renal syndrome cases in China, 2006–2021 |
| |
首先将2006-2019年各月的HFRS发病数据转化为时间序列(图 6),对其进行平稳性检验,经ADF检验,P < 0.01,显示序列平稳。然后进行Ljung-Box检验以确认其是否为白噪声,检验结果P < 0.01,显示为非白噪声序列,可以构建ARIMA模型进行预测。结合R语言的auto.arima函数结果以及时间序列的ACF、PACF图(图 7),最后基于最小赤池信息量准则(AIC)确定最优模型为(2,0,2)(1,1,0)12。

|
| 图 6 2006-2019年中国肾综合征出血热报告病例发病时间序列图 Figure 6 Time series of reported cases of hemorrhagic fever with renal syndrome in China, 2006–2019 |
| |

|
| 图 7 2016-2019年肾综合征出血热病例数时间序列自相关与偏自相关图 Figure 7 The ACF and PACF diagram of time series of hemorrhagic fever with renal syndrome cases in China, 2006-2019 |
| |
从拟合模型残差的正态Q-Q图可以看出残差服从正态分布(图 8),同时进行白噪声检验,Ljung-Box检验结果表示残差具有随机性(χ2=0.088,P=0.767),模型有效。且模型的平均绝对百分比误差为11.29,拟合效果好。

|
| 图 8 肾综合征出血热ARIMA模型残差Q-Q图 Figure 8 The Q-Q diagram of residuals of the autoregressive integrated moving average model for hemorrhagic hemorrhagic fever with renal syndrome |
| |
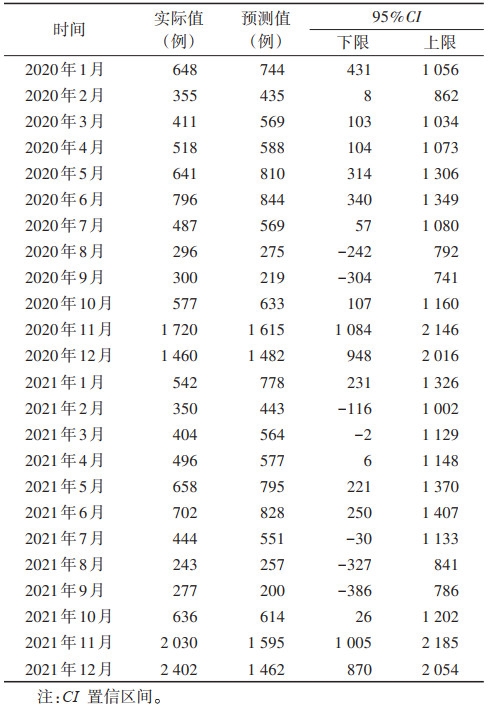
利用ARIMA(2,0,2)(1,1,0)12模型预测我国2020年1月-2021年12月HFRS报告发病数,实际值均在预测值的95%置信区间内(表 2、图 9),没有显著改变。
|

|
| 注:图中实线为实际值,阴影部分为预测值,其中浅色范围为95%置信区间,深色范围为80%置信区间。 图 9 2006-2019年肾综合征出血热病例数及2020-2021年ARIMA模型预测病例数 Figure 9 The reported cases of hemorrhagic fever with renal syndrome cases in 2006-2019 and the predicted number in 2020-2021 by the autoregressive integrated moving average model |
| |
2006年至今,我国HFRS发病趋于平稳,每隔5~10年会出现一个流行高峰,在部分地区(比如陕西省)还存在明显的暴发隐患。目前我国已成功研制出预防效果较好的双价灭活疫苗[9],在江西省宜春市进行的2010-2016年HFRS患者调查中,96.96%的患者未进行过疫苗接种[10]。研究结果显示男性青、中年农民仍是HFRS发病的高危人群,农民的收入水平相对较低,生活条件相对较差,且目前在中国农村,男性青壮年一般为家庭经济来源的主要承担者,一旦患病会将从各方面给整个家庭带来严重的损失。
3.2 新冠肺炎对HFRS的影响在对抗新冠肺炎疫情的过程中,甲型和乙型流感在全球范围内出现显著减少[11],我国采取的针对新冠肺炎疫情的干预措施对许多其他传染病的发病率也产生了影响。本研究首次尝试使用ARIMA模型拟合对比来探究新冠肺炎疫情期间的非药物干预措施对HFRS流行情况是否存在显著影响,结果显示2020-2021年预测值与实际观测值无显著差异,说明在全国尺度上,非药物干预措施并未对HFRS在我国的发病情况产生显著影响。新冠肺炎传播性强,隐匿性高,可以通过飞沫、直接接触、气溶胶和粪-口途径传播。我国通过在公共场所强制佩戴口罩,减少人群聚集,关闭娱乐场所,对疑似感染者和密切接触者采取隔离等措施有效控制了疫情的传播[12]。HFRS是一种通过呼吸道、消化道和直接接触传播的鼠传疾病,革螨和恙螨对鼠间汉坦病毒的传播和保持疫源地有重要作用[13]。HFRS的流行情况受政策影响很大,通过大规模的灭鼠防鼠、提高环境卫生水平、宣传病原体来源、传播途径、疫苗接种等相关知识可以有效预防疾病流行[1, 14]。虽然HFRS和新冠肺炎均可以通过气溶胶传播,但前者主要由鼠传播给人,后者主要为人传人。而我国防控新冠肺炎疫情的主要措施是通过减少人与人之间的联系来降低疾病发生率,可能对居民区以及野外鼠类接触机会并未发生显著影响。同时,人群在居住环境中往往不佩戴口罩,导致患者在家庭接触鼠类感染的情况,防控新冠肺炎的措施可能并未起到保护作用。另外,农民在进行耕种时不佩戴口罩也可能是HFRS疫情未受到显著影响的原因。
综上所述,减少人群聚集、在公共场所佩戴口罩和居家隔离等措施并未对HFRS的流行产生显著影响,防鼠灭鼠、接种疫苗、提高环境卫生水平仍是预防HFRS的重要手段。
利益冲突 无
| [1] |
Zhang YZ, Zou Y, Fu ZF, et al. Hantavirus infections in humans and animals, China[J]. Emerg Infect Dis, 2010, 16(8): 1195-1203. DOI:10.3201/eid1608.090470 |
| [2] |
Cosgriff TM. Hemorrhagic fever with renal syndrome: Four decades of research[J]. Ann Intern Med, 1989, 110(4): 313-316. DOI:10.7326/0003-4819-110-4-313 |
| [3] |
刘起勇. 2005-2020年我国媒介生物传染病报告病例: 流行趋势、防控挑战及应对策略[J]. 中国媒介生物学及控制杂志, 2022, 33(1): 1-7. Liu QY. Reported cases of vector-borne diseases in China, 2005-2020: Epidemic trend, challenges in prevention and control, and related coping strategies[J]. Chin J Vect Biol Control, 2022, 33(1): 1-7. DOI:10.11853/j.issn.1003.8280.2022.01.001 |
| [4] |
Xiao JP, Dai JY, Hu JX, et al. Co-benefits of nonpharmaceutical intervention against COVID-19 on infectious diseases in China: A large population-based observational study[J]. Lancet Reg Health West Pac, 2021, 17: 100282. DOI:10.1016/j.lanwpc.2021.100282 |
| [5] |
Geng MJ, Zhang HY, Yu LJ, et al. Changes in notifiable infectious disease incidence in China during the COVID-19 pandemic[J]. Nat Commun, 2021, 12(1): 6923. DOI:10.1038/s41467-021-27292-7 |
| [6] |
Das RC. Forecasting incidences of COVID-19 using Box-Jenkins method for the period July 12-Septembert 11, 2020: A study on highly affected countries[J]. Chaos Solitons Fractals, 2020, 140: 110248. DOI:10.1016/j.chaos.2020.110248 |
| [7] |
Toğa G, Atalay B, Toksari MD. COVID-19 prevalence forecasting using autoregressive integrated moving average (ARIMA) and Artificial Neural Networks (ANN): Case of Turkey[J]. J Infect Public Health, 2021, 14(7): 811-816. DOI:10.1016/j.jiph.2021.04.015 |
| [8] |
Kabacoff RI. R语言实战(第2版)[M]. 王小宁, 刘撷芯, 黄俊文, 等, 译. 北京: 人民邮电出版社, 2016: 333-339. Kabacoff RI. R in action: Data analysis and graphics with R (2nd ed)[M]. Wang XN, Liu XX, Huang JW, et al, Translation. Beijing: Posts & Telecon Press, 2016: 333-339. (in Chinese) |
| [9] |
刘怀文. 我国流行性出血热的概况[J]. 医药产业资讯, 2006, 3(21): 121-123. Liu HW. General situation of epidemic hemorrhagic fever in China[J]. Med Ind Inf, 2006, 3(21): 121-123. DOI:10.3969/j.issn.1673-7210.2006.21.098 |
| [10] |
杨其松. 2010-2017年宜春市肾综合征出血热时空分布特征与经济负担研究[D]. 南昌: 南昌大学, 2019. Yang QS. Study on spatio-temporal distribution and economic burden of hemorrhagic fever with renal syndrome in Yichun city from 2010 to 2017[D]. Nanchang: Nanchang University, 2019. (in Chinese) |
| [11] |
Koutsakos M, Wheatley AK, Laurie K, et al. Influenza lineage extinction during the COVID-19 pandemic?[J]. Nat Rev Microbiol, 2021, 19(12): 741-742. DOI:10.1038/s41579-021-00642-4 |
| [12] |
Hao XJ, Cheng SS, Wu DG, et al. Reconstruction of the full transmission dynamics of COVID-19 in Wuhan[J]. Nature, 2020, 584(7821): 420-424. DOI:10.1038/s41586-020-2554-8 |
| [13] |
宋干. 新中国流行性出血热防治研究的主要成就[J]. 中华流行病学杂志, 2000, 21(5): 378-382. Song G. The main achievements of epidemic hemorrhagic fever prevention and control in China[J]. Chin J Epidemiol, 2000, 21(5): 378-382. DOI:10.3760/j.issn:0254-6450.2000.05.019 |
| [14] |
吴光华. 近年中国肾综合征出血热流行病学研究进展[J]. 中华流行病学杂志, 2003, 42(5): 413-415. Wu GH. Advances in epidemiology of hemorrhagic fever with renal syndrome in China[J]. Chin J Epidemiol, 2003, 42(5): 413-415. DOI:10.3760/j.issn:0254-6450.2003.05.024 |