 2017, Vol. 32
2017, Vol. 32扩展功能
文章信息
- 郑亚明, 杨娟
- ZHENG Ya-ming, YANG Juan
- 2013-2015年我国手足口病死亡病例社会经济负担估计
- Estimation of social economic burden caused by fatal hand, foot and mouth disease cases in China, 2013-2015
- 疾病监测, 2017, 32(6): 516-520
- Disease Surveillance, 2017, 32(6): 516-520
- 10.3784/j.issn.1003-9961.2017.06.018
-
文章历史
- 收稿日期:2017-04-05




手足口病(hand,foot and mouth disease,HFMD)是由肠道病毒引起的急性发热出疹性疾病,主要病原体为肠道病毒71型(Enterovirus 71,EV71) 和柯萨奇病毒A组16型(Cox A16)[1-3]。手足口病发病人群以≤5岁儿童为主,大多数病例症状较轻,出现发热、口腔疱疹或溃疡,手掌、足底等部位出现皮疹。少数病例会进展为重症,出现无菌性脑膜炎、脑干脑炎、急性弛缓性麻痹、肺出血或肺水肿、心肺功能衰竭等,极少数病例会进展为死亡[4]。2009年以来,全国法定报告传染病中手足口病发病数一直居于首位,而死亡人数位于报告死亡人数的前5位之内[5],给儿童的生命健康带来严重威胁,同时也给患者家庭带来沉重的经济负担。
目前,对于手足口病轻症病例、住院病例及重症病例的经济负担研究较多[6-8],但对死亡病例的研究较少。2013年12月至2014年1月,笔者对全国手足口病死亡病例的直接经济负担进行了调查[9],然而并未评估早亡引起的生产力损失(早亡损失),由于早亡损失是疾病经济负担的重要组成部分,为更全面地评估手足口病死亡病例的经济负担,本研究采用人力资本法计算死亡病例早亡损失,并结合前期调查得到的经济负担,获得2013—2015年我国手足口病死亡病例的社会经济负担。
1 资料与方法1.1 资料来源手足口病死亡病例社会经济负担包括手足口病死亡病例在治疗期间发生的经济负担,包括直接医疗费用(门诊费、住院费、自购药品费)、直接非医疗费用(治疗期间交通费、住宿费等)和间接费用(治疗期间患者及家庭的收入损失)以及早亡损失。各年全国手足口病死亡病例社会经济负担=(人均直接医疗费用+人均直接非医疗费用+人均间接费用+人均早亡损失)ⅹ全国手足口病年度死亡人数。其中,2013—2015年全国手足口病死亡人数来自全国法定传染病报告系统。2013年手足口病死亡病例人均经济负担采用本研究团队前期研究结果[9]。
1.2 调查方式2013年12月至2014年1月,通过电话调查的方式对2012—2013年全国法定报告手足口病死亡病例的家长或看护人进行访谈,获得病例治疗期间的经济负担。本研究采用2014—2015年医疗部门消费价格指数对上述2013年手足口病死亡病例治疗期间经济负担数据进行校正,获得2014—2015年经济负担。
1.3 计算方法早亡损失指在某年龄段死亡的病例从死亡年龄到期望年龄之间损失总收入的现值(present value of lifetime earnings,PVLE),采用人力资本法进行计算[10],公式:

|
式中:s为当前年龄;n为年龄s岁人群的期望寿命;La为年龄a岁时的劳动参与率;Ia为a岁人群年收入;r为贴现率,基线分析时设置为3%,并分别采用0和5%进行敏感性分析。研究使用数据及来源见表 1。
| 参数名称 | 参数值 | 数据来源 |
| 2013—2015手足口病死亡病例 | 见表 2 | 全国法定报告传染病报告系统 |
| 手足口病死亡病例治疗期间经济负担(元/人) | 2013年总费用:14 548 直接医疗费用:11 085;直接非医疗费用:2 384;间接费用:1 079 2014年总费用:14 723;直接医疗费用:11 218;直接非医疗费用:2 413;间接费用:1092 2015年总费用:15 017±9 274;直接医疗费用: 11 443;直接非医疗费用:2 461;间接费用:1 113 | 本研究团队以往研究结果[9] |
| 2013—2015年龄别期望寿命 | 见原始数据- | WHO期望寿命表[11] |
| 不同年龄组人群劳动参与率 | 见原始数据- | 我国2010年人口普查数据[12] |
| 人均国内生产总值(元/人) | 2013年43 852;2014年47 203;2015年50 251 | 国家统计局网站年度数据[13] |
| 医疗部门消费价格指数 | 2014年1.2%;2015年2.0% | 2014—2015国家统计局国民经济和社会发展统计公报[14-15] |
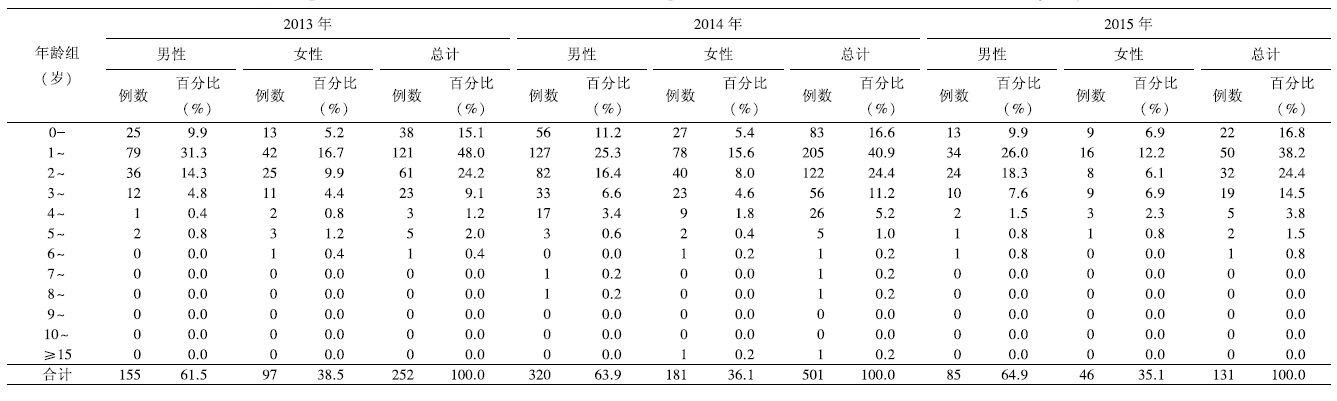
2013—2015年全国手足口病死亡病例分别为252、501和129例,60%以上为男性,以散居儿童为主。从地域分布分析,2013年死亡病例以西南地区最多(85例,占33.7%),2014年华南地区死亡病例最多(211例,占42.1%);2015年西南地区死亡病例最多(51例,占39.5%)。以1~3岁年龄组为主,占全部死亡病例的62.0%~72.0%。死亡病例的年龄及性别分布见表 2。
 |
不同年龄组的手足口病死亡病例早亡损失见表 3。女性的早亡损失比男性高0.2%~1.2%,低年龄的死亡儿童损失预寿命长;由于<16岁儿童的劳动参与率为0,无生产力损失,同时贴现年数多,因而其早亡损失较年龄大的儿童低。随着居民可支配收入的增长,早亡的损失同时增加,2014年死亡病例的早亡损失较2013年增长7.6%~7.7%,2015年较2014年增长6.5%。
| 年龄组 (岁) | 2013年 | 2014年 | 2015年 | |||
| 男性 | 女性 | 男性 | 女性 | 男性 | 女性 | |
| 0~ | 550 979 | 552 113 | 593 082 | 594 304 | 631 825 | 633 088 |
| 1~ | 567 508 | 568 677 | 610 875 | 612 133 | 650 320 | 651 660 |
| 2~ | 584 533 | 585 737 | 629 201 | 630 497 | 669 830 | 671 209 |
| 3~ | 602 069 | 603 309 | 648 077 | 649 412 | 689 925 | 691 346 |
| 4~ | 620 131 | 621 408 | 667 991 | 668 894 | 710 623 | 712 086 |
| 5~ | 634 355 | 637 836 | 682 830 | 686 577 | 728 418 | 730 911 |
| 6~ | 653 386 | 656 971 | 703 315 | 707 174 | 750 270 | 752 838 |
| 7~ | 672 987 | 676 680 | 724 414 | 728 389 | 772 778 | 775 423 |
| 8~ | 693 177 | 696 980 | 746 147 | 750 241 | 795 962 | 798 686 |
| 9~ | 713 972 | 717 890 | 768 531 | 772 748 | 819 840 | 822 646 |
| 10~ | 722 480 | 731 300 | 777 689 | 787 184 | 831 693 | 840 634 |
| ≥15 | 812 681 | 828 795 | 881 009 | 892 129 | 937 898 | 954 979 |
2013—2015年手足口病死亡病例的人均社会经济损失在56.5万~97.0万元之间。全国手足口病死亡病例治疗期间经济负担、早亡损失和总经济负担见表 4。早亡损失占社会经济负担的97.5%~97.7%。2014年死亡病例数较多,早亡损失最高。敏感性分析中,当贴现率设置为0时,2013—2015年早亡损失增长2.0倍,手足口病社会经济负担增长了2.0倍;当贴现率设置为5%时,2013—2015年早亡损失下降了47.2%,社会经济负担下降了46.1%。
| 项目 | 手足口病死亡病例数(例) | ||
| 2013年 (n=252) | 2014年 (n=501) | 2015年 (n=129) | |
| 治疗期间经济负担(万元) | 366.6 | 737.6 | 193.7 |
| 直接医疗费用(万元) | 279.4 | 562.0 | 147.6 |
| 直接非医疗费用(万元) | 60.1 | 120.9 | 31.7 |
| 间接费用(万元) | 27.2 | 54.7 | 14.4 |
| 早亡损失(万元) | |||
| 贴现率为3% | 14 491.9 | 31 159.1 | 8 316.7 |
| 贴现率为0 | 44 043.1 | 94 228.9 | 25 232.3 |
| 贴现率5% | 7 638.7 | 16 482.3 | 4 387.5 |
| 总经济负担(万元) | |||
| 贴现率为3% | 14 858.6 | 31 896.7 | 8 510.4 |
| 贴现率为0 | 44 409.7 | 94 966.5 | 25 426.0 |
| 贴现率5% | 8 005.4 | 17 220.0 | 4 581.2 |
2013—2015年手足口病死亡病例的人均社会经济损失在56.5万~97.0万元之间,手足口病患者死亡给家庭带来精神打击的同时,也给其家庭乃至整个社会带来沉重的经济损失。早亡损失约占死亡病例社会经济负担总额的97%以上,是死亡病例经济损失的最重要的组成部分。2013—2015年我国手足口病死亡病例总经济负担为1.45亿~3.12亿元,占传染病和寄生虫病的早亡损失的1.4%~3.1%[10]。2016年一项针对EV71型疫苗卫生经济学评价的研究显示,因手足口病轻症及重症病例数远超过手足口病死亡病例,手足口病死亡病例经济负担仅占全部手足口病疾病负担的40.0%[16]。若同时考虑全国轻症、重症及死亡病例时,手足口病的社会经济负担将更为沉重。
由于全国手足口病死亡病例数相对较小且在全国分布较为分散,针对死亡病例的社会经济负担研究较少。2011年宁波市的一项研究显示[6],6例手足口病死亡病例的社会经济损失合计为1 452.6万元,但该研究并未考虑贴现率对收入现值的影响,因此其结果可能存在高估。本研究首次对2013—2015年全国人均手足病死亡病例的早亡损失及社会经济损失进行估计,估计时综合考虑了各个年龄组的劳动参与率以及贴现率,并从各个年龄组展示了手足口病死亡病例的早亡损失。此外,研究进一步对全国手足口病死亡病例的社会经济负担进行了评估,为全面了解该病所致死亡的社会经济影响提供了科学依据。本研究仍存在一定局限:(1) 在推算2014—2015年经济负担时,采用的是医疗部门消费价格指数进行校正,可能未反映经济负担中直接非医疗费用和间接费用的增长水平。(2) 死亡病例的离世对其家属将造成极大的精神打击,死者家属平复情绪期间也会带来一定的生产力下降,本研究并未考虑在内。(3) 临床治疗中部分手足口病死亡病例在救治过程中由于治疗无效或经济因素家庭放弃治疗,患者并未在医院死亡因而并未上报到全国法定传染病报告系统中,因而可能造成总经济负担的低估。(4) 本研究采用的全部数据均为全国数据,而各省级经济发展水平不同,因此本研究结果可能仅能反映全国平均水平,不能反映省级水平的手足口病社会经济负担。
如何有效地预防手足口病是降低手足口病死亡率以及降低社会经济负担的关键。2015年12月,全球首支针对手足口病的灭活肠道病毒EV71型疫苗在我国批准上市。EV71是引起手足口病重症及死亡的主要病原,提高该疫苗在适龄儿童中的接种率,是预防手足口病重症及死亡最有效的手段。然而,目前该疫苗在我国仍属二类疫苗,其供应量尚不能满足全部适龄儿童的需求且价格较高。因此如何提高该疫苗的可及性,让更多的儿童能够接种该疫苗,形成有效的群体免疫,是我国卫生主管部门及疫苗产业界目前亟需解决的问题。
作者贡献:
ORCID:0000-0003-0728-175X
郑亚明:构思该文章,数据分析、稿件撰写、修改
杨娟:文章构思及文章审阅
| [1] |
Luo L, Xing WJ, Liao QH, et al.
Research progress on seroepidemiological study of enterovirus 71 and coxsackievirus A16 infection among children[J].
Chinese Journal of Preventive Medicine, 2015, 49(2): 184–188.
(in Chinese) 罗莉, 邢薇佳, 廖巧红, 等. 儿童肠道病毒71型和柯萨奇病毒A16型感染血清流行病学研究进展[J]. 中华预防医学杂志, 2015, 49(2): 184–188. |
| [2] |
Li XL, Li Y, Zhang BF, et al.
Etiology study on severe cases caused by hand, foot and mouth disease in children from Henan province, 2014[J].
Chinese Journal of Epidemiology, 2016, 37(4): 568–571.
(in Chinese) 李幸乐, 李懿, 张白帆, 等. 河南省2014年手足口病重症病例病原学分析[J]. 中华流行病学杂志, 2016, 37(4): 568–571. DOI:10.3760/cma.j.issn.0254-6450.2016.04.026 |
| [3] |
Zha J, Feng Q, Ma ZL.
The pathogenic spectrum of the enteroviruses for non-EV71 and Cox A16 for HFMD in Taizhou between 2010 and 2013 and the VP1 gene character analysis for Coxsackievirus A6[J].
Chinese Journal of Epidemiology, 2014, 35(10): 1181–1182.
(in Chinese) 查杰, 封琦, 马智龙. 2010-2013年江苏省泰州市非EV71和非Cox A16型手足口病肠道病毒病原谱及Cox A6 VP1基因特征分析[J]. 中华流行病学杂志, 2014, 35(10): 1181–1182. |
| [4] | Solomon T, Lewthwaite P, Perera D, et al. Virology, epidemiology, pathogenesis, and control of enterovirus 71[J]. Lancet Infect Dis, 2010, 10(11): 778–790. DOI:10.1016/S1473-3099(10)70194-8 |
| [5] |
National health and family planning commission. National notifiable infectious disease report[EB/OL]. (2016-05-01)[2017-04-01]. http://www.moh.gov.cn/jkj/. (in Chinese)
中华人民共和国国家卫生与计划生育委员会. 全国法定传染病疫情概况[EB/OL]. (2016-05-01)[2017-04-01]. http://www.moh.gov.cn/jkj/. |
| [6] |
Yang TC, Yi B, He TF, et al.
economic burden of hand, foot and mouth disease in Ningbo, Zhejiang[J].
Disease Surveillance, 2012, 27(7): 520–523.
(in Chinese) 杨天池, 易波, 贺天峰, 等. 浙江省宁波市手足口病经济负担调查研究[J]. 疾病监测, 2012, 27(7): 520–523. |
| [7] | Gan ZK, Jin H, Li JX, et al. Disease burden of enterovirus 71 in rural central China:a community-based survey[J]. Hum Vaccin Immunother, 2015, 11(10): 2400–2405. DOI:10.1080/21645515.2015.1059980 |
| [8] | Wang ZL, Xia AM, Li YF, et al. Socioeconomic burden of hand, foot and mouth disease in children in Shanghai, China[J]. Epidemiol Infect, 2016, 144(1): 138–143. DOI:10.1017/S0950268815001569 |
| [9] | Zheng YM, Jit M, Wu J, et al. Economic costs and health-related quality of life for hand, foot and mouth disease (HFMD) patients in China[J]. PLoS One, in peer review. |
| [10] |
Yang J, Feng LZ, Zheng YM, et al.
Estimation on the indirect economic burden of disease related premature deaths in China, 2012[J].
Chinese Journal of Epidemiology, 2014, 35(11): 1256–1262.
(in Chinese) 杨娟, 冯录召, 郑亚明, 等. 中国2012年疾病相关过早死亡的间接经济负担估计[J]. 中华流行病学杂志, 2014, 35(11): 1256–1262. |
| [11] | World Health Organization. Life tables by country[DB/OL]. (2016-06-15)[2017-03-27].http://apps.who.int/gho/data/view.main.60340?lang=en. |
| [12] |
Population census office under the state council & department of population and employment statistics national bureau of statistics of China, employment statistics national bureau of statistics of China. Tabulation on the 2010 population census of the people' republic of China[R/OL]. (2017-03-21)[2017-04-02].http://www.stats.gov.cn/tjsj/pcsj/rkpc/6rp/left.htm. (in Chinese)
国务院人口普查办公室, 国家统计局人口和就业统计司.中国2010年人口普查资料[R/OL]. (2017-03-21)[2017-04-02].http://www.stats.gov.cn/tjsj/pcsj/rkpc/6rp/left.htm. |
| [13] |
National bureau of statistics of China. Annual data[EB/OL]. (2017-03-15)[2017-03-27]. http://data.stats.gov.cn/easyquery.htm?cn=C01. (in Chinese)
中华人民共和国国家统计局. 年度数据[EB/OL]. (2017-03-15)[2017-03-27]. http://data.stats.gov.cn/easyquery.htm?cn=C01. |
| [14] |
National bureau of statistics of China. Statistical communique on national economic and social development, 2014[EB/OL]. (2015-02-26)[2017-03-27]. http://www.stats.gov.cn/tjsj/zxfb/201502/t20150226_685799.html. (in Chinese)
中华人民共和国国家统计局. 2014年国民经济和社会发展统计公报[EB/OL]. (2015-02-26)[2017-03-27]. http://www.stats.gov.cn/tjsj/zxfb/201502/t20150226_685799.html. |
| [15] |
National bureau of statistics of China. Statistical communique on national economic and social development, 2015[EB/OL]. (2016-02-29)[2017-03-27]. http://www.stats.gov.cn/tjsj/zxfb/201602/t20160229_1323991.html. (in Chinese)
中华人民共和国国家统计局. 2015年国民经济和社会发展统计公报[EB/OL]. (2016-02-29)[2017-03-27]. http://www.stats.gov.cn/tjsj/zxfb/201602/t20160229_1323991.html. |
| [16] | Wu JT, Jit M, Zheng YM, et al. Routine pediatric enterovirus 71 vaccination in China:a cost-effectiveness analysis[J]. PLoS Med, 2016, 13(3): e1001975. DOI:10.1371/journal.pmed.1001975 |